DOI : 10.3341/jkos.2008.49.3.384
비강내 누낭비강문합술시 시행한 양막충전술의 단기 임상 결과
최영재․황상준․이태수 고려대학교 의과대학 안과학교실
목적 : 비강내 누낭비강문합술시 양막으로 감싼 MerocelⓇ을 골공에 위치시킨 후 단기 임상결과를 알아보고자 하였다.
대상과 방법 : 2005년 10월부터 2006년 4월까지 비루관 폐쇄의 치료로 비강내 누낭비강문합술을 시행받은 환자 60명을 대상으로 전향적인 연구를 시행하였다. 30명의 환자들에게는 술 후 양막으로 감싼 MerocelⓇ을 골공에 10일 에서 14일간 위치시키고(1군), 나머지 30명의 환자들에게는 일반적인 MerocelⓇ만을 충전하였다(2군). 추적관찰기 간 동안 두 군간의 수술 창상치유과정 및 육아종의 발생, 골공의 유지 정도 등을 비교, 분석하였다.
결과 : 수술 6개월 후의 성공률은 1군에서 93.3%, 2군에서는 86.7%로 1군에서 다소 높았으나 통계학적으로 유의 하지는 않았다(p=0.67). 수술 후 평균 창상치유기간은 1군에서 4.8±1.5주(3~10주), group 2에서 7.3±1.5주 (5~12주)로 1군에서 더 짧았다(p<0.001). 수술 후 2개월까지 육아종이 발생한 환자는 1군과 2군에서 각각 4명 (13%)과 11명(33%)으로 1군에서 더 적었다(p=0.04). 그러나 수술 후 6개월에는 각각 11명(33%)과 14명 (46%)에서 육아종이 발생하여 두 군에서 차이가 없었다.
결론 : 비강내 누낭비강문합술시 양막으로 감싼 MerocelⓇ 충전술 후 단기 임상 결과상 창상의 염증이 줄어들고 창상
치유 속도가 빨라졌으며 초기 육아종 발생을 줄일 수 있었다.
<한안지 49(3):384-389, 2008>
<접수일 : 2007년 3월 16일, 심사통과일 : 2007년 8월 21일>
통신저자 : 이 태 수
서울시 구로구 구로동길 97 고려대학교 구로병원 안과 Tel: 02-2626-1276, Fax: 02-857-8580 E-mail: [email protected]
* 본 논문의 요지는 2006년 대한안과학회 제96회 추계학술대회 에서 구연으로 발표되었음.
양막은 태반을 둘러싸는 태아 쪽으로 향한 가장 안쪽 막으로 1910년 Davis1가 피부이식을 위해 양막을 사 용한 이래로 여러 분야에서 사용되고 있다. 안과 영역 에서는 1940년 de Rotth2가 결막의 검구 유착과 결 손의 치료에 처음 사용하였고 1995년 Kim and Tseng3이 각막 상피제거 및 각막윤부 층판절제술을 시 행한 토끼 모델에서 양막을 사용하여 성공적인 안구 표 면의 재형성을 보고하고 양막의 처치와 보관 방법을 발 전시킨 이후 최근까지 널리 사용되고 있다. 각막 화상,4 스티븐스-존슨 증후군(Stevens-Johnson syndrome),5 재발된 익상편6 등 다양한 안구 표면질환의 치료에 성
공적으로 이용되고 있으며 치유되지 않는 각막궤양 및 지속성 상피세포 결손,7-10 괴사성 공막염,11,12 각막 천 공13 등의 난치성 질병에도 사용되고 있다. 또한 녹내장 환자에서 섬유주절제술 후 여과포 유지에 도움이 된다 는 보고도 있고14 엑시머레이저를 이용한 수술 후 섬유 아세포 증식을 억제하고 각막 혼탁 발생을 줄이는 것으 로 보고되었다.15-17
한편 비강내 누낭비강 문합술 후 비강내 창상 치유기 간은 경피적 누낭비강문합술에 비해 긴 것으로 알려져 있고 수술 초기에 실패의 흔한 요인으로 창상치유기간 동안에 발생하는 육아종, 염증, 반흔 조직의 과다형성 등이 알려져 있다.18-20 이에 저자들은 비강내 누낭비강 문합술 후 양막으로 감싼 MerocelⓇ을 골공부위에 충 전함으로써 단기 임상 결과상 비강내 점막의 창상치유 속도가 빠르고 육아종이 적게 발생하는 등의 결과를 얻 었기에 이를 국내에서 처음으로 보고하는 바이다.
대상과 방법
2005년 10월부터 2006년 4월까지 비루관폐쇄증으 로 진단되어 고려대학교 구로병원 안과에서 비강내 누
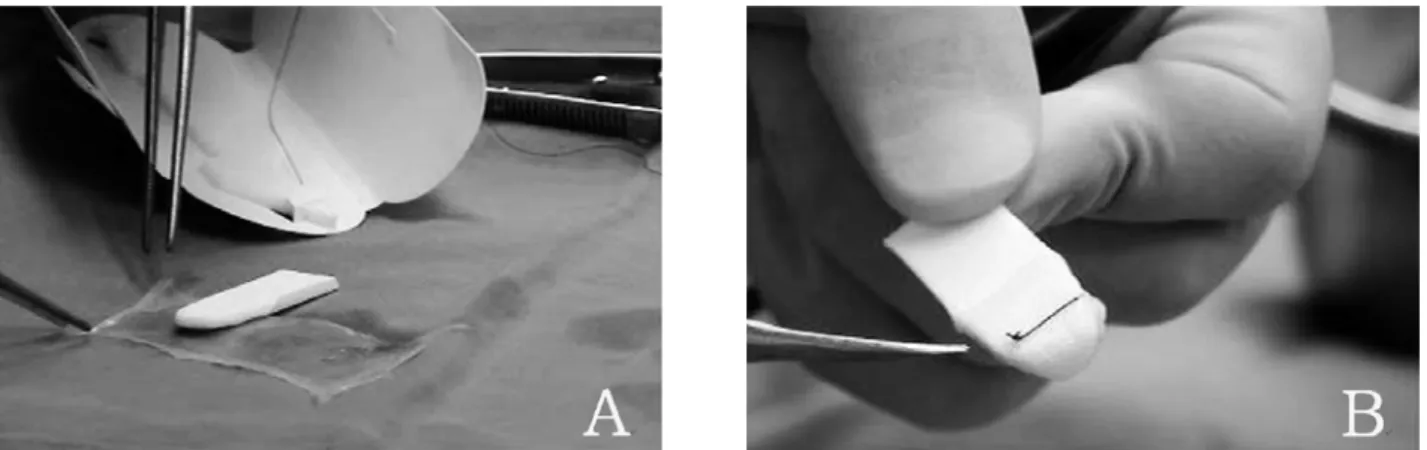
Figure 1. MerocelⓇ was wrapped with amniotic membrane (A) and fixed with 6-0 silk (B).
낭비강문합술을 시행받은 60명의 환자 60안을 대상으 로 이들 중 30안에 대해서는 수술 후 양막으로 감싼 MerocelⓇ을 비강내 골공에 충전하였고(1군), 나머지 30안에 대해서는 일반적인 MerocelⓇ을 충전하여(2 군) 그 결과를 전향적으로 비교 분석하였다.
양막의 채취는 B형, C형간염, HIV, 매독 등의 혈청 검사 상 음성인 산모의 정규 제왕절개시 시행하였고 수 술 전 산모 및 보호자에게 이에 대한 인지 동의서를 받 았다. 양막의 처리 및 보관은 Kim and Tseng3이 보 고한 방법에 따라 시행하였다. 제왕절개 직후 태반으로 부터 양막을 분리하고 phosphate buffered saline (penicillin 50 µg/mg, gentamicin 8 µg/mg, am- photericin B 2.5 µg/mg 함유)을 이용하여 씻고 이 후 양막의 상피쪽이 반대로 향하도록 Nitrocellulose paper 위에 얇게 펼친 후 Dulbecco’s modified Eagle Medium (Life Technologies Inc, N.Y., USA)과 100% glycerin을 1:1로 섞은 media에 넣 어 영하 70℃ 냉장고에 보관하였다.
모든 환자는 수술 전 내시경 검사를 시행하여 비강의 크기, 비강 내 다른 병변의 유무와 비중격만곡 등의 비 강 상태를 확인하였고 심한 비중격만곡이 있는 경우는 이비인후과에서 비중격 교정술을 수술 전에 시행받도록 하였으며 비강의 크기 및 비강의 상태에 따라 전신마취 또는 국소마취로 수술을 시행하였다.
수술 과정 중 점막의 제거는 단극성 소작기나 radio- surgical unit (Ellman ntl. Inc., NY, USA)을 사용하였고 드릴과 Kerrison 펀치를 사용하여 직경 5~8 mm의 골공을 만들었다. 그 후 Nd:YAG 레이저 (LaserscopeⓇ, San Jose, CA, USA) 소식자(La- ser optics, 0.6 mm in diameter)를 누소관을 통 하여 누낭에 집어넣고 내시경으로 비강을 통하여 누낭 의 내측벽을 관찰하면서 내측벽을 제거하였다(Con- tact mode, laser power: 15 watt, continuous
mode). 이후 두 개의 실리콘관(Guibor canalicular intubation setsⓇ, Xomed-Treace, Jackson- ville, FL, USA)을 삽입하여 금속 클립으로 결찰하 고 실리콘 여분이 5 mm 정도 되도록 절단하여 비강 내에 안착시켰다. 그 후 출혈을 방지하기 위하여 Merocel sponge를 비강내에 packing 하였다. 이 때 1군에서는 MerocelⓇ을 양막으로 감싸고 6-0 silk를 이용하여 고정시킨 후(Fig. 1) 비강내에 packing 하 였고 2군에서는 일반적인 MerocelⓇ을 packing 하 였다.
수술 후 점안 항생제와 0.1% fluorometholone 안 약을 첫 날부터 하루 4회 점안하고 생리식염수 비강 세 척기를 이용하여 한 달간 하루 3회 정도 비강세척을 하 도록 교육하였다. 경과관찰은 술 후 첫 한 달간은 매주 마다, 그 다음 한 달간은 2주마다, 그 이후로는 한 달마 다 시행하였다. 매 내원 시 마다 유루증의 유무를 확인 하고 내시경을 통해 창상의 치유과정, 비강내 누공의 상태와 합병증 유무를 관찰하였고 이를 디지털 사진으 로 기록하여 이를 토대로 결과를 분석하였다. 충전된 MerocelⓇ은 1군의 경우에는 술 후 10~14일째 되는 날 제거하였고 감염을 우려해 중간에 내원 시 항생제 세척을 시행하였다. 항생제 세척 시에는 먼저 흡입기를 이용하여 분비물을 깨끗하게 제거한 후 23 G 바늘을 이 용하여 이미 팽창되어 있는 MerocelⓇ 내로 항생제를 주사하였다. 2군에서는 수술 후 1주일 째에 MerocelⓇ 을 제거하였다. 두 군에서 양막으로 둘러 싼 MerocelⓇ packing 이외의 위와 같은 수술 과정 및 수술 후 처 지, 추적관찰 등은 모두 동일하게 시행하였다.
수술의 성공은 환자의 유루증상이 소실되고 내측 누 공이 개통되어 있고 형광색소검사상 +1 이하인 경우로 정의하였다. 또한 재상피화 시기는 내시경으로 관찰하 여 창상의 상피화가 완전히 이루어진 가장 빠른 내원일 로 하였다.
Table 1. Characteristics of patients
Group 1 Group 2 p-value
Number of eyes 30 30 -
Age (yrs) 52.0±17.5 53.9±13.8 0.65*
Sex (M/F) 7/23 6/24 0.75†
Right/Left 13/17 11/19 0.60†
F/U duration (months) 8.5±1.6 8.9±1.8 0.85*
* Student’s t-test; †Pearson’s chi-square test.
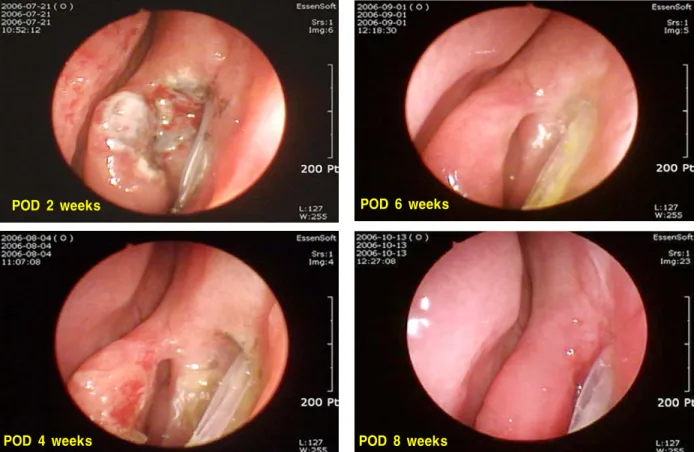
Figure 2. Serial photographs of postoperative wound healing process in group 1. Wound healing was nearly completed at 4 weeks after surgery.
결 과
환자들의 평균 나이는 1군에서 52.0±17.5세(29~
75세) 2군에서는 53.9±13.8세(33~84세)였으며 그 밖에 성별, 추적관찰기간 등은 두 군에서 차이가 없었 다(Table 1).
수술 6개월 후의 일차 성공률은 1군에서 93.3%
(28/30안), 2군에서 86.6% (26/30안)으로 1군 에서 다소 높았으나 통계적으로 유의하지는 않았다(p=
0.67). 수술 후 창상치유기간은 1군에서 평균 4.8±1.5 주(3~10주), 2군에서 7.3±1.5주(5~12주)로 1군에 서 더 짧았다(p<0.001). Figure 2는 1군 환자들 중
평균적인 창상치유과정을 보여주는 사진으로 수술 후 4 주 째 창상치유가 대부분 완료된 것을 볼 수 있다. 수술 후 합병증은 육아종 형성, 염증, 비강내 반흔 형성 등이 있었는데 이 중 육아종 형성이 가장 많았다(Table 2).
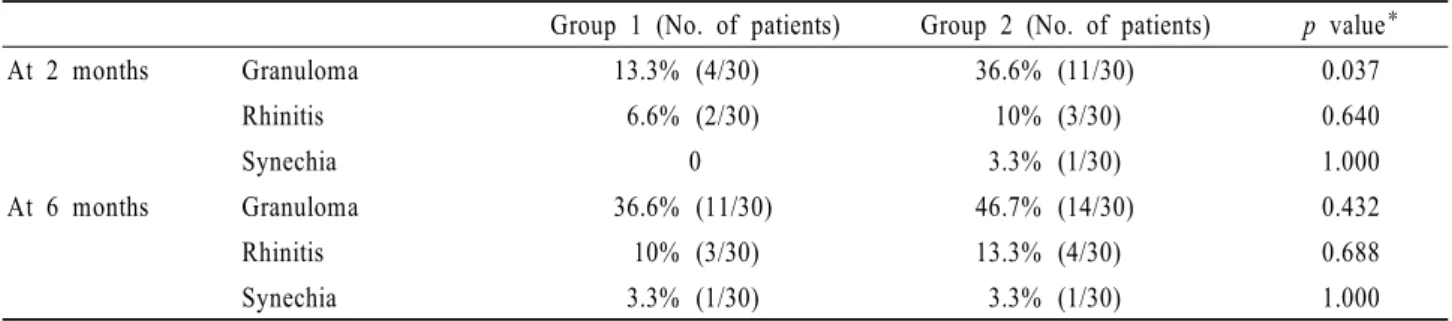
술 후 2개월 째에 육아종 발생은 1군에서 30안 중4안 (13.3%), 2군에서는 30안 중 11안(36.6%)로 1군에 서 유의하게 적었으나(p=0.037), 술 후 6개월 째에는 1군과 2군에서 각각 30안 중 11안(36.6%), 14안 (46.7%)에서 육아종이 발생하여 두 군에서 차이가 없 었다. 육아종의 발생 시기는 1군에서 평균 11.6±2.9 주(8~18주), 2군 에서는 평균 8.9 ± 2.4주(6~16주) 로 1군에서 육아종이 발생하는 시기가 더 늦었다.
POD 2 weeks POD 6 weeks
POD 4 weeks POD 8 weeks
Table 2. Postoperative complications
Group 1 (No. of patients) Group 2 (No. of patients) p value*
At 2 months Granuloma 13.3% (4/30) 36.6% (11/30) 0.037
Rhinitis 6.6% (2/30) 10% (3/30) 0.640
Synechia 0 3.3% (1/30) 1.000
At 6 months Granuloma 36.6% (11/30) 46.7% (14/30) 0.432
Rhinitis 10% (3/30) 13.3% (4/30) 0.688
Synechia 3.3% (1/30) 3.3% (1/30) 1.000
* Pearson’s chi-square test.
고 찰
비강내 누낭비강문합술의 실패 원인으로 비강측 누 공의 육아종, 반흔조직 등에 의한 폐쇄가 가장 흔한 것 으로 알려져 있고 특히 육아종 발생이 수술 실패의 가 장 흔한 원인으로 여러 연구를 통해 알려져 있다.18-20 또한 육아종은 창상치유과정에서 주로 생기기 때문에 창상치유기간이 길수록 육아종이 생길 가능성이 좀 더 높으며 실제로 Lee et al21은 재상피화가 늦게 되면 육 아종과 염증이 더 많이 발생하지만 창상이 깨끗하게 치 유된 경우에는 성공률이 높다고 보고한 바 있다. 따라 서 창상치유기간을 줄이고 좀 더 창상을 깨끗하게 유지 하는 것이 수술의 실패를 줄일 수 있을 것이다. 저자들 은 안구 표면 질환에서 양막이 상처치유에 도움이 된다 는 여러 연구를 바탕으로 누낭비강문합술 후에 양막을 골공에 충전한다면 비강내 점막의 창상 치유에 도움이 되어 창상치유기간을 줄이고 창상을 깨끗하게 유지할 수 있을 것이라는 가정하에 본 연구를 진행하였다.
본 연구에서 비강내 누낭 비강 문합술 후 창상치유 기간은 대조군의 경우 평균 7.3±1.5주로서 이는 저자 들이 이전에 보고한 860명의 성인의 평균 창상치유기 간인 7.1주와 유사하였다.22 반면 양막을 이용하여 MerocelⓇ packing을 시행한 군에서는 평균 4.8±1.5 주로 창상치유기간이 현저히 줄어든 것을 알 수 있었 다. 이는 다음과 같은 양막의 효과에서 기인하는 것으 로 생각된다. 첫째 양막이 상피세포의 이동을 용이케 하고23,24 기저상피세포(basal epithelial cell)의 유 착을 강화시키며,25 상피 분화를 증진시키는 역할을 하 여26,27 창상의 상피화를 증진시키는 것으로 알려져 있 다. 실제로 Meller et al23과 Meller and Tseng24 의 연구에서 윤부 상피세포나 결막 상피세포의 이동 및 분화를 양막이 촉진시키며 이를 임상에 적용하여 좋은 결과를 얻었다는 보고가 있다. 둘째 양막은 IL-1ra, IL-10 등의 항염증단백을 함유하고 있고28 IL-1, IL-8, PMN cell, elastase, neutrophile activation peptide-78 등의 케모카인(chemokine)을 down
regulation시켜 항염증작용을 나타내는 것으로 알려 져 있다.29,30 이러한 작용으로 창상의 염증이 줄어들고 따라서 창상 치유기간도 줄어들었으리라 생각된다. 또 한 양막은 항균 효과를 가져31,32 수술 후 창상의 감염 을 최소화 시킬 수 있으며 신생혈관형성을 억제하는 기 능이 있어28 창상치유에 도움이 되는 것으로 알려져 있다.
그 밖에도 TGF-β 신호전달체계(signaling system) 에 관여하여 섬유아세포의 활동과 근섬유세포로의 분화 를 억제시키므로 반흔 형성을 줄일 수 있다고 보고되고 있다.33,34
한편 육아종은 창상치유가 대부분 완료되는 수술 후 2개월까지는 양막을 이용한 MerocelⓇ 충전술을 시행 한 군에서 대조군보다 적게 발생하는 것으로 나타났으 나 수술 2개월 이후로는 많이 발생하여 수술 후 6개월 에는 두 군에서 유의한 차이가 없었다. 이는 비강내 점 막의 창상은 안구 표면질환들과 달리 비교적 치유기간 이 길어 초기에는 양막의 효과로 인해 육아종 발생이 어느 정도 줄어들었다가 후기에는 양막에서 나오는 인 자들의 효과가 없어지면서 일어나는 염증반응에 의한 것으로 생각된다. 특히 육아종 발생의 큰 원인들 중 하 나로 실리콘 튜브의 지속적인 기계적 자극이 주위 조직 에 만성적인 염증반응을 일으키기 때문인 것으로 알려 져 있다.35 본 연구에서 양막 충전술 군에서 수술 2개월 이후에 육아종 발생이 증가한 것은 이러한 실리콘 튜브 의 작용이 큰 것으로 사료된다.
한편 MerocelⓇ을 제거하는 시기가 1군에서 약 3일 에서 7일 정도 더 길었는데 이는 양막의 효과가 충분히 나타날 수 있도록 하기 위함이었으며 두 군간에 제거 시기가 차이나는 기간이 짧고 감염을 최대한 방지하기 위해 항생제 세척을 충분히 했으므로 MerocelⓇ을 제 거 시기를 다르게 한 것이 결과에 미치는 영향은 거의 없을 것이라고 생각된다.
결론적으로 수술 후 양막으로 감싼 Merocel pack- ing을 시행하는 것은 수술 초기의 염증반응을 최소화하 고 비강내 점막의 재상피화를 촉진시켜 창상 치유기간 을 단축시킬 수 있었고 수술 후 초기에 육아종의 발생
률을 줄일 수 있어 수술의 성공률이 다소 높았다. 그러 나 양막의 효과가 떨어지는 수술 후 2개월 이후로는 육 아종의 발생이 다시 증가하는 경향을 보여 앞으로 양막 충전술을 시행한 환자에 대해서는 조기에 실리콘 튜브 를 제거하는 것과 좀 더 많은 환자들을 대상으로 장기 추적관찰을 하는 연구가 필요할 것으로 생각된다.
참고문헌
1) Davis JW. Skin transplantation with a review of 550 cases at the Johns Hopkins Hospital. Johns Hopkins Med J 1910;15:
307.
2) De Rotth A. Plastic repair of conjunctival defects with fetal membrane. Arch Ophthalmol 1940;23:522-5.
3) Kim JC, Tseng SC. Transplantation of preserved human amniotic membrane for surface reconstruction in severely damaged rabbit corneas. Cornea 1995;14:473-84.
4) Meller D, Pires RT, Mack RJ, et al. Amniotic membrane transplantation for acute chemical or thermal burns. Ophthal- mology 2000;107:980-90.
5) Tsubota K, Satake Y, Ohyama M, et al. Surgical recon- struction of the ocular surface in advanced ocular cicatrical pemphigoid and Stevens-Johnson syndrome. Am J Ophthalmol 1996;122:38-52.
6) Shimazaki J, Shinozaki N, Tsubota K. Transplantation of amniotic membrane and limbal autograft for patients with recurrent pterygium associated symblephron. Br J Ophthalmol 1998;82:235-40
7) Letko E, Stechschulte SU, Kenyon KR, et al. Amniotic membrane inlay and overlay grafting for corneal epithelial defects and stromal ulcers. Arch Ophthalmol 2001;119:659-63.
8) Lee SH, Tseng SC. Amniotic membrane transplantation for persistent epithelial defects with ulceration. Am J Ophthalmol 1997;123:303-12.
9) Hanada K, Shimazaki J, Shimmura S, Tsubota K. Multilayered amniotic membrane transplantation for severe ulceration of the cornea and sclera. Am J Ophthalmol 2001;131:324-31.
10) Chen HJ, Pires RT, Tseng SC. Amniotic membrane trans- plantation for severe neurotrophic corneal ulcers. Br J Oph- thalmol 2000;84:826-33.
11) Alsagoff Z, Tan DT, Chee SP. Necrotising scleritis after bare sclera excision of pterygium. Br J Ophthalmol 2000;84;1050-2.
12) Han YK, Wee WR. Use of immunosuppressant in the treat- ment of surgically induced necrotizing scleritis (SINS) after pterygium excision. J Korean Ophthalmol Soc 2003;44:272-7.
13) Kim JH, Cheong TB, Kim JC. Amniotic membrane transplan- tation in perforation or impending perforation of cornea. J Korean Ophthalmol Soc 1999;40:1487-95.
14) Fujishima H, Shimazaki J, Shinozaki N, Tsubota K. Trabe- culectomy with the use of amniotic membrane for uncon- trollable glaucoma. Ophthalmic Surg Lasers 1998;29:428-31.
15) Woo HM, Kim MS, Kweon OK. The effect of amniotic membrane graft on the inhibition of corneal haze in rabbit. J Korean Ophthalmol Soc 1999;40:2385-94.
16) Wang MX, Gray TB, Park WC, et al. Reduction in corneal haze and apoptosis by amniotic membrane matrix in excimer laser photoablation in rabbits. J Cataract Refract Surg 2001;27:
310-9.
17) Yeom HY, Park SB, Lee HK, Kim EK. Effects of amniotic membrane after LASEK on epithelial healing, clinical and refractive outcomes. J Korean Ophthalmol Soc 2004;45:195-202.
18) Kong YT, Kim TI, Kong BW. A report of 131 cases of endoscopic laser lacrimal surgery. Ophthalmology 1994;101:
1793-800.
19) Lee HC, Chung WS. Success rate of endonasal dacryocystor- hinostomy. J Korean Ophthalmol Soc 1996:37:211-8.
20) Kim JH, Shin JC. Clinical evaluation of endoscopic transnasal dacryocystorhinostomy. J Korean Ophthalmol Soc 1997:38:
1706-11.
21) Lee TS, Kim SW, Park BW. The relationship between rate of wound healing and success rate after endonasal laser-drill assisted dacryocystorhinostomy. J Korean Ophthalmol Soc 1999:40:2969-74.
22) Shin HY, Lee TS, Beak SH. The comparision of surgical results of endonasal dacryocystorhinostomy in childen and adults. J Korean Ophthalmol Soc 2006:47;877-82.
23) Meller D, Pires RT, Tseng SC. Ex vivo preservation and expansion of human limbal epithelial stem cells on amniotic membrane cultures. Br J Ophthalmol 2002;86:463-71.
24) Meller D, Tseng SC. Conjunctival epithelial cell differentiation on amniotic membrane. Invest Ophthalmol Vis Sci 1999;40:
878-86.
25) Khodadoust AA, Silverstein AM, Kenyon DR, Dowling JE.
Adhesion of regenerating corneal epithelium. The role of base- ment membrane. Am J Ophthalmol 1968;65:339-48.
26) Guo M, Grinnell F. Basement membrane and human epider- mal differentiation in vitro. J Invest Dermatol 1989;93:372?8.
27) Kurpakus MA, Stock EL, Jones JC: The role of the basement membrane in differential expression of keratin proteins in epithelial cells. Dev Biol 1992;150:243-55.
28) Hao Y, Ma DH, Hwang DG. Identification of antiangiogenic and antiinflammatory proteins in human amniotic membrane.
Cornea 2000;19:348-52.
29) Bultmann S, You L, Spandau U, et al. Amniotic membrane down-regulate chemokine expression in human keratocyte.
Invest Ophthalmol Vis Sci 1999;40:S578.
30) Solomon A, Rosdnblatt M, Monroy D, et al. Suppression of interleukin 1α and interleukin 1β in human limbal epithelial cells cultured on the amniotic membrane stromal matrix. Br J Ophthalmol 2001;85:444?9.
31) Kjaergaard N, Helmig RB, Schonheyder HC. Chorioamniotic membranes constitute a competent barrier to group B strepto- coccus in vitro. Eur J Obstet Gynecol Reprod Biol 1999;83:
165-9.
=ABSTRACT=
Short-Term Clinical Results of Amniotic Membrane Application to Endonasal Dacryocystorhinostomy
Young Jae Choi, M.D., Sang Jun Hwang, M.D., Tae Soo Lee, M.D.
Department of Ophthalmology, Korea University College of Medicine, Seoul, Korea
Purpose: To evaluate the short-term surgical results of MerocelⓇ nasal packing wrapped with human amniotic membrane on the internal ostium during endonasal dacryocystorhinostomy (DCR).
Methods: Sixty patients who underwent endonasal DCR to treat nasolacrimal duct obstruction from October 2005 to April 2006 were enrolled in this prospective study. The patients were divided into two groups: 30 patients treated with MerocelⓇ packing wrapped with amniotic membrane were assigned to group 1, and the remaining 30 patients were assigned to group 2. During the follow-up period, the authors evaluated surgical wound healing, the incidence of granuloma, and the patency of the internal ostium.
Results: Success rates at 6 months after surgery were higher in group 1 than in group 2, but these rates showed no statistically significant difference between the two groups (group 1: 93.3%, group 2: 86.7%, p=0.67). The time for mean wound healing in group 1 was significantly shorter than that in group 2 (group 1: 4.8±1.5 weeks, group 2: 7.3±1.5 weeks, p<0.001). The incidence of granuloma in group 1 was lower than that in group 2 at 2 months after surgery (group 1: 13% (4/30), group 2:33% (14/30), p=0.04). However, there was no difference of granuloma formation between the two groups at 6 months postoperatively (group 1: 33% (11/30), group 2: 46% (14/30)).
Conclusions: The authors believe that the use of MerocelⓇ packing wrapped with amniotic membrane after endonasal DCR might decrease postoperative inflammation, accelerate wound healing, and decrease granuloma formation in the early postoperative period.
J Korean Ophthalmol Soc 49(3):384-389, 2008
Key Words: Amniotic membrane, Endonasal dacryocystorhinostomy, Merocel
Address reprint requests to Tae Soo Lee, M.D., Ph.D.
Department of Ophthalmology, Guro Hospital, Korea University College of Medicine
#97 Guro-donggil, Guro-gu, Seoul 152-703, Korea
Tel: 82-2-2626-1276, Fax: 82-2-857-8580, E-mail: [email protected] 32) Kjaergaard N, Hein M, Hyttel L. Antibacterial properties of
human amnion and chorion in vitro. Eur J Obstet Gynecol Reprod Biol 2001;94:224-9.
33) Li DQ, Lee SB, Tseng SC. Differential expression and regulation of TGF-beta1, TGF-beta2, TGF-beta3, TGF-beta RI, TGFbeta RII and TGF-beta RIII in cultured human corneal, limbal,and conjunctival fibroblasts. Curr Eye Res 1999;19:
154-61.
34) Tseng SCG, Li, D-Q, Ma, X. Downregulation of TGF- β1,β2, β3, and TGF-β receptor II expression in human corneal fibro- blasts by amniotic membrane. Invest Ophthalmol Vis Sci 1998;39:S428.
35) Dresner SC, Codere F, Brownstein S, Jouve P. Lacrimal drainage system inflammatory masses from retained silicone tubing. Am J ophthalmol 1984:98;609-13.