63
Preliminary Evaluation of the URiSCAN SUPER and Usefulness of a New Urine Reagent Strip to Detect Ascorbic Acid
Sang-Young Shin1, Min-Jung Kwon1, Hee-Yeon Woo1, Hyosoon Park1, and Young Jae Kim2
Department of Laboratory Medicine, Kangbuk Samsung Hospital Sungkyunkwan University School of Medicine1, Seoul;
Department of Laboratory Medicine, Samsung Changwon Hospital Sungkyunkwan University School of Medicine2, Changwon, Korea
URiSCAN SUPER의 평가와 새로운 아스코르빈산 측정 시험지봉의 유용성
신상용1․권민정1․우희연1․박효순1․김영재2
성균관대학교 의과대학 강북삼성병원 진단검사의학과1, 성균관대학교 의과대학 삼성창원병원 진단검사의학과2
접수일: 10 / 12 / 22 최종재심접수일: 11 / 8 / 2 게재승인일: 11 / 8 / 6 교신저자: 우희연
우) 110-746 서울특별시 종로구 새문 안길 78 성균관대학교 의과대학 강북 삼성병원 진단검사의학과
전화: 02)2001-2387 팩스: 02)2001-2364
E-mail: [email protected]
Background: Ascorbic acid can cause false negative results in the detection of urinary hemoglobin (Hb) with reagent test strips. The fully automated urine analyzer URiSCAN SUPER (YD Diagnostics, Korea), which can measure ascorbic acid, was recently developed. We compared the URiSCAN SUPER to the semi-automated urine analyzer URiSCAN PRO II (YD Diagnostics) and evaluated the usefulness of a new reagent strip to detect ascorbic acid.
Methods: A total of 641 urine samples were used to evaluate the agreement between the two analyzers. In addition we performed urine microscopic examinations to investigate the sensitivity and specificity of urinary Hb and white blood cells. We determined the detection limit of urine ascorbic acid. We also determined the positive rate of ascorbic acid and the false negative rate for urinary Hb. Additionally, the interference effect of ascorbic acid for urinary Hb was investigated.
Results: The agreement rate between the two analyzers was greater than 98% for all tests except for urinary specific gravity. The detection limit of urine ascorbic acid was 10 mg/dL. The positive rate of ascorbic acid was 49.8%. The false-negative rate for urinary Hb was 6.0% and 2.8% (P>0.05) in the presence and absence of urine ascorbic acid, respectively.
Conclusions: The performances of the two urine analyzers were comparable.
URiSCAN SUPER for the detection of urinary Hb was resistant to interference by ascorbic acid. Since the URiSCAN SUPER performs a fully automated analysis, it would be useful in urine screening.
Key Words: Ascorbic acid, Automation, False negative reactions, Urinalysis, URiSCAN PRO II, URiSCAN SUPER
INTRODUCTION
Urinalysis, an important tool for the screening, diagnosis, and follow-up of diseases, allows for the detection of many diseases that give rise to chemical
and physical abnormalities in urine[1]. The use of a reagent test strip for the examination of urine chemistry is a widely accepted standard of clinical practice. This simple test has become an essential component of health screenings. Numerous factors
J Lab Med Qual Assur 2011 ; 33:63-9
affect the reagent strip-based urinalysis and cause false negative or false positive results. These factors include not only elevated specific gravity (SG) and urobilinogen levels, but also the presence of ascorbic acid, myoglobin, menstrual blood, or levodopa in urine[1].
Ascorbic acid, present in various foods and dietary supplements, is widely used for disease prevention and treatment[2]. The presence of ascorbic acid in the urine can result in a falsely low or false negative response because of the peroxidase-redox indicator system on the urinalysis test strip[3-8]. The urinary presence of ascorbic acid yields false negative rates for urinary haemoglobin (Hb) and glucose that are proportional to the urinary concentration of ascorbic acid[9]. Ascorbic acid affects the peroxidase-redox system in many ways: it can interfere with the oxidase reaction, compete as a substrate for peroxidase, reverse the dye color, auto-oxidize to generate free radicals, and enhance the peroxidase-catalyzed production of radicals[4,5]. Therefore, the measurement of ascorbic acid level in urine is recommended in order to determine the possibility of false negative results not only for urinary Hb, but also for urinary glucose[9, 10].
The new automated urine analyzer, the URiSCAN SUPER (YD Diagnostics, Seoul, Korea), includes reagent strips for measuring ascorbic acid levels. This analyzer is a fully automated urine analyzer that measures 13 test items including urinary ascorbic acid and urine color and clarity. The URiSCAN SUPER does not require the manual dipping of reagent strips.
After loading a urine bottle into the URiSCAN SUPER, reagent strips are dipped automatically into the urine sample, and urinalysis is performed. The URiSCAN SUPER throughput is 260 tests per hour, and a maximum of 100 urine samples can be loaded at a time.
In this study, we compared the URiSCAN SUPER to the URiSCAN PRO II (YD Diagnostics). We also evaluated the usefulness of a new urine test strip for the detection of ascorbic acid in urine.
MATERIALS AND METHODS
1. Materials
We analyzed the urine samples of 109 hospitalized patients, 117 patients visiting the outpatient clinic,
and 415 healthy adults who underwent health screenings. Subjects ranged in age from 20 to 40. All urine samples were stored in the dark at 4°C and were analyzed within two hours of collection.
2. Methods
1) Agreement rate between URiSCAN SUPER and URiSCAN PRO II
We investigated the agreement rates for 10 test items between the new URiSCAN SUPER and the existing, semi-automated URiSCAN PRO II urine analyzer. Agreement between the two analyzers was defined as a difference between the results that was within one grade.
2) The sensitivity and specificity of urinary Hb and urinary white blood cell (WBC)
We investigated the sensitivity and specificity of urinary Hb and WBC detection by comparing the results with urine microscopic examinations. A well-trained medical technician performed the microscopic examination of all urine samples.
3) URiSCAN SUPER detection limit for ascorbic acid
Ascorbic acid was prepared at concentrations of 0, 5, 10, 25, and 50 mg/dL by the addition of 5 mg ascorbic acid powder (Sigma-Aldrich, St. Louis, MO, USA) to 2 mL of a normal urine sample, followed by serial dilution with normal urine. Ascorbic acid in the urine was measured by colorimetric methods based on the oxidation-reduction properties of ascorbic acid. We used the blue dye, 2,6-dichlorophenolindophenol (DCIP), as the reagent. Because ascorbic acid is oxidized to dehydroascorbic acid, oxidized DCIP is reduced to its colorless form at low pH levels. Each sample was measured five times using the URiSCAN SUPER analyzer.
4) The positive rate, false negative rate and interference effect of ascorbic acid on urinary Hb We investigated the positive rate of ascorbic acid in the urine. We also investigated different false- negative rates of urinary Hb according to the presence or absence of ascorbic acid by comparing results from the URiSCAN SUPER analyzer with those of microscopic examinations. Urine ascorbic acid levels
Table 1. Sensitivities and specificities of the URiSCAN SUPER and the URISCAN PRO II for urinary Hb and urinary WBC estimates compared with the urine microscopic examination
Analyzer Sensitivity (%) Specificity (%)
Urinary Hb Urinary WBC Urinary Hb Urinary WBC
URISCAN PRO II 69.7 76.8 94.1 96.5
URiSCAN Super 77.0 87.0 92.0 94.3
Abbreviations: Hb, hemoglobin; WBC, white blood cell.
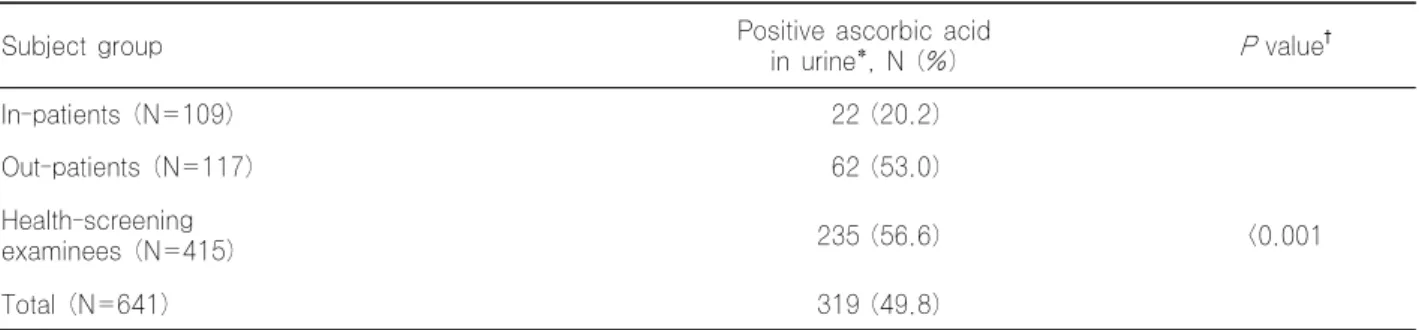
Table 2. Positive rate of ascorbic acid in urine
Subject group Positive ascorbic acid
in urine*, N (%) Pvalue†
In-patients (N=109) 22 (20.2)
Out-patients (N=117) 62 (53.0)
Health-screening
examinees (N=415) 235 (56.6) <0.001
Total (N=641) 319 (49.8)
*Urine showing ≥1+ ascorbic acid value with the URiSCAN SUPER analyser; †Chi-square test was used.
were measured with the URiSCAN SUPER analyzer.
To assess Hb interference, red blood cell (RBC) concentrations of 0, 5, 10, 50, and 240 cells/µL were added to the urine specimens containing ascorbic acid at 0, 10, 25, 50, 100, 200, and 500 mg/dL.
3. Statistics
The Excel 2000 statistics package (Microsoft Corporation, Redmond, WA, USA) was used to calculate the agreement rates. We utilized a Chi-square analysis to compare the differences among groups using SPSS version 12.0 (SPSS, Chicago, IL, USA). P values less than 0.05 were considered statistically significant.
RESULTS
1. The agreement rate between URiSCAN SUPER and URiSCAN Pro II
Agreement rates of more than 98% were observed for all of the test items except for urinary SG. The agreement rates for the presence of urinary Hb, WBC, bilirubin, urobilinogen, ketone, protein, nitrite, and glucose were 98.8%, 99.1%, 100%, 100%, 100%, 99.4%, 100%, and 100%, respectively. The agreement
rates for pH and SG were 98.8%, and 77.1%, respectively.
2. The sensitivity and specificity of urinary Hb and urinary WBC
The sensitivities of the URiSCAN PRO II and URiSCAN SUPER analyzers for urinary Hb were 69.7% and 77.0% respectively, while the specificities for urinary Hb were 94.1% and 92.0%, respectively.
The sensitivities of the URiSCAN PRO II and URiSCAN SUPER analyzers for urinary WBC were 76.8% and 87.0%, respectively. The specificities for urinary WBC of the URiSCAN PRO II and URiSCAN SUPER analyzers were 96.5% and 94.3%, respectively (Table 1).
3. The detection limit of the URiSCAN SUPER for ascorbic acid
The lowest concentration of ascorbic acid detected by the URiSCAN SUPER analyzer was 10 mg/dL.
4. The positive rate, false negative rate, and interference effects of ascorbic acid for urinary Hb Although the overall positive rate of urinary ascorbic acid detection was 49.8%, ascorbic acid was
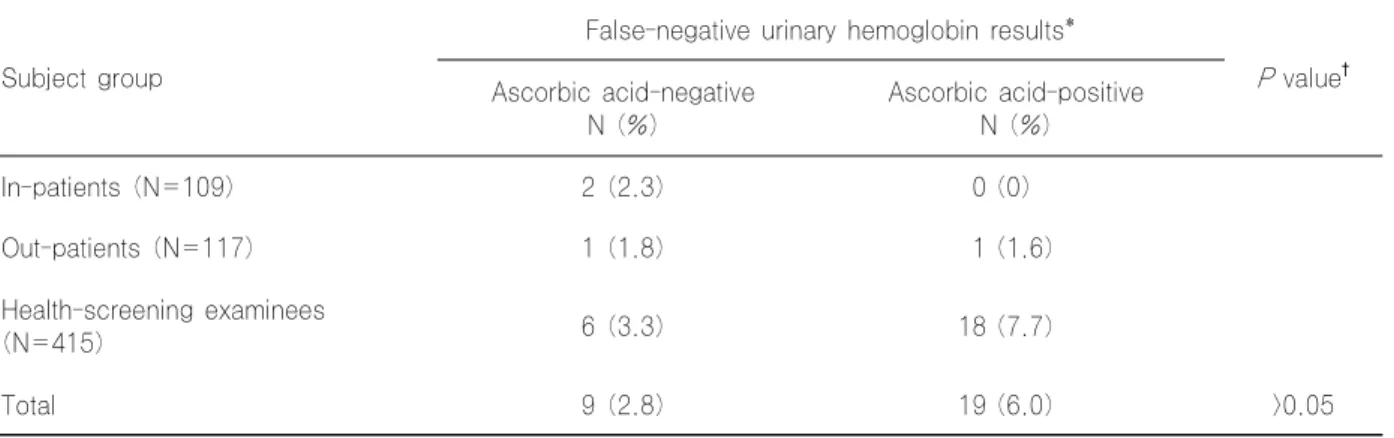
Table 3. False negative rate of hemoglobin in urine Subject group
False-negative urinary hemoglobin results*
Pvalue† Ascorbic acid-negative
N (%) Ascorbic acid-positive N (%)
In-patients (N=109) 2 (2.3) 0 (0)
Out-patients (N=117) 1 (1.8) 1 (1.6)
Health-screening examinees
(N=415) 6 (3.3) 18 (7.7)
Total 9 (2.8) 19 (6.0) >0.05
*Ascorbic acid interference was defined as a false-negative urinary hemoglobin result accompanied by a positive test result for urinary ascorbic acid; †Chi-square test was used.
Table 4. Interference effect of ascorbic acid for urinary hemoglobin
Blood (RBC/µL) Ascorbic acid (mg/dL)
0 10 25 50 200 500
0 Neg Neg Neg Neg Neg Neg
5 Trace Trace Trace Trace Neg* Neg*
10 1+ 1+ 1+ 1+ 1+ 1+
50 2+ 2+ 2+ 2+ 2+ 2+
250 3+ 3+ 3+ 2+ 3+ 3+
*False negative results.
Abbreviations: RBC, red blood cell; Neg, negative.
present in the urine samples of 20.2% of the inpatients, 53.0% of the outpatients, and in 56.6%
of the health-screening examinees (Table 2). The positive rate in the health-screening examinees was significantly higher than in those of inpatients and outpatients (P<0.001).
The false-negative rate for urinary Hb in the presence of urine ascorbic acid was 6.0%. This rate was higher than the 2.8% in the absence of urine ascorbic acid. However, this difference was not statistically significant (P>0.05) (Table 3). For the in-patient group, the false negative rate was not higher in the presence of urine ascorbic acid than in the absence of urine ascorbic acid. Table 4 shows the data for the interference with Hb reactions in the presence of various ascorbic acid concentrations. At ascorbic acid concentrations ≥200 mg/dL, the URiSCAN
SUPER analyzer showed interference.
DISCUSSION
The agreement rates between the two different urine analyzers was greater than 98% for all test items except for the detection of urinary SG, which showed an agreement rate of 77.1%. This relatively low agreement rate for urinary SG might be due to the different unit intervals and measurement principles intrinsic to the two different analyzers. The reagent strips are used to measure the ionic concentration in the URiSCAN PRO II, which is then related to SG with values reported at unit intervals of 0.005. In the URiSCAN SUPER, a drop of urine is placed into the instrument (without reagent strips), and the SG is measured by a refractometer with the values reported
at unit intervals of 0.001. The SG measurements from reagent strips are influenced by urinary pH, glucose, and ionic concentrations, while the refractometer measurements are influenced by urinary glucose, protein levels, and temperature[11]. Methods to correct these factors when measuring urinary SG have been proposed[12,13]. In our study, the urinary SG results from the URiSCAN PRO II analyzer were automatically corrected by the addition of 0.005 to the raw SG values in urine specimens with a pH ≥7.0 or a glucose concentration ≥1,000 mg/dL. Several studies that compared the urinary SG generated by reagent strips with those from a refractometer reported different results[14-16]. Moreover, different SG estimates were reported in studies that compared a reagent strip to an osmometer, which is the gold standard for the measurement of SG[14-16]. One study reported that the correction for urinary pH could influence the urinary SG measurements of a reagent strip. Improved correlation between reagent strip results and those obtained by a refractometer was also observed[13]. Another study reported that, even after correction for urinary pH, the reagent strip results were unreliable[16]. Therefore, it is important for the clinician to know this limitation when comparing urinary SG values according to osmolality. We did not measure the urine osmolality in this study and therefore cannot evaluate whether reagent strips or refractometer methods are more accurate for measuring urinary SG.
The sensitivity of the URiSCAN SUPER analyzer for detecting urinary Hb and WBC was higher than that of the URiSCAN PRO II. However, the specificity of the URiSCAN SUPER analyzer for detecting urinary Hb and WBC was lower than that of the URiSCAN PRO II. Therefore, microscopic examination of the urine is required to correct for false-positive results generated by the URiSCAN SUPER analyzer. In general, it is recommended that a positive dipstick test result for urinary Hb be confirmed by urine microscopic examination[17].
Health-screening examinees had higher urinary Hb false-negative rates than those of the patients in this study. The prevalence of asymptomatic microscopic hematuria based on dipstick testing has been reported to range between 2% and 16%[18]. The underlying causes of asymptomatic microscopic hematuria vary from urethritis to urogenital malignancies[19]. The
detection of microscopic hematuria is more important in older individuals than in younger individuals because severe urologic disease is more likely in elderly individuals[20]. Therefore, the failure to detect hematuria due to a false-negative urinary Hb result might have more serious consequences in older patients. It is recommended that asymptomatic microscopic hematuria (>3 RBCs/high power field on two of three properly performed and collected urinalyses) should be referred to a urologist for complete evaluation[21].
There are many factors that cause false-negative results for urinary Hb. These factors include the use of formalin as a preservative, a high SG, and the presence of ascorbic acid and high protein levels in the urine. Among these interfering factors, the URiSCAN SUPER analyzer can semi-quantitatively measure urine ascorbic acid levels. A high positive rate of urinary ascorbic acid, 49.8% (319/641), was observed in this study. The lowest concentration of urinary ascorbic acid that can cause false negative urinary Hb results has been reported to range from 8.8 mg/dL to 11-21 mg/dL[9,22]. Therefore, various methods have been developed to improve the performance of dipsticks in the presence of ascorbic acid, but the interference reaction still occurs at high ascorbic acid concentrations[6,9]. Our data showed that the URiSCAN SUPER analyzer was resistant to the interference effect of ascorbic acid for urine Hb (Table 4). Only samples with low RBC and high ascorbic acid concentrations showed false-negative results. The manufacturer has developed various methods to reduce the interference of ascorbic acid. The incorporation of oxidants into the reagent strip reduces the interference in the hemoglobin reaction by rapidly oxidizing the ascorbic acid to dehydroas- corbate[6]. Using a metallic oxidant, URiSCAN SUPER reduced the interference effect of ascorbic acid.
The false negative rate of urinary Hb results was 6.0% in ascorbic acid positive samples and 2.8% in ascorbic acid negative samples. However, the false negative rates were not significantly different in ascorbic acid-positive urine compared to those in ascorbic acid-negative urine (P>0.05). Moreover, in the case of patient groups, the false negative rates were higher in the ascorbic acid-negative group (inpatient group-2.3%, outpatient group-1.8%) than
the ascorbic acid-positive group (inpatient group-0%, outpatient group-1.6%). We thought that these results were due to the good performance of URiSCAN SUPER in reducing the interference effect of ascorbic acid. Considering the fact that false-negative results also occurred in ascorbic acid-negative urine as well as in ascorbic acid-positive urine, we concluded that there were other interfering factor(s) in addition to ascorbic acid. The false negative rate was higher in the health-screening examinees group compared to the patients group. Possible interfering factors include high SG, the presence of formalin, and high protein levels[3]. Therefore, clinicians must be aware of these factors when interpreting the results of reagent strip-based urinalysis, especially in health-screening examinees. In addition, urine ascorbic acid can also cause false-negative results in testing urine nitrite and glucose with reagent strips[3]. We did not compare URiSCAN SUPER results with quantitative measurements for urine nitrite and glucose as we could not evaluate the effects of ascorbic acid on these test items.
In conclusion, the results obtained using the URiSCAN SUPER analyzer were consistent with those of the URiSCAN PRO II for all items evaluated, except for SG. Further studies that compare urinary SG measurements obtained using the URiSCAN SUPER analyzer with urine osmolality are required. The URiSCAN SUPER analyzer showed superior sensitivity for urine Hb and WBC, but the specificity of those items was superior when assessed by the URiSCAN PRO II analyzer. Therefore, microscopic examination of urine is still needed to correct for false-negative results. Since the URiSCAN SUPER analyzer can detect ascorbic acid in urine, it can be used to evaluate the possibility of ascorbic acid interference with the urinary Hb assay. However, the URiSCAN SUPER was resistant to the interfering effect of ascorbic acid. Clinicians must be aware of other interfering factors when interpreting the results of reagent strip-based urinalysis, especially in health-screening examinees.
요 약
배경: 아스코르빈산은 시험지봉을 이용한 요중 혈색소 측정 에서 위음성을 유발할 수 있다. 아스코르빈산을 측정할 수 있는 전자동 요분석기인URiSCAN SUPER (YD Diagnostics,
Korea)가 최근 개발되었다. 저자들은 반자동 요분석기인 URiSCAN PRO II 와 URiSCAN SUPER (YD Diagnostics)를 비교하였고 요중 아스코르빈산을 측정할 수 있는 새로운 시험지봉의 유용성을 평가하였다.
방법: 641개의 요 검체를 이용하여 두 장비의 일치율을 구하 였다. 요검경을 실시하여 요중 혈색소와 백혈구 측정의 민감도 와 특이도를 구하였다. 저자들은 아스코르빈산 측정한계를 구 하였다. 또한 요중 아스코르빈산 양성률과 요중 혈색소 위음성 률을 구하였다. 추가적으로 요중 아스코르빈산에 의한 요중 혈 색소의 간섭을 평가하였다.
결과: 요비중을 제외하고 두 장비의 일치율은 98% 이상이 었다. 요중 아스코르빈산의 검출한계는 10mg/dL였다. 요중 아스코르빈산 양성률은 49.8%였다. 요중 헤모글로빈의 위음 성률은 아스코르빈산 양성인 경우 6.0%였고 아스코르빈산이 음성인 경우 2.8%였다(P>0.05).
결론: 두 요분석 장비의 성능은 유사했다. URiSCAN SUPER는 요중 혈색소 측정에서 아스코르빈산의 간섭효과를 덜 받는다. URiSCAN SUPER는 전자동 분석이 가능하므로 요선별검사로 유용할 것이다.
REFERENCES
1. Simerville JA, Maxted WC, Pahira JJ. Urinalysis: a comprehensive review. Am Fam Physician 2005;71:1153-62.
2. McGregor GP and Biesalski HK. Rationale and impact of vitamin C in clinical nutrition. Curr Opin Clin Nutr Metab Care 2006;9:697-703.
3. McPherson RA , Pincus MR, et al. eds. Henry's Clinical Diagnosis and Management by Laboratory Methods. 21th ed.
Philadelpia: Saunders Elsevier, 2007:393-425.
4. White-Stevens RH. Interference by ascorbic acid in test systems involving peroxidase. I. Reversible indicators and the effects of copper, iron, and mercury. Clin Chem 1982;28:578-88.
5. Hirata F and Hayaishi O. Studies on indoleamine 2,3-dioxygenase. I. Superoxide anion as substrate. J Biol Chem 1975;250:5960-6.
6. White-Stevens RH and Stover LR. Interference by ascorbic acid in test systems involving peroxidase. II. Redox-coupled indicator systems. Clin Chem 1982;28:589-95.
7. Martinello F and Luiz da Silva E. Mechanism of ascorbic acid interference in biochemical tests that use peroxide and peroxidase to generate chromophore. Clin Chim Acta 2006;373:108-16.
8. Berg B. Ascorbate interference in the estimation of urinary glucose by test strips. J Clin Chem Clin Biochem 1986;24:89-96.
9. Brigden ML, Edgell D, McPherson M, Leadbeater A, Hoag G.
High incidence of significant urinary ascorbic acid concentrations in a west coast population--implications for routine urinalysis.
Clin Chem 1992;38:426-31.
10. Brigden ML. Unorthodox therapy and your cancer patient.
Postgrad Med 1987;81:271-2, 275-7, 280.
11. de Buys Roessingh AS, Drukker A, Guignard JP. Dipstick measurements of urine specific gravity are unreliable. Arch Dis Child 2001;85:155-7.
12. Gounden D and Newall RG. Urine specific gravity measurements: comparison of a new reagent strip method with existing methodologies, as applied to the water concentration/
dilution tests. Curr Med Res Opin 1983;8:375-81.
13. McCrossin T and Roy LP. Comparison of hydrometry, refractometry, osmometry and Ames N-Multistix SG in estimation of urinary concentration. Aust Paediatr J 1985;
21:185-8.
14. Chadha V, Garg U, Alon US. Measurement of urinary concentration: a critical appraisal of methodologies. Pediatr Nephrol 2001;16:374-82.
15. Burkhardt AE, Johnston KG, Waszak CE, Jackson CE, Shafer SR. A reagent strip for measuring the specific gravity of urine.
Clin Chem 1982;28:2068-72.
16. Chu SY and Sparks D. Assessment of a solid-phase reagent for
urinary specific gravity determination. Clin Biochem 1984;17:34-6.
17. Rao PK, Gao T, Pohl M, Jones JS. Dipstick pseudohematuria:
unnecessary consultation and evaluation. J Urol 2010;183:560-4.
18. Rockall AG, Newman-Sanders AP, al-Kutoubi MA, Vale JA.
Haematuria. Postgrad Med J 1997;73:129-36.
19. Mariani AJ, Mariani MC, Macchioni C, Stams UK, Hariharan A, Moriera A. The significance of adult hematuria: 1,000 hematuria evaluations including a risk-benefit and cost- effectiveness analysis. J Urol 1989;141:350-5.
20. Sultana SR, Goodman CM, Byrne DJ, Baxby K. Microscopic haematuria: urological investigation using a standard protocol.
Br J Urol 1996;78:691-6.
21. Loo R, Whittaker J, Rabrenivich V. National practice recommendations for hematuria: how to evaluate in the absence of strong evidence? Perm J 2009;13:37-46.
22. Zweig MH and Jackson A. Ascorbic acid interference in reagent-strip reactions for assay of urinary glucose and hemoglobin. Clin Chem 1986;32:674-7.