Composite Neuroendocrine Carcinoma with Adenocarcinoma of the Stomach Mimicking Double Primary Cancer
4
0
0
전체 글
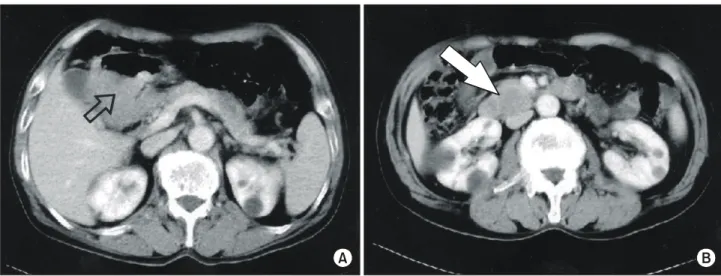
(2) 322. 대한외과학회지:제 70 권 제 4 호 2006. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. A. B. Fig. 1. Preoperative contrast-enhanced axial CT scan demonstrated (A) a huge, exophytic mass in the prepyloric antrum of the stomach (open arrow) and (B) a 4×3 cm sized, ovoid mass just distal to the ampulla of Vater (white arrow).. huge ulcerofungating and infiltrative lesion in the gastric antrum and an ulcerative lesion in the duodenal second portion. Biopsy from the gastric portion of the tumor revealed adenocarcinoma whereas that from the duodenal portion revealed neuroendocrine carcinoma. Contrast-enhanced axial CT scan demonstrated a huge, exophytic mass in the prepyloric antrum of the stomach and a 4×3 cm sized, ovoid mass just distal to the ampulla of Vater (Fig. 1). Following a diagnosis of a double primary cancer of the stomach and periampullary area, pancreaticoduodenectomy with lymph node dissection was performed. Gross examination of the surgical specimen showed an ulcerofungating tumor, measuring 8.5×7.5×4.5 cm to be present in the antrum of the stomach (Fig. 2). The tumor extended to the serosa with bulging out appearance. A well-demarcated ovoid mass was noted in the peripancreatic area, measuring 4×3×3 cm. The overlying duodenal mucosa was ulcerated, and the tumor involved duodenal wall and pancreatic parenchyma. Microscopically, the gastric tumor was composed of well to moderately differentiated adenocarcinoma (CEA; positive, cytokeratin; strong positive, CD56, chromogranin and synapatophysin; negative) and solid sheets of poorly differentiated neuroendocrine carcinoma (cytokeratin; dot-like focal positive, CD56, chromogranin and synapatophysin; strong positive, CEA; negative) (Fig. 3). The Ki67 labeling index (MIB-1) of the small cell carcinoma-. Fig. 2. The cut surface of the primary tumor of the stomach showed an ulcerofungating, huge tumor with exophytic growth to be present in the gastric antrum.. tous components was higher (24.5%) rather than that of adenocarcinomatous components (8.5%). Intermingled or transitional areas of the two tumor components were noted, supporting the diagnosis of composite neuroendocrine carcinoma with adenocarcinoma (mixed exocrine-endocrine carcinoma), with extension to serosa, no vascular tumor emboli, no lymph nodes metastasis (0/29), and clear resection margins. The microscopic features and immunohistochemical profiles of the peripancreatic mass were similar to those of the neuroendocrine carcinoma of the stomach, confirming the diagnosis of a metastatic tumor of neuroendocrine carcinoma component of.
(3) Jin Young Seo, et al:Composite Neuroendocrine Carcinoma with Adenocarcinoma of the Stomach Mimicking Double Primary Cancer. 323. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. A. C. the stomach, with involvement of duodenal wall and pancreatic parenchyma. The postoperative course was uneventful and the patient was discharged without complications. DISCUSSION. It is well known that neuroendocrine carcinomas are occasionally accompanied by adenocarcinomas in the gastrointestinal tract.(1-12) Morphologically, such lesions are classified into two subgroups: compositetype tumors, in which both components appear to be mixed haphazardly,(1-5) and collision-type tumors, which are considered as double tumors with a “side by side” or “one upon another” pattern.(5,6) In this case, the gastric tumor consisted of two different components, one being a well to moderately differentiated adenocarcinomatous area, and the other being a small cell endocrine carcinomatous area composed of a diffuse proliferation of atypical. B Fig. 3. The microscopic features and immunohistochemical profiles of the gastric tumor confirmed the diagnosis of composite neuroendocrine cell carcinoma with adenocarcinoma. (A) The gastric tumor was composed of well to moderately differentiated glandular component and solid sheet of poorly differentiated carcinoma component (×40, hematoxylin and eosin staining). (B) Cytokeratin staining demonstrated diffusely positive in the cytoplasm of the glandular component and focally positive in the solid component with dot-like appearance (×200). (C) Chromogranin and synapatophysin staining showed diffusely positive in the cytoplasm of the solid component, but negative in the glandular component (×200).. round-to-oval cells in a sheet fashion. The tumor cells in the small cell carcinomatous component were immunoreactive to chromogranin and synaptophysin, which indicated that the tumors were neuroendocrine in nature. Furthermore, a histological gradual transition was also observed between the adenocarcinomatous area and the neuroendocrine carcinomatous area. These findings thus indicated the present tumor to be a composite glandular-neuroendocrine carcinoma of the stomach. The microscopic features and immunohistochemical profiles of the peripancreatic mass were similar to those of the neuroendocrine carcinoma of the stomach. Therefore, this should be diagnosed as a metastatic tumor of neuroendocrine carcinoma component of the stomach. Composite glandular-endocrine tumors are rare and are evenly divided between well-differentiated and poorly-differentiated types.(1-5) Composite tumors occur in patients from 32 to 74 years of age and.
(4) 324. 대한외과학회지:제 70 권 제 4 호 2006. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. involve the gastric antrum and body to an equal extent. The histogenesis of composite tumors is unclear, but both types of carcinoma may be derived from the same cell, most likely a pluripotent stem cell or an adenocarcinoma precursor cell as opposed to a preexisting neuroectodermal cell.(1-5) In this case, two possible mechanisms might account for the mixed histologic character of the present tumor. A malignant transformation of a common dysplastic epithelial cell could have produced both adenocarcinoma and neuroendocrine carcinoma. Alternatively, a malignant transormation of dysplastic epithelial cells may have resulted in adenocarcinoma, a part of which then further differentiated into neuroendocrine cell component. The preoperative diagnosis of this case was a double primary cancer of the stomach and periampullary area; upper gastrointestinal endoscopy and contrastenhanced axial CT scan demonstrated two separate tumors in the gastric antrum and the duodenal second portion. Furthermore, biopsies from these two separate tumors revealed adenocarcinoma and neuroendocrine carcinoma, respectively. However, the microscopic features and immunohistochemical profiles of the resected specimen confirmed the diagnosis of the composite neuroendocrine carcinoma with adenocarcinoma of the stomach (mixed exocrine-endocrine carcinoma) and a metastatic tumor of neuroendocrine carcinoma component of the stomach in the duodenal area and pancreatic parenchyma. We report a case of the composite neuroendocrine carcinoma with adenocarcinoma of the stomach (mixed exocrine-endocrine carcinoma), in which upper gastrointestinal endoscopy with biopsies and contrastenhanced axial CT scan suggested the diagnosis of a double primary cancer, preoperatively.. REFERENCES 1) Fukui H, Takada M, Chiba T, Kashiwagi R, Sakane M,. 2). 3) 4). 5). 6). 7) 8). 9). 10). 11). 12). Tabata F, et al. Concurrent occurrence of gastric adenocarcinoma and duodenal neuroendocrine cell carcinoma: a composite tumour or collision tumours? Gut 2001;48: 853-6. Roger LW, Murphy RC. Gastric carcinoids and carcino-mas: morphologic correlates of survival. Am J Surg Pathol 1979; 3:195-202. Ulich TR, Kollin M, Lewin KJ. Composite gastric carcinoma. Arch Pathol Lab Med 1988;112:91-3. Levendoglu H, Cox CA, Nadimpalli V. Composite (adenocarcinoid) tumors of the gastrointestinal tract. Dig Dis Sci 1990;35:519-25. Yamashina M, Flinner RA. Concurrent occurrence of adenocarcinoma and carcinoid tumor in the stomach: a composite tumor or collision tumors? Am J Clin Pathol 1985;83: 233-6. Corsi A, Bosman C. Adenocarcinoma and atypical carcinoid: morphological study of a gastric collision-type tumour in the carcinoma-carcinoid spectrum. Ital J Gastroenterol 1995;27:303-8. Lattes R, Grossi C. Carcinoid tumors of the stomach. Cancer 1956;9:698-711. Baudin E, Gigliotti A, Ducreux M, Ropers J, Comoy E, Sabourin JC, et al. Neuron-specific enolase and chromogranin A as markers of neuroendocrine tumours. Br J Cancer 1998; 78:1102-7. Yamamoto J, Abe Y, Nishihara K, Katsumoto F, Takeda S, Abe R, et al. Composite glandular-neuroendocrine carcinoma of the hilar bile duct: report of a case. Surg Today 1998; 28:758-62. Tsujii T, Kambara T, Shimizu K, Tsubaki M, Kamai T, Abe H, et al. Adenocarcinoma with extensive neuroendocrine differentiation arising in an ileal diverticulum: report of a case. Surg Today 2002;32:439-42. Owen NJ, Sohaib SA, Peppercorn PD, Monson JP, Grossman AB, Besser GM, et al. MRI of pancreatic neuroendocrine tumours. Br J Radiol 2001;74:968-73. Kim YH, Oh ST, Jung DH, Yook JH, Kim BS, Park GC. Clinicopathologic characteristics of neuroendocrine tumor of the stomach. J Korean Surg Soc 2000;58:650-5..
(5)
수치

관련 문서
Since the two countries have established diplomatic relations in 1992, the trade between Korea and China has been developing rapidly, By the end of 2006, Korea
This report, therefore, analyses two important policy issues: (1) the appropriateness of the government allocated GHG reduction targets by sector and industry; (2) the
Relationship between lymph node metastasis and lymphatic invasion, diagnosed by immunohistochemical staining and H&E staining in gastric
Type 2 The number of lines degenerate to a point but there is no degeneration of two dimensional phase regions.. Non-regular two-dimensional sections.. Nodal plexi can
Average of the indexed values of the following data: (1) Total value of the indexed score for disability-adjusted life years (the number of years lost due to illness,
현재 간암(Hepatocellular carcinoma) 1차치료제, 대장암(Colorectal cancer) 3차 치료제, 위암(Gastric cancer) 2차 치료제, 선양낭성암(Adenoid cystic
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
Patients with breast cancer; ovarian cancer; renal cell carcinoma; pancreatic neuroendocrine cancer; colorectal cancer; head and neck cancer; non-small cell lung
