J Korean Soc Radiol 2017;76(1):14-24 https://doi.org/10.3348/jksr.2017.76.1.14
INTRODUCTION
In nonalcoholic fatty liver disease (NAFLD), excess liver fat (more than 5%) can accumulate in a patient without a history of alcohol abuse (1). It affects 20–40% of individuals in Western countries and 5–40% of the general population across the Asia- Pacific area (2, 3). The rising prevalence of NAFLD including
nonalcoholic steatohepatitis is in parallel with that of obesity, type 2 diabetes, and metabolic syndrome (4). Ten to 29% of pa- tients with nonalcoholic steatohepatitis may develop liver cir- rhosis within 10 years and 4–27% of these patients may develop hepatocellular carcinoma (5). Fatty liver is a risk factor for pri- mary dysfunction in donors and recipients after liver transplan- tation (6).
Comparative Study of Ultrasonography, Computed Tomography, Magnetic Resonance Imaging, and Magnetic Resonance
Spectroscopy for the Diagnosis of Fatty Liver in a Rat Model
쥐를 이용한 지방간 실험모델에서 초음파, 전산화단층촬영, 자기공명영상, 자기공명분광술의 진단에 대한 비교연구
Hoon Noh, MD
1, Xiao-li Song, MD
1, Suk Hee Heo, MD
1, Jin Woong Kim, MD
1,
Sang Soo Shin, MD
2, Kyu Youn Ahn, MD
3, Yong Yeon Jeong, MD
1, Heoung-Keun Kang, MD
1*
1Department of Radiology, Chonnam National University Hwasun Hospital, Hwasun, Korea
2Department of Radiology, Chonnam National University Hospital, Gwangju, Korea
3Department of Anatomy, Chonnam National University Medical School, Gwangju, Korea
Purpose: To compare the accuracy of ultrasonography (US), single-energy CT (SECT), dual-energy CT (DECT), MR imaging (MRI), and MR spectroscopy (MRS) for detect- ing fatty liver in a rat model.
Materials and Methods: Fatty liver was induced by 60% high-fat diet for 1, 2, 3, 4, or 5 weeks (3 rats per group, a total of 15 rats). The control group comprised of five rats fed 10% high-fat diet. US, SECT, DECT, MRI, and MRS of the liver were per- formed weekly. Histologic steatosis grade and intrahepatocelluar triglyceride level were determined histologically for the livers of sacrificed rats. Pearson correlation test was used to assess the correlation between examinations and standard refer- ence levels. Receiver operating characteristic curves were constructed. Area under the curve (AUC), sensitivity, and specificity were calculated.
Results: US, SECT, DECT, MRI, and MRS were significantly correlated with histologic steatosis grade. The diagnostic performance of AUC, sensitivity, and specificity were 0.893, 80%, and 80% for US, 0.960, 80%, and 80% for SECT, 0.947, 100%, and 60%
for DECT, 0.933, 93.3%, and 100% for MRI, and 0.960, 93.3%, and 100% for MRS.
Conclusion: MRS showed the strongest correlation with histologic steatosis grade with the highest sensitivity and specificity for diagnosis of fatty liver compared to other modalities.
Index terms Rats Fatty Liver Ultrasound
Computed Tomography Magnetic Resonance Imaging Spectroscopy
Received May 23, 2016 Revised July 4, 2016 Accepted July 11, 2016
*Corresponding author: Heoung-Keun Kang, MD Department of Radiology, Chonnam National University Hwasun Hospital, 322 Seoyang-ro, Hwasun-eup, Hwasun 58128, Korea.
Tel. 82-61-379-7101 Fax. 82-62-226-4380 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
Liver biopsy is the “gold standard” for quantifying a fatty liv- er. However, this procedure can provoke pain, bleeding, and other severe complications. Furthermore, sample error induced by uneven fatty distribution can affect the accuracy of measure- ments (1, 7, 8). A noninvasive method that is accurate, cost-effec- tive, and convenient is very important for evaluating NAFLD in clinical field.
Compared to biopsy, imaging studies such as ultrasonogra- phy (US), computed tomography (CT), and magnetic resonance imaging (MRI) are more commonly applied in clinical practice (9-11). US is a cost-effective imaging technique that is widely available. However, it is limited by observer variability. It is not an accurate technique for assessing fatty liver (12). CT is reli- able for assessing moderate or severe hepatic steatosis. Howev- er, it has unignorable limitation in radiation exposure (13, 14).
Multiecho Dixon MRI and MR spectroscopy (MRS) shows ex- cellent performance in fatty liver quantification with strong correlation with histopathological evaluation for liver biopsies in NAFLD (15). However, its high expense, demands for hold- breath, and requirement of special technique restrict its large- scale application.
Several studies have used US, CT, and MRI to evaluate a fatty liver (9-11, 13-32). Some studies have compared two or three imaging modalities for the diagnosis of a fatty liver (13, 18, 29, 30, 32, 33). To the best of our knowledge, there is no study that has compared all imaging modalities [i.e., US, single-energy CT (SECT), dual-energy CT (DECT), MRI, and MRS]. Therefore, the objective of this study was to compare different imaging mo- dalities (i.e., US, SECT, DECT, multiecho MRI, and high-speed T2-corrected multiecho proton MRS) for the diagnosis of fatty liver induced by a high-fat diet in a rat model.
MATERIALS AND METHODS
Animal Model
Twenty male 8-week-old Sprague-Dawley rats (280–320 g) were used in this study. The experimental study was approved by the governmental committee and Institutional Animal Research Review Board of Chonnam National University Hwasun Hospital.
Rats were housed in a controlled environment (12 hr/12 hr, light/dark cycle) with free access to water and food. Fatty liver was induced by two different high-fat diets (D12450B and
D12492; Research Diets, Inc., New Brunswick, NJ, USA) to ob- tain a wider range of nonfatty livers. Fifteen rats received a 60%
high-fat diet for 1, 2, 3, 4, or 5 weeks (i.e., fatty liver group). Five rats received a 10% high-fat diet (i.e., nonfatty liver group or con- trol group).
US Examination
US, CT, and MR examination were performed on the same day. Rats were intraperitoneally anesthetized with 2% sodium pentobarbital (40 mg/kg). Their abdomens were shaved to reduce imaging artifacts during US examination. US was performed with Philips iU22 ultrasound equipment (Philips Healthcare, Eind- hoven, the Netherlands) with a 15 MHz linear transducer (L15- 7io) by one experienced radiologist who was blinded to other study results. All images were obtained in fundamental bright- ness mode (B-mode). Two-dimensional B-mode image plans were acquired with optimized gain and time gain compensation settings which remained constant throughout the experiment.
The acoustic focus was the center of the liver. To estimate the so- nographic hepatorenal index (HRI), US images of the liver and right kidney were obtained in sagittal liver/right kidney view at supine position.
US imaging data were transmitted to a picture archiving and communication system (PACS, Maroview 5.4; Infinitt, Seoul, Korea). From the sagittal liver/right kidney view of US, a 1-cm2 circular region of interest (ROI) was selected for hepatic paren- chyma uniformly after excluding blood vessels, bile ducts, and other focal hypo- or hyperechogenicity. A ROI of 0.3–0.5 cm2 was selected for the right renal cortex excluding the large ves- sels, sinus, and medulla. The liver and right kidney ROIs were se- lected at the same depth. The mean gray-scale value of the pixels in each ROI was used to determine its echogenicity. HRI (i.e., the ratio of the echogenicity of the liver to the echogenicity of the right kidney parenchyma) was calculated (17).
CT Examination
SECT and DECT were performed on Somatom Definition FLASH equipment (Siemens Medical Systems, Forchheim, Ger- many). The CT scanner has two X-ray tubes and corresponding detectors at an angular offset of 90° within the same gantry. Tube potentials were typically set at 140 kVp for tube A and 80 kVp for tube B. This configuration allowed imaging of the same
voxel at the same time in two different X-ray spectra.
After acquiring a lateral and anterior-posterior topogram, the scan range covered the whole liver in the z-axis extension. Rats were carefully placed in the isocenter of the scanner. The pa- rameters for SECT and DECT scanning are shown in Table 1.
All images were processed with a dedicated medium-soft con- volution kernel (D30f) in the abdominal window [level 50 Hounsfield units (HU), width 450 HU] with slice thickness of a 1.5-mm.
In SECT and DECT, data were processed by a research fellow under direct supervision of an experienced abdominal radiolo- gist (30 years of experience). The research fellow was blinded to study results. Five ROIs were selected in the liver and one ROI was selected in the spleen. The area of the ROI was 0.5–1.0 cm2. Hepatic fat content was measured by using mean liver attenua- tion of all ROIs in the liver (34). The mean HU of the right lobe of the liver and spleen was obtained. Differences between the HU of liver and spleen (HUS) were calculated (Fig. 2). On DECT images, the HU values of liver at 140 kVp and 80 kVp were obtained and the difference between HU of 140 kVp and 80 kVp (HUD) was calculated. The anatomic level, position, set form, and dimension of every ROI were matched those of SECT and DECT images. Difference in HU was calculated (14, 25).
MRI and MRS Examination
Rats anesthetized by isoflurane (2.5% isoflurane in air, 1 L/
min) were fixed in supine position. They were allowed to breathe freely. All rats were scanned with a 3.0 T clinical MR scanner (Magnetom Skyra, Siemens Medical Systems, Forchheim, Ger- many) with knee coil.
For MRI, multiecho MRI was performed using the work in progress (WIP) software package by Siemens Medical System.
Multisection axial images were obtained by using a two-dimen-
sional spoiled gradient echo sequence with all array coil elements.
To minimize T1 effects, a low flip angle (4°) was used at a repe- tition time of 8.83 ms. To estimate fat-water signal interference and T2* effects, six echoes were obtained at a serial of opposed- phase (OP) and in-phase (IP) echo times (1.23, 2.46, 3.69, 4.92, 6.15, and 7.38 ms). Other imaging parameters were: section thickness of 2 mm, 100% intersection gap, 1090 Hz/pixel receiv- er bandwidth, one signal acquired, and rectangular field of view with a 78 × 96 matrix. We used a 10 × 10 × 10 mm voxel for MRI to measure the signal intensity on OP and IP images. T2*
map, water image, fat image, and fat fraction (FF) map were de- rived from the multiecho-spoiled gradient echo sequence by using pixel-by-pixel image calculations for each section.
For MRS, high-speed T2-corrected multiecho proton MRS technique was also used using the WIP of Siemens Medical System. A single 10 × 10 × 10 mm voxel was placed in a right hepatic segment while avoiding vascular and biliary structures.
After shimming, stimulated echo acquisition mode single voxel proton spectroscopy was performed. The repetition time was 3000 ms to minimize T1 effects. To estimate T2, five single-aver- age spectra were collected at echo times of 12, 24, 36, 48, and 72 ms with 1200 Hz receiver bandwidth and 2048-point spectral resolution. Fat signal fraction (%) was determined with MRS.
Data were processed by a research fellow under direct super- vision of an experienced abdominal radiologist and MR physi- cist (10 years of experience) who was blinded to the study results.
FF of the liver was obtained from MRI images. One radiologist reviewed the image by manually placing a circular ROI of ap- proximately 0.5–1.0 cm2, the same area used in MRS (excluding blood vessels, bile ducts structures). The FF from MRS was au- tomatically propagated to PACS.
Histopathologic Examinations
All rats were sacrificed for histopathological and biochemical assessment of the liver. Five samples of the right lateral lobe were excised from all livers. Sample sizes were similar (100–150 mg).
Each specimen was frozen at -80°C and stained with hematoxy- lin-eosin with original magnification of × 400. No separate stain- ing for iron was performed. Fibrosis was not assessed. Grading of the fatty liver was based on quantitative evaluation of the per- centage of hepatocytes containing macrovesicular fat (0–100%) using image analysis software (iSolution FL/Auto, Burnaby, Cana- Table 1. Scanning Parameters of SECT and DECT
SECT DECT
Tube voltage (kVp) 120 140/80
mAs 100 100/425
FOV (cm) 90 90
Pitch 0.55 0.55
Rotation time (sec) 0.5 0.5
Collimation (mm) 120 × 0.6 32 × 0.6
DECT = dual-energy computed tomography, FOV = field of view, SECT = single-energy computed tomography
da). Grading results were expressed as the percentage of cells af- fected by a fatty liver as follows: “none” (≤ 5%), “mild” (> 5%
but < 33%), “moderate” (≥ 33% but < 66), and “severe” (≥ 66%) (Fig. 3) (35). For hepatic triglyceride (TG), approximately 100 mg of rat liver tissue samples were homogenized in 2 mL of chloroform-methanol solution (2:1 v/v) followed by centrifuga-
tion at 3000 rpm for 10 minute. Hepatic TG value was acquired by TG colorimetric assay kit (10010301; Cayman Chemical, Ann Arbor, MI, USA) on a plate reader (Infinite M200 PRO, Tecan, Männedorf, Switzerland).
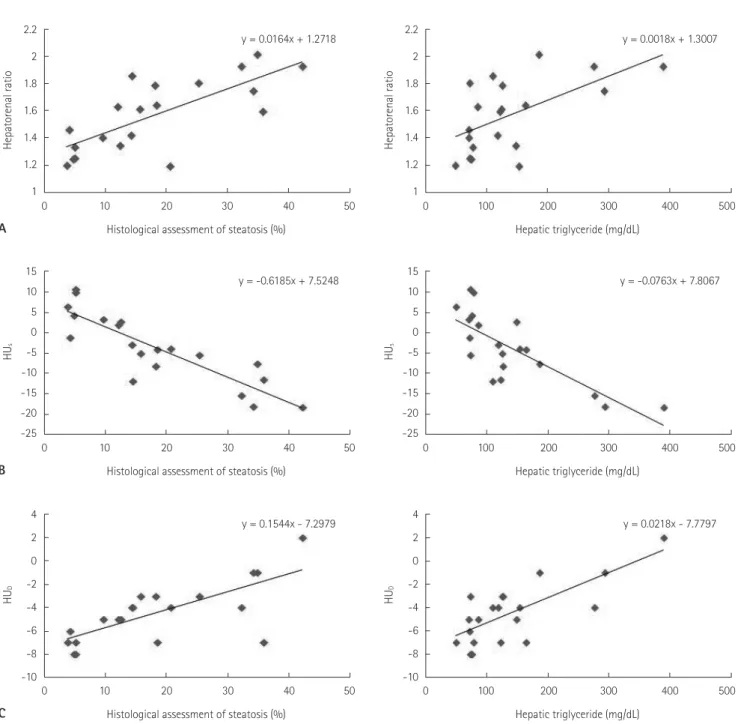
Fig. 1. Scatterplots and regression lines showing correlations between histopathologic results (percentage steatosis) or intra-hepatocellular TG with the degree of fatty liver at US (A), SECT (B), DECT (C), MRI (D), and MRS (E).
DECT = dual-energy computed tomography, HUD = the difference between Hounsfield units of 140 kVp and 80 kVp, HUS = difference in Houn- sfield units between the liver and spleen, MRI = magnetic resonance imaging, MRS = magnetic resonance spectroscopy, SECT = single-energy computed tomography, US = ultrasonography
2.2 2 1.8 1.6 1.4 1.2 1
2.2 2 1.8 1.6 1.4 1.2 1
0 10 20 0 100 200
Histological assessment of steatosis (%) Hepatic triglyceride (mg/dL)
30 40 300 400
y = 0.0164x + 1.2718 y = 0.0018x + 1.3007
50 500
Hepatorenal ratio Hepatorenal ratio
A
15 10 5 0 -5 -10 -15 -20 -25
15 10 5 0 -5 -10 -15 -20 -25
0 10 20 0 100 200
Histological assessment of steatosis (%) Hepatic triglyceride (mg/dL)
30 40 300 400
y = -0.6185x + 7.5248 y = -0.0763x + 7.8067
50 500
HUs HUs
B
4 2 0 -2 -4 -6 -8 -10
4 2 0 -2 -4 -6 -8 -10
0 10 20 0 100 200
Histological assessment of steatosis (%) Hepatic triglyceride (mg/dL)
30 40 300 400
y = 0.1544x - 7.2979 y = 0.0218x - 7.7797
50 500
HUD HUD
C
Statistical Analysis
Statistical analysis was performed using SPSS v.16.0 software (IBM, Chicago, IL, USA). Means ± standard deviations were calculated for descriptive data. A two-sample t test was used to compare two independent mean values. Pearson correlation test was used to assess the linear correlation among histologic ste- atosis grade, intra-hepatocellular TG content, HRI of US, HUS
of SECT, HUD of DECT, and FF of MRI and MRS. A coefficient of 0.25 or less was considered as “low” correlation. A coefficient of 0.26–0.50 was considered as “fair” correlation. A coefficient of 0.51–0.75 was considered as “good” correlation. A coefficient of greater than 0.75 was considered as “excellent” correlation. Re- ceiver operating characteristic (ROC) curves were created. Op- timal cut-off points were estimated for the diagnosis of a fatty liver (> 5%). Sensitivity and specificity were estimated for the diagnosis of fatty liver. A p value of less than 0.05 was consid- ered as statistically significant. All tests were two-tailed.
RESULTS
Histopathologic Examination of the Rat Model
Based on histopathologic examination, five rats had no fatty liver, 10 rats had mild fatty liver, and five rats had moderate fat- ty liver. Of the five rats with nonfatty liver, three were fed the 60%
high-fat diet and two were fed the 10% high-fat diet (Table 2).
US Examination
There was no significant (p = 0.736) difference in renal echo- genicity between the two groups (Table 3). However, hepatic echo- genicity in the fatty liver group was significantly (p = 0.036) high- er than that in the nonfatty liver group. The mean HRI value in the fatty liver group was significantly (p = 0.004) higher than that in the nonfatty liver group.
25
20 15
10
5 0
25
20 15
10
5 0
D
0 10 20 0 100 200
Histological assessment of steatosis (%) Hepatic triglyceride (mg/dL)
30 40 300 400
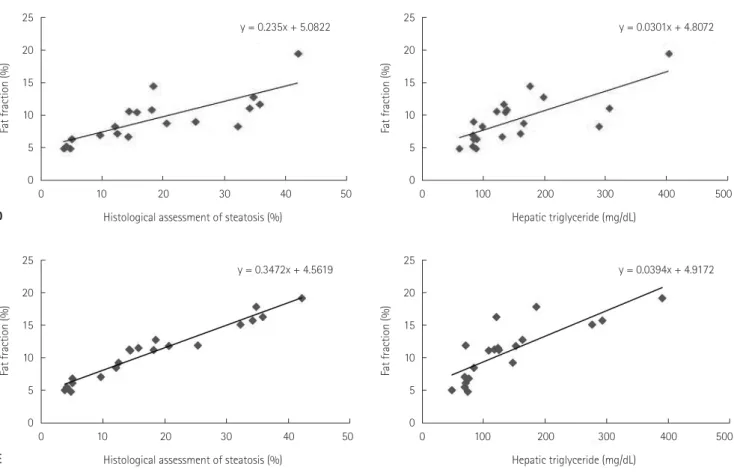
y = 0.235x + 5.0822 y = 0.0301x + 4.8072
50 500
Fat fraction (%) Fat fraction (%)
25 20
15 10
5 0
25 20
15 10
5 0
E
0 10 20 0 100 200
Histological assessment of steatosis (%) Hepatic triglyceride (mg/dL)
30 40 300 400
y = 0.3472x + 4.5619 y = 0.0394x + 4.9172
50 500
Fat fraction (%) Fat fraction (%)
Fig. 1. Scatterplots and regression lines showing correlations between histopathologic results (percentage steatosis) or intra-hepatocellular TG with the degree of fatty liver at US (A), SECT (B), DECT (C), MRI (D), and MRS (E).
DECT = dual-energy computed tomography, HUD = the difference between Hounsfield units of 140 kVp and 80 kVp, HUS = difference in Houn- sfield units between the liver and spleen, MRI = magnetic resonance imaging, MRS = magnetic resonance spectroscopy, SECT = single-energy computed tomography, US = ultrasonography
CT Examination
On SECT, the mean attenuation value of the liver in the fatty liver group was significantly (p = 0.001) lower than that in the nonfatty liver group. The mean value of HUS in the fatty liver group was significantly (p = 0.001) lower than that in the non- fatty liver group (Table 3). On DECT, the difference between HU of 140 kVp and 80 kVp was significant (p = 0.009). The mean val- ue of hepatic HU in the fatty liver group was significantly (p = 0.004) lower than that in the nonfatty liver group.
MRI and MRS
On MRI, the mean values of liver FF measured in the nonfatty liver group and the fatty liver group were 5.7 ± 0.8% and 11.2 ± 3.7%, respectively (p = 0.005). MRS showed that the mean FF values of the nonfatty liver group and fatty liver group were 4.9 ± 0.6%, and 12.1 ± 4.0%, respectively (p = 0.001) (Table 3).
Correlations
Results of correlation between imaging techniques and histo- pathologic examination are summarized in Table 4. Fig. 1 graphi- cally shows these correlations. The US findings showed good correlation with histologic steatosis grades (r = 0.744, p < 0.001) and TG levels (r = 0.588, p = 0.006). The SECT, DECT, MRI, and MRS findings had excellent correlation with histologic steatosis grades (r = -0.867, 0.775, 0.869, and 0.916, respectively) and TG levels (r = -0.780, 0.765, 0.767, and 0.910, respectively). The MRS showed a higher correlation with histologic steatosis grades and TG levels compared to other examinations.
Diagnostic Accuracy
The diagnostic performance in the diagnosis of fatty liver was calculated for the five imaging modalities. Results are summa- rized in Table 5. We performed ROC curve fitting for US, SECT, DECT, MRI, and MRS. From the ROC curves, we determined the cut-off value for each imaging modality. These cut-off val- ues were used to calculate diagnostic accuracy (Table 5). MRS and SECT had the highest AUC (0.960), indicating the best ac- ceptable diagnostic performance. The AUC of US was the low- est (0.893). The AUC was 0.947 for DECT and 0.933 for MRI.
DECT had the highest sensitivity (100%) while US and SECT had the lowest sensitivity (80%). Specificity was the highest for MRI and MRS (100%) but the lowest for DECT (60%).
DISCUSSION
Our study evaluated five up-to-date imaging modalities for the diagnosis of fatty liver in rat model. Our results demonstrat- ed that MRS had higher correlation with histopathologic find- ings and yielded greater diagnostic accuracy for the diagnosis of fatty liver than other modalities. MRI and MRS allowed ob- jective assessment of fatty liver with the highest specificity.
In our study, the diagnostic performance of US was relatively Fig. 2. Transverse single energy computed tomographic image at 120
kVp of a rat showing the gate of the liver and the mean position of the region of interest at liver and spleen.
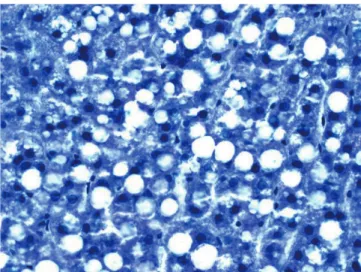
Fig. 3. Typical histologic slides of liver section from 60% high-fat diet of the rats for three weeks with approximately 30% steatosis. The fat content of the drop-shaped observation showed no signs of inflam- mation or fibrosis findings (hematoxylin-eosin stain, × 400).
Table 2. The Number of Fatty Livers after High-Fat Diet in Rats
High-Fat Diet Normal Mild Moderate
60% (n = 15) 3 7 5
10% (n = 5) 2 3 0
Total (n = 20) 5 10 5
lower than that of other imaging modalities. The cut-off HRI value of 1.33 on US had relatively low sensitivity and specificity (both 80%). Previous studies have reported a wide range of HRI for predicting a hepatic steatosis grade greater than 5% (17, 23, 24), suggesting that HRI is useful for screening fatty liver. How- ever, it is based on subjective impression of “bright liver echo”
pattern (36-38). Although US is a cost-effective imaging tech- nique for the diagnosis of fatty liver in clinical practice, poor echoic screening can affect the accuracy of fatty liver quantifica- tion (12).
SECT and DECT showed stronger correlation with the refer- ence standard and yielded higher diagnostic accuracy than US
in our study. The cut-off HUS value of 0 HU on SECT showed sensitivity and specificity of 80% each. Previously, a threshold cut-off HUS value of 3.2 has a sensitivity of 72.7% and a speci- ficity of 91.3% (26), and a threshold cut-off HU value of -9 has a sensitivity of 82% and a specificity of 100% in detecting mod- erate degree of fatty liver (25). We found similar sensitivity.
However, the specificity in this study was relatively lower than those in previous studies due to the relatively lower cut-off val- ue used in this study.
DECT scanners require less effort because two image datas- ets are acquired in the same anatomic location with two differ- ent X-ray spectra which allow the analysis of energy-dependent changes in the attenuation of different materials from soft tissues (13). When scanned with different energy (140 and 80 kVp), fat- ty livers have shown greater changes in attenuation than nor- mal livers (21). In our study, the ability of DECT to quantify a fatty liver and using a threshold cut-off HUD value of 2.5 for di- agnosing fatty liver had a high sensitivity (100%) but relatively low specificity (60%). However, the theoretical advantage of DECT has not yet been established clinically. Similar to other studies (13, 39), the diagnostic performance of DECT was rela- tively lower than that of SECT in this study.
The threshold values of CT indices for the diagnosis of fatty liver also varied depending on the methods and populations used. Although the accuracy of CT in diagnosing fatty liver var- ied, CT was quite accurate for the diagnosis of moderate-to-se- vere fatty liver. However, CT was not as accurate for detecting mild fatty liver. Although its advantages include low cost, wide Table 3. Data Analysis of US, SECT, and DECT
Nonfatty Liver Group Fatty Liver Group p-Value
US
Liver 77.6 ± 15.1 101.4 ± 21.5 0.036
Kidney 59.6 ± 8.7 61.7 ± 12.9 0.736
HRI 1.3 ± 0.1 1.7 ± 0.2 0.004
SECT
Liver 69.1 ± 4.2 55.0 ± 7.9 0.001
HUs 6.1 ± 4.7 -6.9 ± 7.0 0.001
DECT
140 kVp 65.0 ± 3.3 59.6 ± 6.7 0.106
80 kVp 62.8 ± 2.3 53.5 ± 6.9 0.009
HUD 2.2 ± 1.3 6.1 ± 2.5 0.004
DECT = HUD on dual-energy computed tomography, HRI = hepatorenal index, HUD = difference in Hounsfield units between 140 kVp and 80 kVp, HUS = difference in Hounsfield units between the liver and spleen, Kidney = gray-scale value of the kidney, Liver = gray-scale value of the liver, SECT = HUS on single-energy computed tomography, US = ultrasonography, 80 kVp = hepatic attenuation on 80 kVp, 140 kVp = hepatic attenuation on 140 kVp Table 4. Assessment of a Linear Correlation between Imaging Stud-
ies, Intra-Hepatocellular Triglyceride and Histologic Steatosis
Imaging Studies TG p-Value
Steatosis Grade
US 0.588 < 0.001
0.744 0.006
SECT -0.780 < 0.001
-0.867 < 0.001
DECT 0.765 < 0.001
0.775 < 0.005
MRI 0.767 < 0.001
0.869 < 0.001
MRS 0.910 < 0.001
0.916 < 0.001
DECT = dual-energy computed tomography, MRI = magnetic resonance imaging, MRS = magnetic resonance spectroscopy, SECT = single-energy computed tomography, Steatosis grade = r value of the histologic steatosis grade, TG = r value of the intra-hepatocellular triglyceride content obtained by histology, US = ultrasonography
not have severe fatty liver. Mild fatty liver was the most common kind. However, our results proved the diagnostic performance of these modalities for distinguishing normal liver from mild fatty livers. Second, we did not consider the effect of microve- sicular fatty liver on the diagnostic performance of these imaging techniques because macrovesicular fatty liver is clinically more relevant as a risk factor in liver surgery and transplantation (18).
Third, because small sample size was used, there was no statisti- cal comparison for imaging or spectroscopic values for sensitiv- ity and specificity. However, we performed ROC curve analysis to assess test accuracy. Fourth, the rat model used in our study may not accurately represent liver disease in humans. Since such testing is impossible in humans owing to the small size of biopsy sample to avoid substantial biohazards, an animal model en- abled more extensive and thorough testing than what is possible in humans. We used large sample sizes and tested the entire liv- er to represent a true mass FF across the entire liver.
In conclusion, compared to US, SECT, DECT, and MRI, MRS is a more precise modality with higher accuracy for evaluating a fatty liver in rat model. MRS is currently the most accurate im- aging method for diagnosing fatty liver, although both MRS and MRI are very reproducible and accurate in quantifying he- patic fat. They might replace liver biopsy.
REFERENCES
1. Krawczyk M, Bonfrate L, Portincasa P. Nonalcoholic fatty liver disease. Best Pract Res Clin Gastroenterol 2010;24:
695-708
2. Chitturi S, Farrell GC, George J. Non-alcoholic steatohepa- titis in the Asia-Pacific region: future shock? J Gastroen- terol Hepatol 2004;19:368-374
3. Farrell GC. Non-alcoholic steatohepatitis: what is it, and usage, and short examination time, it is impractical for routine
follow-up use due to radiation exposure. Another limitation of CT is its low accuracy for early-stage fatty liver compared to MR techniques (11). Moreover, its sensitivity and specificity will de- crease when diffuse iron deposition exists (25).
In our study, the correlation was stronger when MRI was used rather than US or CT. The sensitivity and specificity of MRI for detecting mild fatty liver have been reported to be 76.7–90.0%
and 87.1–91%, respectively, while those of MRS are 80.0–91.0%
and 80.2–87.0%, respectively (18, 26). Although the sensitivity and specificity of MRI and MRS in our study were similar to those reported earlier, MRS yielded higher diagnostic accuracy in this study. However, MRI is more practical than MRS as it can cover the entire liver. Technical optimization of MRS and MRI may result in more accurate and unbiased hepatic fat quantifica- tion (40).
MRS detected fatty liver with high sensitivity (93.3%) and specificity (100.0%) in this study. These values were higher for MRS in previous reports. The highest AUC value was 0.960 for both SECT and MRS. However, the correlation between SECT and histopathologic examination was significantly lower than that between MRS and histopathologic examination. Wu et al.
(16) have reported that MRS has high sensitivity (92.9%) and high specificity (82.6%) in detecting a fatty liver. Van Werven et al. (18) have found that MRS results are strongly correlated with histopathologic assessment and superior to US or SECT.
MRS is the best noninvasive technique for fatty liver detection.
It is increasingly replacing liver biopsy as the reference standard (10, 15, 20, 24). Multi-echo MRS techniques are typically per- formed within a single breath-hold with five single averaged spectra acquired at five different echo times. Our study used the same technique.
Our study had several limitations. First, our animal model did
Table 5. Diagnostic Performance of Imaging Studies in the Diagnosis of Fatty Liver (> 5%) as the Upper Normal Limit
AUC (95% CI) Cut-Off Value Sensitivity (%) Specificity (%)
US 0.893 (0.674–0.985) 1.33 80 80
SECT 0.960 (0.766–1.000) 0 HU 80 80
DECT 0.947 (0.746–0.998) 2.5 HU 100 60
MRI 0.933 (0.728–0.996) 6.88% 93.3 100
MRS 0.960 (0.766–1.000) 6.19% 93.3 100
AUC = area under curve, CI = confidence interval, DECT = difference between Hounsfield units of 140 kVp and 80 kVp on dual-energy computed tomogra- phy, MRI = fat fraction on magnetic resonance imaging, MRS = fat fraction on magnetic resonance spectroscopy, SECT = difference in Hounsfield units between the liver and spleen on single-energy computed tomography, US = hepatorenal index on ultrasonography
why is it important in the Asia-Pacific region? J Gastroen- terol Hepatol 2003;18:124-138
4. Starley BQ, Calcagno CJ, Harrison SA. Nonalcoholic fatty liver disease and hepatocellular carcinoma: a weighty con- nection. Hepatology 2010;51:1820-1832
5. Hsu CS, Kao JH. Non-alcoholic fatty liver disease: an emerg- ing liver disease in Taiwan. J Formos Med Assoc 2012;
111:527-535
6. Marcos A. Right lobe living donor liver transplantation: a review. Liver Transpl 2000;6:3-20
7. Piccinino F, Sagnelli E, Pasquale G, Giusti G. Complications following percutaneous liver biopsy. A multicentre retro- spective study on 68,276 biopsies. J Hepatol 1986;2:165- 173
8. Ratziu V, Charlotte F, Heurtier A, Gombert S, Giral P, Bruck- ert E, et al. Sampling variability of liver biopsy in nonalco- holic fatty liver disease. Gastroenterology 2005;128:1898- 1906
9. Schwenzer NF, Springer F, Schraml C, Stefan N, Machann J, Schick F. Non-invasive assessment and quantification of liver steatosis by ultrasound, computed tomography and magnetic resonance. J Hepatol 2009;51:433-445
10. Bohte AE, van Werven JR, Bipat S, Stoker J. The diagnostic accuracy of US, CT, MRI and 1H-MRS for the evaluation of hepatic steatosis compared with liver biopsy: a meta-anal- ysis. Eur Radiol 2011;21:87-97
11. Pickhardt PJ, Park SH, Hahn L, Lee SG, Bae KT, Yu ES. Spec- ificity of unenhanced CT for non-invasive diagnosis of he- patic steatosis: implications for the investigation of the natural history of incidental steatosis. Eur Radiol 2012;22:
1075-1082
12. Bohte AE, Koot BG, van der Baan-Slootweg OH, van Wer- ven JR, Bipat S, Nederveen AJ, et al. US cannot be used to predict the presence or severity of hepatic steatosis in se- verely obese adolescents. Radiology 2012;262:327-334 13. Artz NS, Hines CD, Brunner ST, Agni RM, Kühn JP, Roldan-
Alzate A, et al. Quantification of hepatic steatosis with dual-energy computed tomography: comparison with tis- sue reference standards and quantitative magnetic reso- nance imaging in the ob/ob mouse. Invest Radiol 2012;47:
603-610
14. Wang B, Gao Z, Zou Q, Li L. Quantitative diagnosis of fatty
liver with dual-energy CT. An experimental study in rab- bits. Acta Radiol 2003;44:92-97
15. van Werven JR, Marsman HA, Nederveen AJ, ten Kate FJ, van Gulik TM, Stoker J. Hepatic lipid composition analysis using 3.0-T MR spectroscopy in a steatotic rat model.
Magn Reson Imaging 2012;30:112-121
16. Wu CH, Ho MC, Jeng YM, Hsu CY, Liang PC, Hu RH, et al.
Quantification of hepatic steatosis: a comparison of the accuracy among multiple magnetic resonance techniques.
J Gastroenterol Hepatol 2014;29:807-813
17. Webb M, Yeshua H, Zelber-Sagi S, Santo E, Brazowski E, Halpern Z, et al. Diagnostic value of a computerized hepa- torenal index for sonographic quantification of liver ste- atosis. AJR Am J Roentgenol 2009;192:909-914
18. van Werven JR, Marsman HA, Nederveen AJ, Smits NJ, ten Kate FJ, van Gulik TM, et al. Assessment of hepatic steato- sis in patients undergoing liver resection: comparison of US, CT, T1-weighted dual-echo MR imaging, and point-re- solved 1H MR spectroscopy. Radiology 2010;256:159-168 19. Szczepaniak LS, Nurenberg P, Leonard D, Browning JD, Re-
ingold JS, Grundy S, et al. Magnetic resonance spectroscopy to measure hepatic triglyceride content: prevalence of he- patic steatosis in the general population. Am J Physiol En- docrinol Metab 2005;288:E462-E468
20. Pineda N, Sharma P, Xu Q, Hu X, Vos M, Martin DR. Mea- surement of hepatic lipid: high-speed T2-corrected multi- echo acquisition at 1H MR spectroscopy--a rapid and ac- curate technique. Radiology 2009;252:568-576
21. Patel BN, Kumbla RA, Berland LL, Fineberg NS, Morgan DE.
Material density hepatic steatosis quantification on intra- venous contrast-enhanced rapid kilovolt (peak)-switching single-source dual-energy computed tomography. J Com- put Assist Tomogr 2013;37:904-910
22. Park SH, Kim PN, Kim KW, Lee SW, Yoon SE, Park SW, et al.
Macrovesicular hepatic steatosis in living liver donors: use of CT for quantitative and qualitative assessment. Radiol- ogy 2006;239:105-112
23. Martín-Rodríguez JL, Arrebola JP, Jiménez-Moleón JJ, Olea N, González-Calvin JL. Sonographic quantification of a hepato-renal index for the assessment of hepatic steatosis in comparison with 3T proton magnetic resonance spec- troscopy. Eur J Gastroenterol Hepatol 2014;26:88-94
24. Mancini M, Prinster A, Annuzzi G, Liuzzi R, Giacco R, Med- agli C, et al. Sonographic hepatic-renal ratio as indicator of hepatic steatosis: comparison with (1)H magnetic reso- nance spectroscopy. Metabolism 2009;58:1724-1730 25. Lee SW, Park SH, Kim KW, Choi EK, Shin YM, Kim PN, et al.
Unenhanced CT for assessment of macrovesicular hepatic steatosis in living liver donors: comparison of visual grading with liver attenuation index. Radiology 2007;244:479-485 26. Lee SS, Park SH, Kim HJ, Kim SY, Kim MY, Kim DY, et al.
Non-invasive assessment of hepatic steatosis: prospective comparison of the accuracy of imaging examinations. J Hep- atol 2010;52:579-585
27. Lee SS, Lee Y, Kim N, Kim SW, Byun JH, Park SH, et al. He- patic fat quantification using chemical shift MR imaging and MR spectroscopy in the presence of hepatic iron depo- sition: validation in phantoms and in patients with chronic liver disease. J Magn Reson Imaging 2011;33:1390-1398 28. Hines CD, Yu H, Shimakawa A, McKenzie CA, Warner TF,
Brittain JH, et al. Quantification of hepatic steatosis with 3-T MR imaging: validation in ob/ob mice. Radiology 2010;
254:119-128
29. Cowin GJ, Jonsson JR, Bauer JD, Ash S, Ali A, Osland EJ, et al. Magnetic resonance imaging and spectroscopy for monitoring liver steatosis. J Magn Reson Imaging 2008;28:
937-945
30. Qayyum A, Chen DM, Breiman RS, Westphalen AC, Yeh BM, Jones KD, et al. Evaluation of diffuse liver steatosis by ultrasound, computed tomography, and magnetic reso- nance imaging: which modality is best? Clin Imaging 2009;
33:110-115
31. Yoshimitsu K, Kuroda Y, Nakamuta M, Taketomi A, Irie H, Tajima T, et al. Noninvasive estimation of hepatic steatosis using plain CT vs. chemical-shift MR imaging: significance for living donors. J Magn Reson Imaging 2008;28:678-684 32. Fishbein M, Castro F, Cheruku S, Jain S, Webb B, Gleason T,
et al. Hepatic MRI for fat quantitation: its relationship to fat morphology, diagnosis, and ultrasound. J Clin Gastro- enterol 2005;39:619-625
33. Korkusuz H, Keese D, Raschidi BA, Hübner F, Namgaladze D, Hintereder G, et al. Detection of a fatty liver after binge drinking: correlation of MR-spectroscopy, DECT, biochem- istry and histology in a rat model. Acad Radiol 2011;18:
1349-1357
34. Kodama Y, Ng CS, Wu TT, Ayers GD, Curley SA, Abdalla EK, et al. Comparison of CT methods for determining the fat content of the liver. AJR Am J Roentgenol 2007;188:1307- 1312
35. Kleiner DE, Brunt EM, Van Natta M, Behling C, Contos MJ, Cummings OW, et al. Design and validation of a histologi- cal scoring system for nonalcoholic fatty liver disease.
Hepatology 2005;41:1313-1321
36. Strauss S, Gavish E, Gottlieb P, Katsnelson L. Interobserver and intraobserver variability in the sonographic assess- ment of fatty liver. AJR Am J Roentgenol 2007;189:W320- W323
37. Dasarathy S, Dasarathy J, Khiyami A, Joseph R, Lopez R, McCullough AJ. Validity of real time ultrasound in the di- agnosis of hepatic steatosis: a prospective study. J Hepatol 2009;51:1061-1067
38. Hamer OW, Aguirre DA, Casola G, Lavine JE, Woenckhaus M, Sirlin CB. Fatty liver: imaging patterns and pitfalls. Ra- diographics 2006;26:1637-1653
39. Mendler MH, Bouillet P, Le Sidaner A, Lavoine E, Labrousse F, Sautereau D, et al. Dual-energy CT in the diagnosis and quantification of fatty liver: limited clinical value in com- parison to ultrasound scan and single-energy CT, with spe- cial reference to iron overload. J Hepatol 1998;28:785-794 40. Lee SS, Park SH. Radiologic evaluation of nonalcoholic fat- ty liver disease. World J Gastroenterol 2014;20:7392-7402
쥐를 이용한 지방간 실험모델에서 초음파, 전산화단층촬영, 자기공명영상, 자기공명분광술의 진단에 대한 비교연구
노 훈
1· Song Xiao-li
1· 허숙희
1· 김진웅
1· 신상수
2· 안규윤
3· 정용연
1· 강형근
1*
목적: 쥐를 이용한 지방간 실험모델에서 초음파(ultrasonography; 이하 US), 단일 에너지 전산화단층촬영(single energy computed tomography; 이하 SECT), 이중 에너지 전산화단층촬영(dual energy computed tomography; 이하 DECT), 자 기공명영상(magnetic resonance imaging; 이하 MRI), 자기공명분광술(magnetic resonance spectroscopy; 이하 MRS)의 진단적 정확도를 비교하고자 하였다.
대상과 방법: 실험군인 15마리의 쥐에서 60% 지방식이를 이용하여 1, 2, 3, 4, 5주간 지방간을 유발하였고 대조군인 5 마리의 쥐는 10% 지방식이를 이용하였다. 각 주마다 US, SECT, DECT, MRI와 MRS를 시행하였다. 그 후 희생된 쥐들의 간에서 조직학적, 생화학적 평가를 하였다. 영상검사결과와 조직학적인 결과의 평가를 위해 Pearson 상관계수를 이용하 였고 곡선하면적(area under the curve), 민감도, 특이도를 계산하였다.
결과: US, SECT, DECT, MRI와 MRS는 간 조직내 지방분율과 의의있는 상관관계를 보였다. 곡선하면적에 의한 진단수 행도, 민감도, 특이도는 각각 US에서 0.893, 80%, 80%; SECT에서 0.960, 80%, 80%; DECT에서 0.947, 100%, 60%; MRI에서 0.933, 93.3%, 100%; MRS에서 0.960, 93.3%, 100%였다.
결론: MRS는 간 조직내 지방분율과 가장 좋은 상관관계를 보이며 다른 검사들에 비해 지방간의 진단에 있어서 더 좋은 진단능을 보인다.
1화순전남대학교병원 영상의학과, 2전남대학교병원 영상의학과, 3전남대학교 의과대학 해부학교실