대한망사선의학호1:;\11998;39:793-799
양성 거대세포종에서 종양주위 골수부종1
김성헌·박정미·검지영·지원희·성미숙·이재문·신경섭
목 적 : 사지골에서 발생한 거대세포종에서 자기공명 (MR) 영상 검사상 골수부종이 얼 마나 동반되는지 또 골수부종과 단순 X 천 사진 빛 골신티그램 소견과의 연관성을 알아 보 고자한다.
대상 및 방법 : 병리조직학적으로 확진된 사지골에서 발생된 양성 거대세포종 18예의 단순 X진 사진, 골신티그램 및 MR 영상 소견을 후향적으로 분석하였다. 18예에 대해서 전부
MR 검사를 시행하였고 이중 15예에서 단순 X 진 사진을 얻을 수 있었고 골신티그램은 6예 에서만시행하였다.
거대세포종 종양주변부 골수부총은 T1 강조영상에서 저신호강도 또는 중등도 신호강도,
T2 강조영상에서 고신호강도, 조영증강후에는 균일한 조영증강을 보이는 것으로 정의하였 다. 단순 X진 사진상 종양에 의 한 골파괴 와 정 상골사이 의 이 행 범 위 (transition zone) 가 넓 은지 흑은 좁은지, 종양경계에 경화성 테두리 유무 및 병변의 침습정도 (aggressi veness)를 분석하여 MR 영상 사진에서 보이는 골수부종과 단순 X 전 사진상의 소견 및 골신티그램상 의 침습정도와의 연관성을 분석하였다.
결 과 :1. 사지골에 발생한 거대세포종에 있어서 종양주변의 골수부종은 MR 영상 사진 상 18예중 10예 (55.5%) 에서 동반된 것을 관찰할 수 있었다.
2. 단순 X 건 사진과 MR 영상 소견을 비교 분석할 수 있었던 15예중 골수부종은 8예에서 관찰할 수 있었고 이중 6예에서는 단순 X천 사진상 넓은 이행범위를 보이는 반면, 골수부 종이 없었던 7예중 6예에서는 단순 X 진 사진상 종양의 이행범위가 좁게 관찰되어 골수부 종유무와 단순 X 진 사진상 보이는 이행범위의 양상은 통계학적으로 유의한 상관관계가 있
었다 (x
2, p=O.05). 그러나 골수부종유무와단순 X 천 사진상 보이는 침습정도와는 약한 상
관관계를 보였고 경화성 테두리 유무와는 유의한 상관관계가 없었다.
3. 골신티그램을 시행한 6예는 모두 단순 X정 사진상 종양의 침습범위를 넘어서는 핵제 제의 섭취를 보였으며 이들 중 5예에서는 MR 영상 사진상 부종의 소견을 나타냈다.
결 론 . 사지골에서 발생된 양성 거대세포종에서도 MR 영상에서 종양주위에 골수부종 이 흔히 동반되었으며 (55.5%), 단순 X 천 촬영에서 골파괴와 정상골사이의 이행범위가 넓 은 경우 골수부종이 더 많이 나타나는 것을 알 수 있었다.
1987년 근골격계 종양에 동반된 부종을 시사하는 MR 소견 에 대한 첫번째 보고 이후(1), 여러 가지 양성과 악성종양에서 종양 주변부위 골수 및 연부조직 부종이 보고 되었다 (2-4). 골 의 양성질환 중 골수 부종은 연골아세포종 (chondroblastoma) , 유골 골종 (osteoid osteoma), 골아세포종 (osteoblastoma) 에 서 빈번하게 보이고, 거대세포종에서는 드물게 보이는 것으로 알려져 있다(5, 6).
이 연구의 목적은 양성 거대세포종의 MR 영상에서 골수부 종이 동반되는 빈도를 알아보고 MR상 보이는 골수부종과 단 순 X 진 사진, 골신티그램 소견과의 연관성을 분석하고자 하였 다.
대상및방법
1990년부터 1996년까지 병리조직학적으로 확진된, 사지골에 l 가톨릭대학교의과대학방사선과학교실 서 발생한 양성 거대세포종 18예의 MR 영상과 이중 단순
x-
본 논문은 1998년도 가툴릭중앙의료원 학술연구 보조비로 이루어졌음 선 사진을 얻을 수 있였던 15예와 6예의 골신티그램을 대상으
이 논문은 1998년 3월 25일 접수하여 1998년 7월 28일에 채택되었음.
m m
로 후향적 분석을 하였다.
남녀비는 8: 10으로 여자가 약간 많았으며, 연령 분포는 14세 에서 48세 였다(평균 연령 31세) . 병소의 위치는 대퇴골 원위부 2예, 경골 근위부가 8예로 무릎관절부위가 10예였고, 대퇴골 근 위부 1예, 상완골 근위부 2예, 요골 원위부 2예, 종골, 비골, 슬 개골이 각각 l예였다. 장골의 거대 세포종은 골 수질에서 편향 (eccentric) 되게 위치하였다.
MR 촬영은 모든 예에서 스핀에코 (spin echo) 기법으로 T1 및 T2 강조영상의 횡단영상 빛 병소의 부위에 따라 시상 및 관 상영상을 얻었다. MR영상은 14예는 0.5 Tesla Gyroscan T5
(Philips, Amsterdam, Netherland)를 사용하여, 스핀에코 기 법으로 T1(TR/TE 460/20msec) 강조영상과 T2(TR/TE 1800/90 msec) 강조영상을 얻었고, 4예는 1.5 Tesla Signa (GE Medical Systems, Milwaukee, USA) 를 사용하여, 스핀 에코 기법으로 Tl(TR/TE 450/20msec) 강조영상과 T2 (TR/TE 1800/80msec) 강조영상을 얻었다. 시야는 160- 210mm, 절편두께는 5mm 로 하였다. 또한 전례에서 Gadolin ium-DTPA(Gd)를 정맥 주사한 후 T1 강조영상을 얻었다.
MR 영상에서 종양 주변부 골수부종은 T1 강조영상에서는 저신호강도 또는 중등도 신호강도, T2 강조영상에서는 고신호 강도, 조영 증강후에는 균일한 조영 증강을 보이는 것으로 정의 하였다. 거대세포종 주변 골수의 부종 여부를 알아 보았고, T1 강조영상에서 종양을 둘러싸고 있는 저신호강도의 테두리 (hy- pointense rim) 유무를 알아보았다.
단순 X선 사진에서는종양에 의한골파괴와정상골사이의
김성헌 오1: 양성 거대세포종에서 종앙주위 골수부종
이행범위 (transition zone) 가 좁은지 흑은 넓은지, 종양경계에 경화성 테두리 유무 빛 병변의 침습정도(aggressiveness)를 이 용하여 분석하였다. 이행범위가 부분적으로 넓은 경우도 넓은 이행범위로 포함하였다. Enneking의 수정 병기결정계 (modi fied staging system) 에서는 단순 X 선 사진으로 거대세포종 의 침습정도를 분류하였다. (7) 이를 근거로 침습정도를 단순 히 골파괴만 있고 골팽창이 없는 경우는 잠복형(latent)으로,
종양에 의해 골팽창이 있으나 골피질의 파괴가 없는 경우는 촬 성형(active)으로, 콜피질을 파괴하며 주변조직으로 침범을 보 이는 경우는 공격형 (aggressi ve)으로 구분하였다.
TC99m_MDP 골신티그램을 시행한 6예에서 확장된 방사능 집적 (extended uptake) 유무를 알아보았다. 단순 사진의 골파 괴 범위를 넘어서서 골신티그램에서 핵제재의 섭취가 있을 때 확장된 방사능 집적이 있는 것으로 보았다. 또한 MR 영상에서 보이는 골수부종과 단순 X 진 사진상의 소견 및 골신티그램상 의 침범정도와의 연관성을 ; 검정법을 사용하여 비교 분석하 였다.
결 과
거대세포종 각 증례의 MR, 단순 X 진 사진 및 골스캔의 소 견은 Table 1 과 같다.
MR 영상에서 종양주변부의 골수부종은 18예중 10예 (55.5
%)에서 동반되 었으며 (Fig. 1) MR T1 강조영상에서 종OJ:을 둘러싸는 저신호강도의 띠는 18예중 10여1 (55.5%) 에서 관칠되
Table 1. Case Analysis of the GCT on the MR, Plain Radiography & Bone Scintigraphy
No of MRI PLAIN X-RAY BONE SCAN
Age/Sex Location
T/Z
Case Edema Hypo rim Scl Mar Aggressiveness Ext Uptake
14/F P humerus (+) (- )
w
(- ) Aggressive (+)2 17/M P femur (+) (- )
w
(- ) Latent (+)3 20/M P tibia (+) (+) N (+) Active NA
4 21/M P humerus (+) (- )
w
(- ) Aggressive NA5 25/M D radius (+) (+) NA NA NA (- )
6 25/F D femur (+ ) (+)
w
(- ) Aggressive (+)7 38/F P tibia (+) (- ) NA NA NA NA
8 40/F P tibia (+) (+)
w
(- ) Aggressive (+)9 44/M D femur (+) (+ )
w
(- ) Active (+ )10 48/F D radius (+) (•) N (- ) Aggressive NA
11 23/M Calcaneus
(- )
(+) N (+) Latent NA12 27/M P tibia (- ) (+) N (- ) Active NA
13 30/F Patella (- ) (+) N (- ) Active NA
14 33/M P fibula (- )
(- )
N (- ) Active NA15 34/M P tibia (- ) (- )
w
(- ) Active NA16 37/F P tibia (- ) (+) N
(+)
Aggressive NA17 38/F P tibia
(- )
(- ) N (- ) Active NA18 42/F P tibia
(- )
( +) NA NA NA NAGCT: giant cell tumor P : proximal D: distal Hypo rim:hypointense rim
(+) :
positive ( - ) : negative T /Z: transition zone NA: not available W: wide N: narrow Scl mar:sclerotic margin Ext uptake: extended uptake…
대한방사선의학호1::\11998;39:793-799
었다.
MR 영상과 단순 X전 사진이 모두 있었던 15예에서 골수부 종과 단순 X선 사진상의 연관성을 분석한 결과 골수부종이 있 던 8예중 6예에서 이행범위가 넓게 보였고 골수부종이 없었던
Table 2. Correlation of BM Edema on MR and Transition Zone on Radiography of the GCT
PLAIN Transition Zone
Total
MR ____________ W ide Narrow
EDEMA
+
6 2 86 7
Total 7 8 15
x2,
P
< 0.05A
7예중 6예가 이행범위가 좁게 관찰되어 골수부종과 이행범위 양상은 통계학적으로 유의한 상관관계가 있었다 (Table 2) (Fig. 2). 골수부종과 단순 사진상 보이는 경화성 테두리 유무 와는 유의한 상관관계가 없었으나 (Table 3) 침습정도오}는 약
Table 3. Correlation of BM Edema on MR and Sclerotic Rim on Radiography of the GCT
_________ PLAIN Sclerotic rim
--- - _ .• _.‘ Total
MR ______________ (
+ ) ( - )
EDEMA
+
7 82 3 7
Total
x2, P
>
0.053 12 15
B
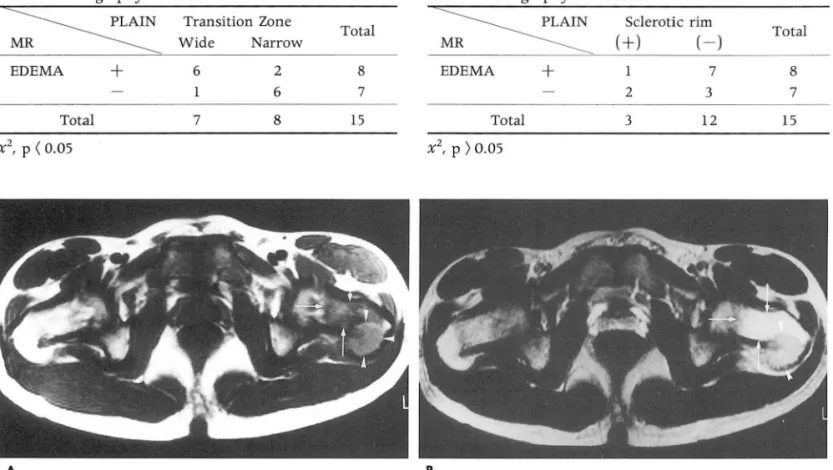
Fig. 1. A. Axial T1-weighted spin echo MR image demonstrates indistinct areas of low signal intensity(SI) in the mar- row (white arrows) outside the well-defined margins of the tumor (white arrowheads) at the greater trochanter of the proximal femur
B. Axial T2-weighted spin echo MR image shows peritumoral edematous homogeneous high SI (white arrows) in the neck adjacent to the GCT mass (white arrowheads).
A B
- 795 -
Fig. 2. Case 8
A. Plain radiograph shows a poorly defined osteolytic lesion with a wide transition zone in the proxi- mal tibia.
B. Coronal T2-weighted image reve als peritumoral bone marrow edema as an area of high SI(black arrows)
김성헌 오1 : 암성 거대세포종에서 종암주위 골수부종
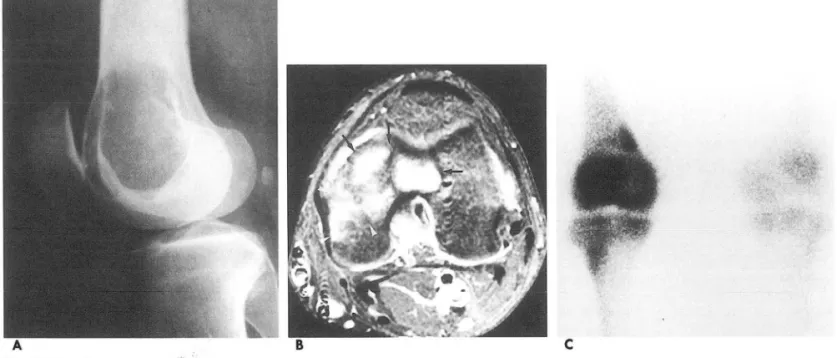
C Fig. 3. Case 9
A. Plain lateral radiograph shows subarticular osteolytic lesion in the lateral femoral condyle.
B. Coronal fat saturation enhanced T1-weighted image demonstrates edematous increased SI (white arrowheads) a이 ac
ent the tumor (black arrows).
C. Bone scan reveals increased tracer activity beyond the anatomic limit of the tumor
Table 4. Correlation of BM Edema on MR and Aggress- Table S. Correlation of Hypointense Rim on MR T1 WI lveness on Radiography of the GCT and Marginal Sclerosis on Radiography of the GCT
PLA1N Aggressiveness
Total
MR ---~ latent + acti ve aggress
EDEMA + 3(1+2) 5 8
6(1+5) 7
Total 9 6 15
x2, P
=
0.1, marginally significant한 상관관계를 보<j q(Table 4). 단순 X 전 사진에서 경화성 태두리가 없는 12예 중 7예에서는
MR
영상에서도 저신호강도 의 띠를 보이지 않았으나 5예에서는 저신호강도의 띠가 보였고,단순 X 선 사진에서 경화성 테두리가 있는 3예 모두
MR
영상 에서 저신호강도의 띠를 보였으나 통계학적으로 유의한 상관관 계는 없었 q(Table 5).골신티그램을 시행한 6여l 모두 단순 사진상 보이는 종양의 침습범위를넘어서는핵제제의 섭취를보였으며 이들중 5예에 서
MR
영상에서 골수부종의 소견이 보였다 (Fig.3).고 찰
MR
영상은 골수와 연부조직의 신호강도 변화를 잘나타내주 므로 근골격계 질환의 진단 및 감별진단에 불가결한 방사선학 적 검사방법이 되고 있다. 그러나 높은 민감도로 인해 양성 골 병변의 공격성 (aggressiveness) 과 침범범위를 과장되게 나타 내 주는 단점이 있다. 그 대표적인MR
소견 중의 하나가 골수 부종이다.MR
영상에서 골수부종은 T1 강조영상에서 불명확~ _________ -PLA1N ---. Sclerotic Ri ~ ~--- ~ .---.---- Total
MR ____________
+
Hypointens + 3 5 8
Rim
Total x2, P > 0.05
0 3
7 12
7 15
한 경계를 갖는 중등도 신호강도의 병변이, T2 강조영상, 지방 억제 가법 (fat suppression), 그리고 STIR 영상에서 신호강도 가 증가할 때 의심할 수 있다 (8, 9).
종양주위에 골수부종은 종양등의 자극에 대한 조직의 비특이 적인 반응으로 알려져 있고 세포외 물성분의 증가는 혈관과다
(hypervascularity), 관류증가 (hyperperfusion) 의 정도에 영 향을 받는다 (8, 9). 부종이 보이는 콧의 조직은 결합조직과 만 성 염증세포 침윤과 함께 상당한 양의 부종액을 보인다(1이.
Crim 등은 골아세포종에서 주변 골수의 만성 염증 침윤 반응
을 장개현상 (f1are phenomenon) 으로 명명하였다(11). 그러나 이러한 염증반응은 조직학적으로 다양한 양상을 띄며, 염증반 응이 관찰되지 않을 수도 있다(1 2, 13). Kroon등은 조직학적 확인이 가능 했던 환자들에서 골수부종이 보인 곳에서 위와 같 은 염증 소견이 보이지 않았음을 보고 했고 (5) , 본연구에서도 공격적인 모습 (aggressive nature) 으로 인해 광범위 제거술 (wide resection) 을 시행받은 4예에서도 염증반응의 조직 소견 은보이지 않았다.
또한
MR
영상의 종%¥주변부 부종이 종양 조직의 프로스타대한방사선의학호|지 1998; 39: 793-799
글란딘 (PG) 측정치와 연관성이 있음이 보고 되었다( 6). 특히 연골아세포종에서 프로스타글란딘 측정치가 골수부종이 적게 보이는 다른 양성 골종양보다 현저히 높았다. 프로스타글란딘 은 염증반응, 통증과 혈관이완을 조절하는 물질이며 정상 골 대 사의 중요한 매개체이다. 따라서 이러한 자동조절이 없는 골형 성종양은 많은 양의 프로스타글란딘을 생성하는 것으로 추정된 다. 골수부종은 양성, 악성 병변 모두에서 광범위하게 나타나므 로 골수부종의 존재와 벙위는 단일 골병변의 생물학적 활성
(bi이 ogic potentiaI)을 시사하는 지표는 아니다 (5) . 하지만 이 러한 현상에 대한 이해는 병변 크기의 과장 (overestimation) , 생검 채취 오류를피하고수술전 검사시 정확한진단뿐아니라 추적 검사에서 잔류명변과재발 병변을찾는데 아주중요하다 (5,14,15).
종양 주변부 부종과 종양과의 감별에 있어 골수부종은 종양 과 유사한 신호강도 때문에 T1 강조영상에서는 구별이 어렵다.
T2 강조영상에서도구별하기는 어렵지만, 대부분의 종양의 비 균일성 (inhomogenei ty) 과 부종의 균일한 신호강도가 이 물을 감별하는데 도움을 준다. Gd DTPA 주사 후 T1 강조영상에서 는 골수와 연부조직 부종이 거의 예외 없이 균일한 조영증강을 보이는 반면 종양조직은 비균일하게 구불구불한 (serpentine) 조영증강을 보이므로 대부분의 경우에 있어 감별을 가능하게 해준다(1 1, 16, 17).
골수부종은 단순 골신티그램에서는 방사능 집적이 증가되어 보이고(1 8) 삼상 골신티그램 (three phase r adionuclide bone scan) 에서는 모든 시기에 방사능이 증가되어 보인다(1 9). 거대 세포종에서 골신티그램은 종양의 범위를 넘어서는 확장된 방사 능 집적을 보이는 경우가 많아 유용성이 적은 것으로 알려져 있 다 (7). Hudson등은 거대세포종 37예중 25예에서, Levine등은 21예중 10예에서 골신티그램상 확장된 방사능 집척을 보고하였 다 (20, 21). 본 연구에서 골신티그램을 시행한 6예 모두 확장된 방사능 집척을 보였고 이중 5예가 MR 영상에서 골수부종이 동반되었던 것을 연관지어 볼 때,저자들은 이러한 확장된 방사 능 집척의 현상이 종양 주변에 생긴 반응성 신생골 (reactive new bone) 에 의해 또는 골수부종과 연관된 혈류증가에 의한 골섭취 방사능 약품 집적을 반영하는 것으로 생각한다 (20, 22).
Kroon등운 근골격계 종양에서 골수부종은 악성종양보다는 양성질환을 갖는 환자에서 더 빈번하게 나다남을 보고 하였다
(5). 특히 연골아세포종, 유골 골종, 골아세포총에서 많이 보고
되고 있으며, 악성 종양중에서는 골육종이 가장 빈번하게 골수 부종의 소견을 보이는 것으로 알려져 있다. Kroon등은 4예의 거대세포종중 1예에서, Yamamura등은 6예의 거대세포종중 l 예에서 골수부종이 적은 빈도로 나타남을 보고하였으나 (5, 6), 본연구에서는 골수부종이 거대세포종주위에 훨씬 많이 관찰되 었다 (55.5%). MR에서 종öJ주변의 저신호강도 테두리는 종양 주변 경화 (marginal sclerosis) 에 의한 것으로 추정되며 임상 적 의의는 아직 밝혀지지 않았다 (7, 23). 이등 (24) 은 장골에서 의 거대세포종 11예중 10예에서 종양주변의 저신호강도 테두리 가 있었고 단순 X진 사진이 업수가능하였던 7예중 3예에서만 종양주변 골경화를 보였다고 보고하였다. 이러한 결과를 토대
로 저신호강도의 테두리가 모두 골경화에 의한 것은 아니며 기 질의 섬유화 (stromal fibrosis) 나 종양조직에 의해 눌린 정상 골수조직등의 가능성을 제시하였다. 본 연구에서도 단순 X 진 사진에서 경화성 테두리가 없는 경우에도 MR 영상에서 저신 호강도의 테두리가 있는 경우가 많아 (41%, Table 5) 저신호강 도의 태두리가 경화성 테두리 자체를 나타내는 것은 아니며 이 에 대한 병리조직 학적 소견과의 비교연구가 필요할 것으로 생 각된다.
전형적인 거대세포종은 젊은나이에, 좁은 이행범위를 갖지만 경화성 테두리가 없는 골파괴를 보이고 대퇴골 하단, 경골 근위 부 또는 요골 원위부의 골간단 (metaphysis) 에서 생기는 특정 을 보인다. 거대세포종의 조직학적 생물학적 활성도는 단순
x-
선 사진에서 가장 잘 보인다 (2, 3). 거대세포종은 단순 X 선 사 진상 좁은 이행범위를 갖는 것이 특정적이긴 하나 본 연구에서 는 15예중 7예에서 종양의 이행범위가 넓게 관찰되었으며 이는 아마도 이행범위가 부분적으로 넓은 경우도 넓은 이행부위로 포함한 까닭이 아닌가 생각되며 이렇게 이행범위가 넓은 경우 MR상 골수 부종이 좀더 빈번하게 관찰되 었다 (Table 2). 그리 고 비록 통계적으로는 의의가 약하지만 침습정도가 공격적으로 보였던 거대세포종에서 MR상 골수부종이 많이 동반되었던 것 으로 (Table 4) 미루어 거대세포종의 단순 X선 사진상의 조직 학적 그리고 생물학적인 활성도와 MR 소견괴는 큰 연관성이 있을것으로생각된다.
결론적으로 사지골에서 발생된 양성 거대세포종에서도 MR 영상에서 종양주위에 골수부종을 흔히 동반하는 것을 관찰할 수 있었으며 (55.5%), 단순 X 선 사진에서 골파괴와 정/끓사 이의 이행범위가 넓은 경우 또 공격성향이 있을수록 MR 영상 에서 종양주위에 골수부종이 더 많이 나타나는것을알수있었 다.
참 고 문 헌
1. Beltran J, Simon DC, Katz W,et al. Increased MR signal inten sity in skeletal muscle adjacent to malignant tumors: pathologic correlation and clinical relevance. Radiology 1987; 162: 251-255 2. Moore SG, Bisset GS, Siegel MJ,et al. Pediatric musculoskeletal
MR imaging. Radiology 1991; 179: 345-360
3. Weatherall PT, Maale GE, Jayson H,et al. The confusing and classic MR appearance (abstract). Magn Reson Imaging 1990; 8 [suppl lJ: 134
4. Beltran J, Aparisi F, Bonmati LM,et al. Eosinophilic granuloma MRI manifestations. Skeletal Raiol 1993; 22: 157-161
5. Kroon HM, Bloem JL, Holscher HC. MR imaging of edema ac- companying benign and malignant bone tumors. Skeletal Radiol 1994;23: 261269
6. Yamamura S, Sato K, Sugiura J, et al. Prostaglandin levels of primary bone tumor tissues correlate with peritumoral edema demonstrated by MRI. Cancer 1997; 79: 255-261
7. Manaster BJ, Doyle AJ. Giant cell tumors of bone. Radio/ Clin North Am 1993;31(2):299-306
8. Vogler JB, Murphy WA. Bone marrow imaging. Radiology 1988
; 168: 679-693
9. Pay NT, Singer WS, Barrtal E. Hip pain in three children ac-
- 797 -
companied by transient abnormal [indings on MR images. Rad-
i% 양1 1989; 171: 147-149
10. Yaeger BA, Schiebler ML, Werthem SB,et a1. MR imaging of osteoid osteoma of the talus. J Comput Assist Tomogr 1987; 11 ‘
916-917
11. Crim JR, Mirra JM, Eckardt JJ, et a1. Wide spread inf1amma tory response to the osteoblastoma: the flare phenomenon. Rad- iology 1990; 177 : 835-836
12. Hanna SL, Magill HL, Brooks MT,et a1. Case o[ the day. Pedi- atric myositis ossificans circumscripta. RadioGraphics 199Q; 10 945-949
13. Pan G, Raymond AK, Carrasco CH,et a1. Osteosarcoma: MR imaging after preoperative chemotherapy. Radiology 1990; 174:
517-526
14. Yamamura S, Sato K, Sugiura H. Inflammatory reaction in chon- droblastoma. Skeletal Radiol 1996; 25 : 371-376
15. Hayes CW, Conway WF, Sundaram M. Misleading aggressive MR imaging appearance of some benign musculoskeletal lesios- n. RadioGraphics 1992; 12‘ 1119-1134
16. Beltran F, Chandnani V, McGhee RA,et a1. Gadopentetate dim- eglumine-enhanced MR imaging ‘ MR imaging of the muscul oskeletal system. AJR 1991; 156: 457-466
김성헌 오1: 앙성 거대세포종에서 종앙주위 걸수부종
17. Erlemann R, Reiser MF, Peters PE,et a1. Musculoskeletal neop- lasms: static and dynamic Gd-DTPA enhancing MR imaging Radiology 1989; 171 : 767-773
18. Hofmann S, Engel A, Neuhold A,et al: Bone-marrow edema syndrome and transient osteoporosis of the hip. J Bone Joint Surg 1993; 75(2): 210-216
19. Fertakos RJ, Swayne LC, Colston WC. Three-phase Bone Imag ing in BM edema of the Knee. Clin Nuc/ Med 1995; 20(7) 587-590
20. Hudson TM, Schiebler M, Springfìeld DS,et a1. Radiology of Giant Cell Tumors of Bone: Computed Tomography, Arthr。
Tomography, and Scintigraphy. Skeletal Radiol 1984; 11: 85-98 21. Levine E, Smet AD, Neff JR. Role of Radiologic Imaging in
Management Planning of Giant Cell Tumor of Bone. Skeletal Radiol 1984; 12: 79-89
22. Charkes ND. Mechanisms of skeletal tracer uptake. J Nuc/ Med 1979; 20 ‘ 794-795
23. Mclnerney DP, Middlemiss JH. Giant cell tumor of bone‘ Skel- etal Radiol 1978; 2: 195-204
24 이선규, 강흥식, 김주완 등 거대세포종의 자기공병영상 소견 신호강도 빛 형태학적 특성을 중심으로 대한방사선의학희지 1984;31(1):139-144
대한밤시선의학호|지 1998; 39 : 793-799
J Korean Radiol Soc 1998; 39 : 793-799
Peritumoral Bone Marrow Edema Accompan yin g Benign Giant Cell Tumor
1Sung-Hun Kim, M.D., Jeong-Mi Park, M.D., Ji-Yong Kim, M.D.,
Won-Hee Gi, M.D., Mi-Suk Sung, M.D., Jae-Mun Lee, M.D., Kyung-Sub Shin, M.D
1 Department of Radiology, The Calholic University of Korea
Purpose: To evaluate the frequency of peritumoral bone marrow(BM) edema accompanying be- nign giant cell tumor(GCT) of the appendicular bone by magnetic resonance(MR) imaging and to correlate MR1 findings with those of plain radiography and bone scintigraphy.
Materials and Methods: Eighteen cases of pathologically proven benign GCT of the appendicular bone were retrospectively analyzed using MR images, plain radiographs and bone scintigrams. A plain radiograph was available in 15 cases, and a scintigram in six. Marrow edema was defined as peritumoral signal changes which were of homogeneous intermediate or low signal intensity(S1) on T1 W1 and high S1 on T2WI, relative to the SI of normal BM, and homogeneous enhancement on Gd-DTP A-enhanced T1 WI. The transition zone, sclerotic margin and aggressiveness of the lesion were assessed on the basis of plain radiographs. BM edema seen on MR images was correlated with plain radiographic and scintigraphic findings.
Results: 1. Peritumoral BM edema was seen on MR images in 10 of 18 cases (55.5%). 2. 1n 8 of 15 cases for which plain radiographs were available, MR imaging revealed BM εdema. 1n six of these eight, transition zone was wide, while in two it was narrow. Six of seven patients without marrow edema showed a wide transition zone, and in one this was narrow. There was significant correlation between BM edema shown by MR imaging and the transition zone seen on plain radiographs (x2, p < 0.05). But The aggressiveness shown by plain radiographs correlated only marginally while the presence of sclerotic rim did not correlate. 3. All six cases for which a bone scintigram was available showed an extended uptake pattern. 1n five of the six, MR imaging revealed edema.
Conclusion: Peritumoral BM edema was frequently seen (55.5 %) in the GCTs of appendicular bone; it was more often shown in association with a wide transition zone by plain radiographs.
Index words: Bone marrow, MR Bone neoplasms, MR Bones, radiography
Address reprint requests to: Sung Hun Kim, M.D., Department of Radiology, St. Mary' s Hospital # 62 Youido-dong, Yongdungpo-gu SeouL 150-010 Korea Tel. 82-2-3779-1277 Fax.82-2-783-5288
799
국제 학술대회 일정표 [ 1 J
• International Congress on Imaging Science (1998/09/07 -11)
venue: University of Antwerp Antwerp, Belgium contact: M r. Jan de roeck, c/o Agfa-Gevaert N. V.,
Septestraat 27, B-2640 Mortsel, Belgium (tel: 32 - 3 μ47010; fax:32-3-4447485)
• Annual Meeting American College of Radiology (1998/09/12 -16)
venue: Pittsburgh, PA, USA
contact: John J. Curry, Ex. Dir., ACR, 1891 Preston White Drive, Reston, VA 20191-4397, USA (tel: 1 -703 - 6488900; fax: 1 - 703 - 6489176)
• 6th European Symposium on Uroradiology (1998/09/12 -16)
venue: Music and Convention Ctr. Strasbourg, France.
contact: Catherine Roy, Radiol. B, Chir. A-Hopita1 Civil, BP 426, F- Strasbourg Cedex, France
(tel:33-3-88116785; fax‘ 33-3-88116402)
• Organ Imaging Review (1998/09/13-19) venue: The Toronto Hilton Toronto, Ontario, Canada contact: Rya1s & Ass., Inc., P.O. Box 1925,
Roswell, GA 30077-1925, USA
(tel: 1-770-6419773; fax: 1-770-5529859)
• The Conf. on Cardiovascular & Interventional Radi- ology & Contrast Agents (1998/09/16 -17)
venue: donetsk Medical Univ. Donetsk, Ukraine contact: Dr. V.T. Djomin,
Lomonosova str. 33/43, Kiev, Ukraine 252022 (tel: 380-44-2637610; fax: 380 -44-2660108)
• 15th Ann. Mtg. Eur. Soc. for Magnetic Resonance in Medicine and Bio1ogy (1998/09/17-20)
venue: Hi1ton Noga Geneva, Switzerland contact: ESMRMB Secretariat,
Neu torgasse 9/2a, A-I 이
o
Vienna, Austria.(tel:43-1-5351306; fax:43-1-53340649)
• 20th International Congress of Radiology: Imaging in the Third Milennium (1998/09/19-23)
venue: Pragati Maidan New Delhi, India
contact: Dr. S.K. Aggarwal, Imaging Research Ctr., 10-B Kasturba Gandhi Marg, 110001 New Delhi, India.
(tel:91-11-3329887; fax:91-11-3713308)
• 11th QUADR. World Congress Int. Soc. of Radiog- raphers & Radiological techn. (1998/09/19 -23) venue ‘ Nippon Convention Center tokyo, Japan‘ contact‘ c/o The Japan Ass. of, Radiologica1technologists,
3-3-2 Minato, Chuo-ku, Tokyo 104, Japan (tel: 81 -3 - 35530155; 떠x: 81- 3 - 35533761)
• XXIV Congress & VIII Advanced Course of the Eur opean Soc. of Neuroradiology (1998/09/22-26) venue: Centro Cultural Belem Lisbon, Portugal contact: Mara Carletti, c/o MGR Congressi,
Via Servio Tullio 4, 1-20123 M ilano, Italy (tel:39-2-430071; fax:39-2-48008471)
• CIRSE ’98- Cardiovascular and Interventional Radio- logical Soc. of Europe (1998/09/27 -01)
venue ‘ Lido Venice, Italy contact: CIRSE 98
Pi1atusstrasse 14, CH-8032 Zuerich, Switzerland (te1:41-1-2622404; fax:41-1-2610578)
• 16th World Congress on Endo-Urology & Extrac- oporeal Shock Wave Lithotripsy (1998/10/00-00) venue ‘ Antwerp, Belgium.
contact: Dr. A.D. Smith, Long Island Jewish Med. Ct, 27005 76th Avenue, New Hyde Park Long Island, NY 11042, USA
(tel: 1-718-4707221/5; fax: 1-718-3438254)
• 23rd Annual San Diego Postgraduate Radiology Re- view Course (1998/10/00- 00)
venue: Hotel De1 Coronado San diego, CA, USA contact: ryals & Ass., Inc., P.O. Box 1925,
Roswell, GA 30077-1925, USA
(tel: 1-770-6419773; fax: 1-770-5529859)
• 18th Annual Comprehensive Review of Vascular and Interventional Radiology (1998/10/00 -00)
venue: Hotel Del Coronado San diego, CA, USA.
contact: ryals & Ass., Inc., P.O. Box 1925, Roswell, GA 30077-1925, USA
(tel: 1 -770-6419773; fax: 1 -770- 5529859)
• 11th Annual Meeting European Society of Head and Neck Radiology( Eshnr) (1998/10/01 -03)
venue: General Hospita1 Vienna, Austria contact: He1ga Fischer, AKH-University of Vienna,
Waehringer Guertel 18-20, A-1090 Vienna, austria (te1:43 -1 -404005801 ; fax: 43 - 1 -404003777)
• Muscu10skeletal MR (1998/10/05 -08) venue: The Ritz-Carlton Hotel Naples, FL, USA contact: Ryals & Ass., Inc., P.O. Box 1925,
Roswell, GA 30077-1925, USA.
(tel : 1 -770 - 6419773; fax: 1 -770 -5529859)
• 4th International Symposium on Cardiovascular &
Interventional Radiology (1998/10/05-09) venue: Hyatt Regency Cambridge, MA, USA
contact: Candace Cutler, CME Mngr., Brigham & Women’s Hosp., 75 Francis Street, Boston, MA 02115, USA (tel: 1-617-7326265; fax: 1-617- 7326509)
제공 : 대한방사선의학회 국제협력위원회
- 800 -