© Copyright
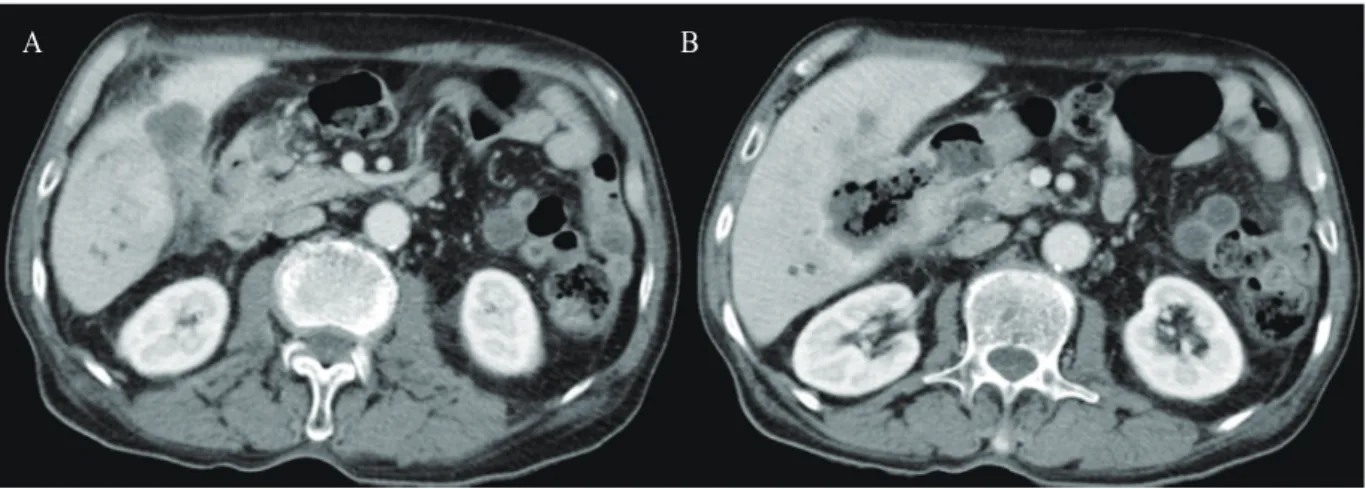
Squamous Cell Carcinoma of the Gallbladder Presenting with a Cholecystoduodenal Fistula
5
0
0
전체 글
(2)
(3)
(4)
(5)
수치
관련 문서
Distinction of basaloid squamous cell carcinoma from adenoid cystic and small cell undifferentiated carcinoma by immunohistochemistry. Basaloid squamous cell carcinoma of the
(A, B) The follow-up computed tomography scan reveals spontaneous regression of the lacrimal sac squamous cell carcinoma 15 months after the surgical biopsy (A: coronal view, B:
The left renal tumor was misdiagnosed as a renal abscess but finally diagnosed as squamous cell carcinoma metastasized from the intrahepatic bile duct.. The patient expired because
Results: Analyses on each tumor marker indicated that squamous cell carcinoma in the head and neck region had statistically significant correlation with p53, SCC-Ag(TA-4),
Basaloid squamous carcinoma of the uterine cervix is a rare tumor type characterized by an ulcerated, infiltrating growth pattern; nests or cords of small basaloid cells;
We herein report on an interesting case of vulval metastasis from squamous cell carcinoma of the cervix with an unusual clinical manifestation resembling lymphagioma
Acantholytic squamous cell carcinoma is a well-defined variant of squamous cell cancer in which significant portions of the neoplastic proliferation show a pseudoglandular or tubular
Extensive squamous metaplasia simulating squamous cell carcinoma in benign breast papillo- matosis.. Significance of squamous cells in fine nee- dle aspiration
