DOI : 10.3341/jkos.2008.49.10.1611
당뇨황반부종의 빛간섭단층촬영 분류에 따른 트리암시놀론 안내주입술의 효과
윤상철․이대영․남동흔 가천의과학대학교 안과학교실
목적: 빛간섭단층촬영을 통하여 분류한 당뇨황반부종의 유형별 술 전 인자를 파악하고 유리체내 트리암시놀론 주입술 후 유형별 단기치료효과, 유형변화를 분석하고자 하였다.
대상과 방법: 임상적으로 유의한 황반부종이 관찰된 성인 60명 77안을 대상으로 OCT를 통해 제1형(균질 반사도의 황반부종), 제2형(망막외층에 저 반사도를 가진 황반부종), 제3형(장액성 황반박리)로 분류하였다. 각 군간 나이, 성 별, 당뇨유병기간, 시력저하기간과 술 전과 술 후 1달째 최대교정시력, 안압, 황반부 두께 및 전체부피, 유형변화를 비 교하였다.
결과: 당뇨유병기간은 3형이 짧았으며 술 전 시력은 1형이 2, 3형에 비해 높았다. 황반부 두께, 전체부피는 1, 2, 3형 순으로 두꺼워졌다. IVTA 후 2, 3형은 시력 호전을 보였다. 황반부 두께, 전체 부피는 모든 군에서 감소했으나 변화 량은 1형보다 2, 3형이 유의하게 컸다. 2, 3형의 경우 IVTA 후 1형으로 유형이 변하는 비율은 74%, 83%였다.
결론: OCT에 의한 당뇨황반부종 유형에 따라 IVTA 치료효과가 차이가 있었다. 이를 통해 IVTA 치료효과를 예측하여 치료의 객관화 확립에 도움이 될 것으로 생각된다.
<대한안과학회지 2008;49(10):1611-1618>
<접수일 : 2007년 10월 2일, 심사통과일 : 2008년 7월 2일>
통신저자 : 남 동 흔
인천시 남동구 구월동 1198 가천의과학대학교 길병원 안과 Tel.: 032-460-3364, Fax: 032-460-3358 E-mail: [email protected]
당뇨망막병증은 당뇨병성 신증, 당뇨병성 신경병증 과 함께 3가지 중요한 당뇨 미세혈관 합병증 가운데 하 나이다. 전세계적으로 매년 당뇨 유병률은 높아지고 있 으며 이에 따라 당뇨망막병증 환자도 증가하는 추세여 서 그 중요성이 더해지고 있다. 당뇨망막병증 소견으로 는 망막출혈, 경성 삼출물, 미세혈관류, 황반부종 등이 있으며 특히 황반부종은 당뇨망막병증 환자에 있어 시 력저하의 가장 흔한 원인으로 알려져 있다.1
임상적으로 황반부종은 안저검사상 황반중심에서 1 유두지름(1,500 µm)을 반지름으로 하는 원 안에서 두 꺼워진 망막이나 경성삼출물이 관찰되는 경우를 말하며 이를 진단하기 위해서는 현재까지는 검안경과 세극등으 로 안저검사를 시행하는 방법을 사용하여 왔다.2 하지 만 이러한 방법으로는 황반두께의 객관적, 정량적 평가 를 할 수 없었다. 당뇨황반부종의 치료시기와 방법 결
정 및 치료 효과판정을 위해 황반부종을 조기에 진단하 고 형태적, 정량적으로 평가하는 것이 중요하므로3 이 를 위해 망막두께분석기(retinal thickness analy zer, RTA),4,5 망막단층촬영기(heidelberg retina tomography, HRT),6 빛간섭단층촬영기(optical coherence tomography, OCT)7,8 등을 사용하여 황반부종의 정량화 및 다양한 형태학적 분류를 시도하 였다. 이 중 OCT는 다른 검사들에 비해 민감도가 매우 높고 굴절력의 영향을 적게 받으며 정량적인 측정과 망 막내 구조파악이 가능하다는 장점이 있어 망막두께 측 정에 널리 쓰이고 있다.7-9 이러한 장점들을 이용하여 Otani et al10은 형태적 차이에 따라 3가지 유형으로 당뇨황반부종을 분류하였고 Kang et al11은 OCT의 형태학적인 분류와 형광안저촬영 소견에 따른 분류와의 연관성이 있음을 밝혔으며 이를 통하여 당뇨황반부종의 해부학적, 생리학적 특성을 알아보고자 하였다. 또한 미만성 당뇨황반부종의 OCT 유형별 위험인자 차이에 대해 Kim et al12은 미만성 당뇨황반부종을 OCT로 분류한 뒤 각각 유형별로 위험인자의 차이를 분석하였 지만 위험인자들과 유형간의 인과관계는 밝히지 못하였 고 연관성만 제시하는 한계가 있었다.
당뇨황반부종의 치료는 황반부종의 원인 및 병태생
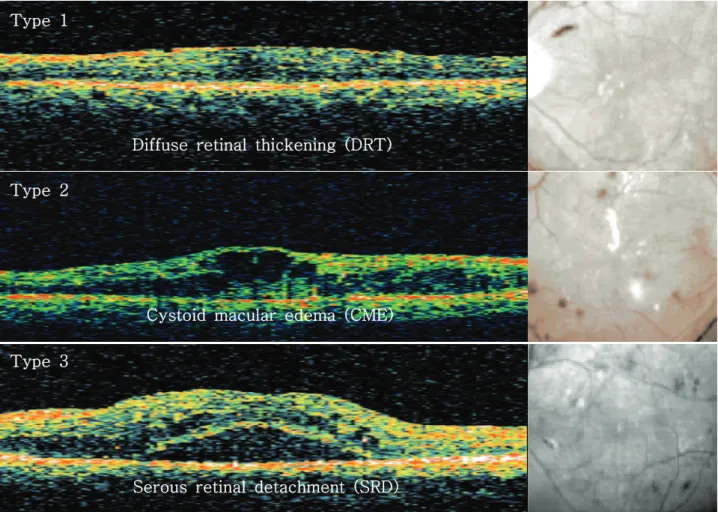
Diffuse retinal thickening (DRT) Type 1
Cystoid macular edema (CME) Type 2
Serous retinal detachment (SRD) Type 3
Figure 1. The classification of clinically significant diabetic macular edema by OCT features. Type 1 (top): the thickening of the fovea with homogeneous optical reflectivity throughout the whole layer of the retina. Type 2 (middle): the thickening of the fovea with markedly decreased optical reflectivity in the outer retinal layer. Type 3 (bottom): the foveolar detachment without vitreofoveal traction; OCT=optical coherence tomography.
리학적 기전에 따라 유리체내 트리암시놀론 주입술 (intravitreal triamcinolone injection, IVTA), 항혈관내피성장인자 항체 주입술(Anti-VEGF anti body injection), 유리체절제술(pars plana vitrec tomy, PPV) 등이 시도되고 있으나 아직까지 명확히 정립된 치료방법은 없는 실정이다. 이 중 유리체내 트 리암시놀론 주입술을 통해 당뇨황반부종을 성공적으로 치료했다는 여러 보고들이 있은 다음 당뇨황반부종 치 료에 널리 사용되고 있으며 많은 연구들이 진행되었
다.13-15 OCT로 측정한 당뇨황반부종의 유형별 IVTA
의 효과에 대한 여러 연구가 있었으며 이 중 Brasil et al16은 IVTA 단기치료효과 및 예측인자에 대한 연구를 하였으나 술 후 OCT로 측정한 황반부 변화에 대한 내 용은 없었다. 또한 Kim et al17은 IVTA 전, 후 당뇨 황반부종의 유형별 시력 및 황반두께변화에 대한 연구 를 하였지만 본 연구에 비해 대상환자수가 적고 술 후 유형변화에 대한 비교는 없었다.
본 연구는 OCT를 통해 분류한 당뇨황반부종의 유형 별 술 전 인자를 분석하여 각 유형별 차이를 비교해 보 았으며 IVTA 전, 후 여러 비교인자들과 황반두께의 변 화를 분석하여 유형별 단기치료효과를 평가하고 술 후 유형변화를 통해 이를 통해 정량화, 객관화된 당뇨황반 부종의 치료방법을 제시하고자 하였다.
대상과 방법
2006년 5월부터 2007년 1월까지 본원 안과에 내원 한 인슐린 비의존성 당뇨병환자에서 안저검사 및 형광 안저촬영상 임상적으로 유의한 황반부종이 관찰되며 레 이저나 다른 특별한 치료를 시행하지 않은 환자 중 치 료목적으로 IVTA를 시행한 60명 77안을 대상으로 하 였고 이전에 안내수술을 받았거나 다은 유리체망막병이 동반된 경우, 매체의 혼탁이 심하거나 OCT 소견상 주 된 유형없이 여러 소견이 혼재된 경우는 대상에서 제외
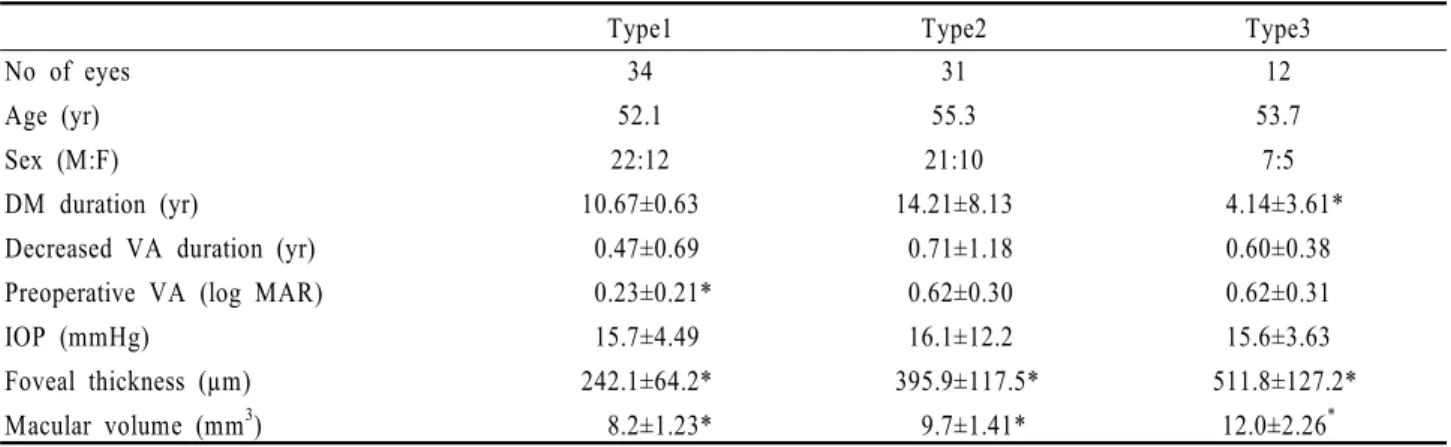
Type1 Type2 Type3 No of eyes
Age (yr) Sex (M:F) DM duration (yr)
Decreased VA duration (yr) Preoperative VA (log MAR) IOP (mmHg)
Foveal thickness (µm) Macular volume (mm3)
34 52.1 22:12 10.67±0.63 0.47±0.69 0.23±0.21*
15.7±4.49 242.1±64.2*
8.2±1.23*
31 55.3 21:10 14.21±8.13 0.71±1.18 0.62±0.30 16.1±12.2 395.9±117.5*
9.7±1.41*
12 53.7
7:5 4.14±3.61*
0.60±0.38 0.62±0.31 15.6±3.63 511.8±127.2*
12.0±2.26*
* Krusckal-Wallis test: p<0.05; VA=visual acuity; IOP=intraocular pressure.
Table 1. Basic characteristics of eyes with different OCT types 하였다.
빛간섭단층활영은 STRATUS OCT 3 (version 4.0, Carl Zeiss, California, USA)의 fast macu lar mode)를 이용하여 검사하였다. 한 명의 연구자의 의해 fast macular mode의 6장 스캔사진으로 단면 구조를 분석하여 당뇨황반부종을 형태적으로 분류하였 다. 당뇨황반부종의 분류는 Kang et al11의 분류를 일 부 변형하여 제1형은 망막전층에 걸쳐 균질의 반사도를 가진 황반부종, 제2형은 망막외층에 현저하게 감소된 반사도를 가진 황반부종, 제3형은 유리체황반견인이 동 반되지 않은 장액성 황반박리로 하였으며 망막전막이나 유리체황반견인이 동반된 경우는 본 연구에서 제외하였 다(Fig. 1).
IVTA는 Triamcinolone acetonide (트리암시놀 론 주®, 동광제약)을 4 mg/0.1 ml 농도로 유리체내 주입하였으며 IVTA 전 비교 요인으로는 나이, 당뇨유 병기간, 시력저하기간, 최대교정시력, 안압, OCT로 측 정한 지름 1 mm의 중심와 두께(foveal thickness) 와 전체 황반부 부피(total macular volume) 이며 이중 최대교정시력과 황반부 두께, 전체부피와 각각의 변화량은 술 전과 술 후의 차이를 비교하였다.
통계분석은 S-link 2.2를 사용하였으며 제 3형의 경우 대상이 12명밖에 되지 않아 비모수적인 방법을 사 용하였다. 각 그룹간에 차이가 있는지 알아보기 위하여 Kruskal Wallis test와 Wilcoxon’s signed rank test를 시행하였고 결과는 평균±표준오차(mean±
tandard error; SE)로 표시하였다. P값이 0.05 미 만일 경우를 통계학적으로 의미 있다고 판정하였다.
결 과
대상군 60명 77안 중 제 1형은 34안(44%), 2형은 31안(40%), 3형은 12안(16%)이었다. 환자들의 평균
나이와 시력저하기간, 안압은 세 군간의 차이는 없었으 나 당뇨유병기간은 3형이 1, 2형에 비해 통계적으로 유 의하게 짧았으며(Kruskal-wallis test, p<.01) 술 전 시력의 경우 1형이 2, 3형에 비해 의미 있게 양호하 였다(Kruskal-wallis test, p<.01). 술 전 황반부 두께는 제 1, 2, 3형에서 각각 242.1±64.2 µm, 395.9 ±117.5 µm, 511.8±127.2 µm로 각 그룹간 유 의한 차이가 있었으며(Kruskal-wallis test, p<.05) 전체 황반부부피도 1형이 8.20±1.23 mm3으로 가장 얇고 2형 9.74±1.41 mm3, 3형 12.0±2.26 mm3순으 로 두꺼웠으며 각 군간 통계적으로 유의한 차이가 있었 다(Kruskal-wallis test, p<.05)(Table 1).
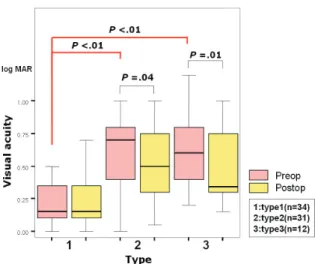
IVTA 전 후 최대교정시력의 차이는 1형의 경우 차 이가 없었으나 2, 3형의 경우 통계적으로 유의한 호전 을 보였다(Wilcoxon’s signed rank test, p=.45, p=.04, p=.01)(Fig. 2). IVTA 후 모든 군에서 황반 부 두께가 의미있게 감소하였으나(Wilcoxon’s signed rank test, p=.002, p<.0001, p=.0001) 그 변화 량을 비교해 보았을 때 1형의 변화량에 비해 2, 3형의 변화량이 유의하게 차이가 났으며 2, 3군간의 변화량의 차이는 없었다(Kruskal-wallis test, p<.01, p<.01, p=.40)(Fig. 3). 황반부 전체부피의 경우에도 IVTA 후 모든 군에서 의미있는 감소를 보였고(Wilcoxon’s signed rank test, p=.0002, p<.0001, p=.0001) 변화량 비교시 1형의 변화량에 비해 2, 3형의 변화량이 유의하게 크고 2, 3형간의 차이는 없었다(Kruskal- allis test, p=.02, p<.01, p=.10). 이는 황반부 두 께 변화양상과 동일하였다(Fig. 4).
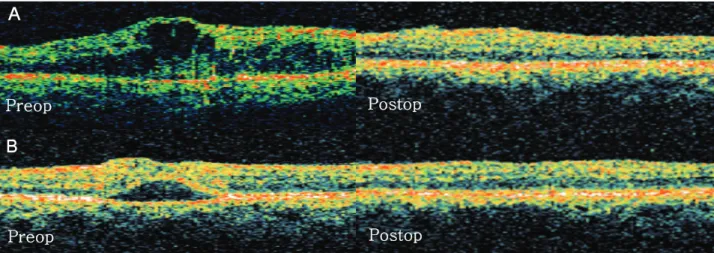
IVTA 후 1달뒤 측정한 OCT 검사상 2, 3형의 황반 부종 환자 중 대부분에서 유형변화가 관찰 되었다. 2형 의 경우 74%에서 IVTA 후 1형으로 유형이 변하였으 며 3형의 경우에는 83%에서 1형으로 유형이 변화하였 다(Fig. 5).
Figure 2. An analysis of the VA before and after IVTA.
Pre-operative VA was significantly higher in type 1 than in types 2 and 3 (Kruskal-Wallis test=p<.01, with p<.05 regarded as significant). VA after IVTA improved significantly in types 2 and 3 (Wilcoxon’s signed rank test, p=.04, p=.01, with p<.05 regarded as significant); VA=visual acuity;
IVTA=intravitreal triamcinolone acetonide injection; log MAR=the logarithm of the minimum angle of resolution.
Figure 3. An analysis of the foveal thickness before and after IVTA. Foveal thickness significantly decreased in every types (Wilcoxon’s signed rank test, p=.002, p<.0001, p=.0001, with p<.05 regarded as significant). But the extent of changes in Types 2 and 3 was greater than in Type 1 (Kruskal-Wallis test p<.01, with p<.05 regarded as significant).
Figure 4. An analysis of total macular volume before and after IVTA. Total macular volume was significantly decreased in every types (Wilcoxon’s signed rank test, p=.0002, p<.0001, p=.0001, with p<.05 regarded as significant). But the extent of changes in Types 2 and 3 was greater than in Type 1 (Kruskal-Wallis test p<.01, with p<.05 regarded as significant).
고 찰
당뇨황반부종을 진단하는 기존의 방법으로 형광안저 촬영과 안저검사를 사용하였다. 형광안저촬영은 혈관누 출의 양상을 파악하여 국소형과 확산형으로 당뇨황반부 종을 분류하였으나 형광안저촬영은 주관적이며 정량적
인 측정이 불가능하고 형광물질의 누출양과 시력예후와 는 상관관계가 없으며 형광누출이 없는 경우에도 시력 저하와 황반부종이 나타나는 등의 한계점이 있었다.18 따라서 정확하고 객관적, 정량적인 망막두께의 변화를 파악하기 위한 새로운 방법으로 OCT를 사용하게 되었 다. OCT를 통해 망막내부구조 파악과 당뇨황반부종에 대한 정량적이고 객관화된 평가를 할 수 있게 되었으며 이러한 장점들을 이용하여 당뇨황반부종의 형태학적 분 류가 가능하게 되었다.
형태학적인 분류 방법으로는 Otani et al10이 사용 한 3가지 형태로 분류하는 방법이 가장 널리 쓰이고 있 으며 연구자마다 이를 세부적으로 응용해서 3~5개의 유형으로 분류한 연구들도 있다.11,16,19 기존 연구들의 형태별 유병률을 보면 Otani et al과 Kim et al의 연 구에서는 1형(망막전층에 걸쳐 균질의 반사도를 가진 황반부종)은 88~97%, 2형(망막외층에 현저하게 감 소된 반사도를 가진 황반부)은 47~55%, 3형(유리체 황반견인이 동반되지 않은 장액성 황반박리)은 7~15
% 였다.10,19 하지만 Brasil et al의 연구에 의하면 1 형은 57.5%, 2, 3형은 각각 47.9%, 20.5%으로 차이 가 있었으며 본 연구에서는 1형, 2형, 3형 각각 44%, 40%, 16%로 이와 가까운 결과를 보였다.16 이러한 유 병률의 차이를 보이는 이유로는 우선 Otani et al은 두가지 이상의 형태가 중복되어 나타나는 경우 각각의 형태를 모두 빈도에 포함시켰으므로 1형의 유병률이 높 아졌다고 보여진다. 또한 본 연구는 IVTA를 받은 환자 들만 대상으로 하였으므로 전체적인 당뇨황반부종 환자
B Preop
Preop
Postop
Postop A
Figure 5. DME pattern changes before and after IVTA injection at 1 month. The OCT feature changed to diffuse thickened macula (Type 1) in (A) 74% of cystoid macular edema (Type 2), (B) 83% of serous retinal detachment (Type 3); DME=diabetic macular edema; OCT=optical coherence tomography.
의 유병률과는 차이가 있을 수 있으며 이는 선택편위 (Selection-bias)의 가능성을 시사한다. 본 연구와 Brasil et al은 OCT3를 사용하였으나 Otani et al 과 Kim et al은 구기종인 OCT2를 사용하였기에 OCT3의 높은 해상도에 의해 파악되는 작은 낭종들을 가진 2형을 1형으로 잘못 분류했을 가능성도 있다.
당뇨황반부종의 유발기전은 아직 명확하게 밝혀지지 는 않았으나 현재까지 알려진 바로는 내측혈액망막장벽 인 모세혈관 내피세포층의 손상을 입어 그 결과 혈관의 투과성의 증가로 발생한다고 한다.20,21 망막의 허혈성 변화가 오면 세포독성부종(cytotoxic edema)이라 불 리는 뮐러세포의 팽창이 유발되고 prostaglandin과 VEGF 같은 망막혈관투과성 증가를 일으키는 성장인 자들의 분비 증가로 인해 혈관인성부종(vasogenic edema)으로 진행하게 된다.20,22,23 지속되는 부종과 허혈은 뮐러세포와 주변신경조직에 액상괴사(liquefa ction necrosis)를 유발하며 이는 망막외층에 낭포를 생성한다.24,25 이외에도 망막색소상피층의 이상과 유리 체 견인 등도 당뇨황반부종의 발생에 관여하는 것으로 알려져 있다.26,27
Kang et al11은 당뇨황반부종의 OCT 분류와 병인 론을 연관지어 살펴보았으며 1형은 형광안저촬영의 국 소형과 연관이 있고 이는 미세혈관류에서 발생한 국소 누출에 기인하는 것으로 보이며 2형과 3형은 확산형과 가깝고 망막혈관의 투과성 증가가 있는 경우 발병율이 높아짐을 확인한 바 혈관투과성 증가로 인하여 발생한 다고 하였다. 그리고 3형은 2형의 선행병변으로 생각된 다고 가정하였고 그 근거로 황반부박리가 낭포성 황반 변화를 유발한다는 기존의 연구 결과와 3형에 비해 2형 이 시력이 저하되었고 황반두께도 더 두껍다는 것을 제
시하였다.28,29 본 연구에서도 2형에 비해 3형이 통계적 으로 유병기간이 짧다는 것을 볼 때 이 가설이 의미가 있다고 보여진다. 하지만 시력은 유형보다는 황반부 두 께와 연관성이 있으며 3형의 경우 기존의 모든 연구에 서 표본수가 17개 이하로 적다는 것을 볼 때 단지 저하 된 시력과 두꺼운 황반부가 더 진행된 당뇨황반부종의 근거라 보기 어려운 점이 있어 이에 대한 추가적인 연 구가 필요할 것으로 생각된다.10,19,30,31
본 연구에서 IVTA 전 후 최대교정시력을 비교해 본 결과 1형의 경우 IVTA 후 시력호전을 보이지 않지만 2, 3형의 경우 통계적으로 유의한 향상을 보였다. 이는 당뇨황반부종의 병인에 따른 IVTA 치료 효과의 차이 로 볼 수도 있다. 하지만 Brasil et al16과 Jonas et al32 연구에 의하면 당뇨황반부종의 유형이 같더라도 IVTA 전 시력이 저하되어 있을수록 IVTA 후 시력은 더 많이 향상된다고 하였고 이는 단지 유형에 따른 차 이뿐만 아니라 저하된 술 전 시력 때문에 2, 3형에서 더 좋은 시력 호전을 보인것이라 생각된다. 이러한 점 들을 고려할 때 당뇨황반부종의 유형이 2, 3형이며 술 전 시력이 저하될수록 IVTA 후 시력향상이 클 것이라 고 예상할 수 있다.
황반부 두께와 부피의 경우 본 연구에서는 IVTA 후 모든 유형에서 통계적으로 의미 있는 감소를 보였다.
하지만 감소량을 비교해 보았을 때 1형에 비해 2, 3형 의 변화량이 통계적으로 의미 있게 큰 것을 알 수 있었 으며 2, 3형간의 차이는 없었다. 이는 IVTA가 황반부 두께와 부피 감소에 모든 유형에서 효과적이나 유형에 따라 차이가 있으며 이러한 원인으로는 술 전 두께 차 이이거나 당뇨황반부종의 병인의 차이로 생각된다.
IVTA 후 재측정한 OCT에서 2, 3형의 당뇨황반부
종이 1형으로 유형 변화가 관찰되었다. 이는 트리암시 놀론이 혈액망막장벽의 투과성증대를 효과적으로 억제 하여 낭포성 변화나 장액성 박리는 사라지고 미세혈관 류에서 발생하는 국소적인 누출만 남은 1형의 형태로 변하는 것으로 생각된다.
본 연구는 IVTA 후 최소 3개월 이후 최대교정시력 과 황반부 두께 및 부피를 측정한 타 연구들과 달리 IVTA 후 1개월째 결과를 비교하여 추적관찰의 기간이 짧다는 것이 한계점이 될 수 있다. 하지만 트리암시놀 론의 반감기가 2.75개월이며 단기 치료효과를 연구한 기존보고들을 보면 술 후 1개월의 결과와 3개월의 결과 의 차이가 미미하다는 점을 볼 때 결과의 신뢰도에 영 향을 주지 않을 것으로 보인다.33
본 연구를 포함하여 현재까지 밝혀진 연구결과들을 종합하여 당뇨황반부종의 객관화된 치료방법을 제시할 수 있을 것이다. 형광안저촬영상 국소형이면서 OCT 검사에서 균질성 중심와부종(본 연구의 1형)의 경우 국 소누출을 차단하는 황반광응고술을 초치료로 시도해 볼 수 있으며 형광안저촬영상 확산형이면서 OCT 유형이 망막외층에 현저하게 감소된 반사도를 가진 황반부종 (본 연구의 2형)이나 유리체황반견인이 동반되지 않은 장액성 황반박리(본 연구의 3형)은 IVTA를 우선적인 치료로 선택할 수 있을 것이다. Kang et al34의 연구 결과에 따르면 확산형 당뇨황반부종 환자에서 IVTA 시행한 뒤 3주 후 황반광응고술을 시행한 결과 시력향 상과 재발감소를 보였다. 이를 본 연구 결과와 함께 적 용해 보면 IVTA 후 OCT 검사상 유형이 1형으로 변화 된 것을 확인한 후 황반광응고술을 시행할 경우 시력호 전, 황반부종의 감소 및 재발억제에 효과적이라 생각되 며 IVTA 후 1형으로 변화되지 않은 채 2, 3형이 지속 되면서 재발하는 경우 IVTA 재주사를 고려해 볼 수 있 다. 그리고 유리체황반견인이 동반된 황반부종의 경우 유리체절제술을 통한 견인력의 제거가 효과적인 치료라 생각된다.35
결론적으로 최대교정시력이 낮을수록 IVTA 후 시력 호전이 양호하였고 술 전 OCT 검사상 2, 3형이 1형에 비해 IVTA 후 황반부종의 감소와 시력증가에 뛰어난 효과가 있었다. IVTA 전 최대교정시력과 OCT 검사 상 당뇨황반부종 유형 파악으로 IVTA효과를 술 전에 미리 예측할 수 있으며 더 나아가 유형에 따른 정확하 고 정량화, 객관화된 치료방법을 선택함으로써 효과적 으로 당뇨황반부종을 치료할 수 있을 것으로 생각된다.
참고문헌
1) Klein R, Klein BE, Moss SE, et al. The Wisconsin
epidemiologic study of diabetic retinopathy IV: Diabetic macular ede ma. Ophthalmology 1984;91:1464-74.
2) Johnson RN, Howard SH, McDonald R, Ai E. Fluorescein angiography: basic principles and interpretation. In : Ryan SJ, ed. Retina, revised. St. Louis: Mosby, 2001; v. 2. chap. 55.
3) Early Treatment Diabetic Retinopathy Study Research Group.
Early Treatment Diabetic Retinopathy Study report number 1:
Photocoagulation for diabetic macular edema. Arch Ophthalmol 1985;103:1796-806.
4) Shahidi M, Ogura Y, Blair NP, et al. Retinal thickness analysis of quantitative assessment of diabetic macular edema.
Arch Ophthalmol 1991;109:1115-9.
5) Oshima Y, Emi K, Yamanishi S, Motokura M. Quantitative assessment of macular thickness in normal subjects and patients with diabetic retinopathy by scanning retinal thickness analyser. Br J Ophthalmol 1999;83:54-61.
6) Zambarakji HJ, Amoaku WM, Vernon SA. Volumetric analysis of early macular edema with the Heidelberg Retina Tomograph in diabetic retinopathy. Ophthalmology 1998;105:1051-9.
7) Hee MR, Izatt JA, Swanson EA, et al. Optical coherence tomography of the human retina. Arch Ophthalmol 1995;113:325-32.
8) Hee MR, Puliafito CA, Wong C, et al. Quantitative assessment of macular edema with optical coherence tomography. Arch Ophthalmol 1995;113:1019-29.
9) Konno S, Akiba J, Yoshida A. Retinal thickness measurements with optical coherence tomography and the scanning retinal thickness analyzer. Retina 2001;21:57-61.
10) Otani T, Kishi S, Maruyama Y. Patterns of diabetic macular edema with optical coherence tomography. Am J Ophthalmol 1999;127:688-93.
11) Kang SW, Park CY, Ham DI. The correlation between fluorescein angio and optical coherence tomographic features in clinically significant diabetic macular edema. Am J Ophthalmol 2004;137:313-22.
12) Kim DH, Kim SH, Kim HW, Yoon IH. Risk factors for diffuse diabetic macular edema as classified by optical coherence tomography. J Korean Ophthalmol Soc 2006;47:
548-55.
13) Jonas JB, Sofker A. Intraocular injection of crystalline cortisone as adjunctive treatment of diabetic macular edema.
Am J Ophthalmol 2001;132:425-7.
14) Martidis A, Duker JS, Greenberg PB, et al. Intravitreal triamcinolone for refractory diabetic macular edema. Ophthal mology 2002;109:920-7.
15) Ip MS. Intravitreal injection of triamcinolone: an emerging treatment for diabetic macular edema. Diabetes Care 2004;27:
1794-7.
16) Brasil OF, Smith SD, Galor A, et al. Predictive factors for short-term visual outcome after intravitreal triamcinolone acetonide injection for diabetic macular oedema: an optical coherence tomography study. Br J Ophthalmol 2007;91:761-5.
17) Kim YG, Yu SY, Kwak HW. The effect of intravitreal
triamcinolone acetonide injection according to the diabetic macular edema type. J Korean Ophthalmol Soc 2005;46:84-9.
18) Nussenblatt RB, Kaufman SC, Palestine AG, et al. Macular thickening and visual acuity. Measurement in patients with cystoid macular edema. Ophthalmology 1987;94:1134-9.
19) Kim BY, Smith SD, Kaiser PK. Optical coherence tomography patterns of diabetic macular edema. Am J Ophthalmol 2006;142:405-12.
20) Ferris FL III, Patz A. Macular edema. A complication of diabetic retinopathy. Surv Ophthalmol 1984;28:S452-61.
21) Antcliff RJ, Marshall J. The pathogenesis of edema in diabetic maculopathy. Semin Ophthalmol 1999;14:223-32.
22) Cunha-Vaz JG. Diabetic macular edema. Eur J Ophthalmol 1998;8:127-30.
23) Lobo C, Bernardes R, Faria de Abreu JR, Cunha-Vaz JG.
Novel imaging techniques for diabetic macular edema. Doc Ophthalmol 1999;97:341-7.
24) Yannoff M, Fine BS, Brucker AG, Eagle RC Jr. Pathology of human cystoid macular edema. Surv Ophthalmol 1984;28:
S505-11.
25) Fine BS, Brucker AJ. Macular dema. Macular edema and cystoid macular edema. Am J Ophthalmol 1981;92:466-81.
26) Kaiser Pk, Riemann CD, Sears JE, Lewis H. Macular traction detachment and diabetic macular edema associated with posterior hyaloidal traction. Am J Ophthalmol 2001;131:44-9.
27) Yamaguchi Y, Otani T, Kishi S. Resolution of diabetic cystoid macular edema associated with spontaneous vitreofoveal separation. Am J Ophthalmol 2003;135:116-8.
28) Iida T, Yannuzzi LA, Spaide RF, et al. Cystoid macular degeneration in chronic central serous chorioretinopathy. Retina 2003;23:1-7.
29) Sabates NR, Sabates FN, Sabates R, et al. Macular changes after retinal detachment surgery. Am J Ophthalmol 1989;108:
22-9.
30) Alkuraya H, Kangave D, Abu El-Asrar AM. The correlation between optical coherence tomographic features and severity of retinopathy, macular thickness and visual acuity in diabetic macular edema. Int Ophthalmol 2005;26:93-9.
31) Cho HY, Lee JH. The correlation between visual acuity and patterns of diabetic macular edema in OCT images. J Korean Ophthalmol Soc 2003;44:2028-34.
32) Jonas JB, Martus P, Degenring RF, et al. Predictive factors for visual acuity after intravitreal triamcinolone treatment for diabetic macular edema. Arch Ophthalmol 2005;123:1338-43.
33) Mason JO 3rd, Somaiya MD, Singh RJ. Intravitreal concentration and clearance of triamcinolone acetonide in non-vitrectomized hyman eyes. Retina 2004;24:900-4.
34) Kang SW, Sa HS, Cho HY, Kim JI. Macular grid photocoagulation after intravitreal triamcinolone aceonide for diffuse diabetic macular edema. Arch Ophthalmol 2006;124:
653-8.
35) Lewis H, Abrams GW, Blumenkranz MS, Campo RV.
Vitrectomy for diabetic macular traction and edema associated with posterior hyaloidal traction. Ophthalmology 1992;99:
753-9.
=ABSTRACT=
The Effect of Intravitreal Triamcinolone Injection According to the OCT Patterns of Diabetic Macular Edema
Sang Chul Yoon, M.D., Dae Young Lee, M.D., Dong Heun Nam, M.D., Ph.D.
Department of Ophthalmology, Gachon University of Medicine and Science, Incheon, Korea
Purpose: To determine the preoperative factors of different types of diabetic macular edema (DME) classified using Optical Coherence Tomography (OCT) and to evaluate the short-term therapeutic effects and pattern changes of intravitreal triamcinolone acetonide injection (IVTA).
Methods: Seventy-seven eyes of 60 patients, who had been previously diagnosed with DME through fundoscopy and fluorescein angiography, were enrolled, and each patient was classified as one of three DME types according to his/her OCT features: Type 1, diffuse retinal thickening; Type 2, cystoid macular edema;
and Type 3, serous macular detachment. We compared age, sex, the duration of diabetes mellitus (DM), and decreased visual acuity (VA). We analyzed VA, intraocular pressure (IOP), foveal thickness (FT), total macular volume (TMV), and pattern changes that occurred between pre-operation and 1 month post-operation.
Results: The duration of DM was short in Type 3 DME patients. There were no differences in age or the duration of decreased VA. Pre-operative VA was higher in Type 1 than in Type 2 or 3 patients. FT and TMV increased in thickness from Type 1 through Type 3. VA after IVTA improved in Types 2 and 3. FT and TMV after IVTA decreased in each type. However, the extent of the changes in Types 2 and 3 was greater than that in Type 1. Seventy-four percent of Type 2 and 83% of Type 3 changed to Type 1 after IVTA.
Conclusions: This study found that there were differences in the therapeutic effect of IVTA among patients with different DME patterns. According to our results, the effectiveness of IVTA can be predicted, which we believe will help to objectively determine DME treatment.
J Korean Ophthalmol Soc 2008;49(10):1611-1618
Key Words: Diabetic macular edema, Intravitreal triamcinolone injection, Optical coherence tomography
Address reprint requests to Dong Heun Nam, M.D. Ph.D.
Department of Ophthalmology, Gachon University of Medicine and Science, Gil Medical Center
#1198 Kuwol-dong, Namdong-gu, Incheon 405-760, Korea
Tel: 82-32-460-3364, Fax: 82-32-460-3358, E-mail: [email protected]