247
Copyrights © 2014 The Korean Society of Radiology
INTRODUCTION
Neurofibromatosis type 1 (NF-1) is a autosomal dominant in- herited condition. The diagnostic criteria for this disease include development of café au lait spots, plexiform neruofibroma, axil- lary or groin freckling, optic glioma, Lisch nodule formation, distinctive bony lesions, and a first-degree relative with NF-1.
Patients with NF-1 may have additional features such as intra- cranial tumors, macrocephaly, pheochromocytoma, neurologic impairment, vascular stenosis, or aneurysms. Vascular involve- ment of NF-1 is very rare and may present as an aneurysm, ob- struction, or stenosis. Vasculopathy associated with NF-1 may result in hemothorax, a condition that can result in fatal compli- cations or sudden death (1).
CASE REPORT
A 34-year-old man developed sudden onset left pleuritic pain and dyspnea 5 days before admission to the emergency room.
He had a palpable, nonpulsatile swelling on the left side of his neck. The patient also had multiple café au lait spots and polyp- osis all over his body. His mother had a history of multiple cuta- neous neurofibromas. The patient had sinus tachycardia and hy- pophonesis on the left hemithorax. His blood pressure was 110/70 mm Hg with a heart rate of 104 beats/min, respiratory rate of 24 breaths/min, and oxygen saturation of 97%. His he- matocrit value was 25% with a hemoglobin level of 8.8 g/dL.
A large degree of left pleural effusion and atelectasis of the left lung were observed on the chest radiograph, and the trachea had shifted to the right thorax (Fig. 1A). Thoracic computed to- mography (CT) revealed a massive left hemothorax and passive atelectasis. In addition, a pseudoaneurysm (maximum diameter 3.8 cm, 2.4 cm in neck size) was detected in the left proximal vertebral artery with a perianeurysmal hematoma. The left sub- clavian artery was compressed by the aneurysm with a hemato- ma (Fig. 1B). The patient was referred to the interventional unit for emergent embolization of the aneurysm. Selective vertebral angiography showed a pseudoaneurysm 3.8 cm in size originat-
Case Report
pISSN 1738-2637 / eISSN 2288-2928 J Korean Soc Radiol 2014;70(4):247-250 http://dx.doi.org/10.3348/jksr.2014.70.4.247
Received December 20, 2013; Accepted March 3, 2014 Corresponding author: Dong Hun Kim, MD Department of Radiology, Chosun University Hospital, 365 Pilmun-daero, Dong-gu, Gwangju 501-717, Korea.
Tel. 82-62-220-3543 Fax. 82-62-228-9061 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
We report a case of a massive hemothorax arising from a ruptured vertebral artery aneurysm in a patient with neurofibromatosis type 1 suffering from sudden onset of dyspnea. The vertebral artery aneurysm was treated with endovascular coil em- bolization. Then, an open thoracotomy was performed to evacuate the hematoma.
Index terms Aneurysm Vertebral Artery Hemothorax Neurofibromatosis Computed Tomography Coil Embolization
Interventional and Surgical Treatment of a Hemothorax Caused by a Ruptured Vertebral Artery in a Patient with Neurofibromatosis Type I
1 제1형 신경섬유종증 환자에서 척추동맥 파열에 의한 혈흉에 대한 중재적, 수술적 치료1Ji Hoon Lee, MD
1, Dong Hun Kim, MD
1, Dong Hyun Kim, MD
1, Hong Joo Seo, MD
2Departments of 1Radiology, 2Cardiovascular Surgery, Chosun University College of Medicine, Gwangju, Korea
Spontaneous Hemothorax by Ruptured Vertebral Artery in NF-1
248
J Korean Soc Radiol 2014;70(4):247-250 jksronline.orgbolization and stent deployment, patency of left subclavian ar- tery and occlusion of distal portion of left vertebral artery are confirmed by thoracic aortography (Fig. 1D). The patient was subsequently transferred to the operating room for an explor- atory thoracotomy and evacuation of the hematoma. A 4 L he- matoma was removed during the operation.
The patient was stable after surgery. However, he experienced numbness and pain in the left forearm. Thoracic CT was repeat- ed 13 days after embolization and surgery. An in-stent occlusion within the left subclavian artery was observed (Fig. 1E). A by- ing from the left proximal vertebral artery and 80% narrowing
of the left mid-subclavian artery (Fig. 1C). The patient under- went embolization of the efferent vertebral artery with microplex 7EA coils (5 mm/15 cm, Microvention Terumo Medical Prod- ucts, Somerset, NJ, USA) to occlude proximal and distal blood flow of the vertebral aneurysm. However, coil embolization of the afferent vertebral artery failed as the afferent segment was adjacent to the origin of the left subclavian artery. Additionally, an uncovered stent 1EA (10/60 mm, SNG, Seoul, Korea) was in- serted into the compressed left subclavian artery. After coil em-
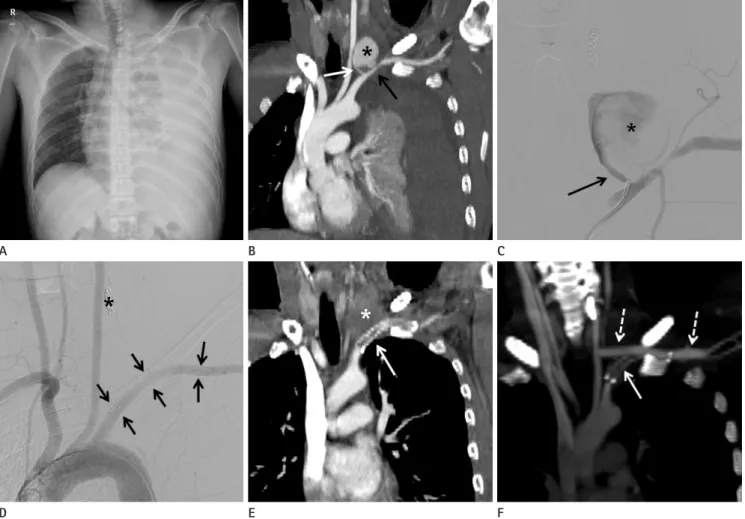
Fig. 1. A 34-year-old man with neurofibromatosis.
A. Chest radiography reveals a large degree of left pleural effusion with passive atelectasis. The trachea has also shifted to the right side.
B. Thoracic CT angiography reveals a pseudoaneurysm (asterisk) 3.8 cm in size in the left proximal vertebral artery (white arrow). The left subcla- vian artery (black arrow) is compressed by an aneurysm with a hematoma.
C. Vertebral angiography after embolization with a microcoil was performed to treat a pseudoaneurysm (asterisk) 3.8 cm in size originating from the left proximal vertebral artery (black arrow) and an 80% narrowing of the left mid-subclavian artery.
D. Thoracic aortography after coil embolization (asterisk) and stent deployment (arrows) shows patency of left subclavian artery and occlusion of distal portion of left vertebral artery.
E. On thoracic CT performed 13 days after embolization and surgery, an in-stent occlusion within the left subclavian artery (arrow) attached to a perivertebral hematoma (asterisk) is detected.
F. An oblique coronal CT scan with maximal intensity projection shows good patency within the left common carotid artery to the left subclavian artery bypass graft (dotted arrows) and an occluded stent in the left subclavian artery (arrow).
E B
D A
F C
Ji Hoon Lee, et al
249
jksronline.org J Korean Soc Radiol 2014;70(4):247-250
due to an intrathoracic aneurysm include surgical and non-sur- gical techniques. As this disease can be fatal, emergency opera- tions such as thoracotomy with excision of lesion have been per- formed. However, some recent reports demonstrated that non- surgical methods such as endovascular intervention or stent- graft placement are preferable for treating hemothorax arising from an aneurysm rupture in cases of NF-1 (3, 4, 9). In addition, a good prognosis of patients undergoing these procedures has been described (2, 10). Endovascular coil embolization is a use- ful, less invasive, and a safe method for controlling arterial hem- orrhage in cases that do not require preservation of arterial flow.
In our patient, we performed endovascular coil embolization and also inserted a stent into the adjacent stenotic lesion. NF-1 vasculopathy may cause further hemodynamic and neurologic complications. Accordingly, the effects of vasculopathy and re- sulting secondary consequences should be considered.
In conclusion, vasculopathy associated with NF-1 is rare condi- tion. However, ruptured aneurysms can cause a fatal hemothorax and secondary complications such as blood flow disturbances.
Imaging techniques to determine the extent of the lesion, detect complications, and plan treatment methods including endovascu- lar intervention or surgery should be carefully performed.
REFERENCES
1. Hirsch NP, Murphy A, Radcliffe JJ. Neurofibromatosis:
clinical presentations and anaesthetic implications. Br J Anaesth 2001;86:555-564
2. Niimi M, Ikeda Y, Kan S, Takami H, Furui S, Takeshita K. Re:
spontaneous rupture of an intercostal artery due to neu- rofibromatosis type I disease treated by percutaneous em- bolization. Cardiovasc Intervent Radiol 2002;25:160-161 3. Kim SJ, Kim CW, Kim S, Lee TH, Kim KI, Moon TY, et al. En-
dovascular treatment of a ruptured internal thoracic ar- tery pseudoaneurysm presenting as a massive hemothorax in a patient with type I neurofibromatosis. Cardiovasc In- tervent Radiol 2005;28:818-821
4. Hongsakul K, Rookkapan S, Tanutit P, Pakdeejit S, Song- jamrat A, Sungsiri J. Spontaneous massive hemothorax in a patient with neurofibromatosis type 1 with successful transarterial embolization. Korean J Radiol 2013;14:86-90 5. Hall RJ, Miller GA, Kerr IH. Ruptured bronchial artery an- pass graft from the left carotid artery to the left subclavian artery
was performed, and the hematoma around the left vertebral ar- tery was removed (Fig. 1F). Postoperative electromusculogra- phy for persistent pain and paresthesia in the left forearm indi- cated a left brachial plexus injury at the trunk level. The patient was transferred to the rehabilitation department and his condi- tion improved with medication, physical therapy, and occupa- tional therapy.
DISCUSSION
A spontaneous hemothorax due to an intrathoracic arterial rupture in cases of NF-1 is rare. The incidence of vasculopathy in patients with NF-1 is only 3.6% (2) including individuals with aneurysms and a stenosis. Aneurysms may rupture and result in a fatality. Rupture of aneurysms in the subclavian (3), intercostal (4), bronchial (5), and vertebral arteries (6) have been reported in patients with NF-1. Salyer and Salyer (7) suggested that inti- mal thickening accompanying NF-1 vasculopathy is the result of Schwann cell proliferation within the arteries. This demon- strates a pathogenic relationship between vasculopathy and neurofibromas that characterize NF-1. An aneurysm in a pa- tient with NF-1 is characterized by fibrous intimal thickening, irregular loss of smooth muscle media, and elastic membrane fragmentation. These features often cause weakening of the sup- portive connective tissue and adjacent muscle coat in the wall of the artery, which could cause rupture of the arterial wall (6). A more recent study showed that smooth muscle cells rather than Schwann cells proliferate in cases of NF-1 vasculopathy (7).
Diagnostic modalities for patients with NF-1 and vasculopa- thy include CT or magnetic resonance angiography, chest X-ray, chest ultrasound, and thoracentesis. Among these methods, CT angiography is the best method for assessing vascular lesions and the selection of treatment by endovascular intervention (8, 9). CT can show detailed anatomy, and is less invasive. We be- lieve that postoperative CT angiography was important for our case not only because it allowed us to evaluate complications and the prognosis, but it was also a non-invasive procedure and alleviated patient pain during the evaluation. We were also able to detected stent occlusion and obliteration of the pseudoaneu- rysm by follow-up CT angiography.
Therapeutic maneuvers for treating a massive hemothorax
Spontaneous Hemothorax by Ruptured Vertebral Artery in NF-1
250
J Korean Soc Radiol 2014;70(4):247-250 jksronline.orglopathy. Eur J Pediatr 1994;153:107-109
9. Chang WC, Hsu HH, Chang H, Chen CY. Spontaneous he- mothorax caused by a ruptured intercostal artery aneu- rysm in von Recklinghausen’s neurofibromatosis. J Formos Med Assoc 2005;104:286-289
10. Dominguez J, Sancho C, Escalante E, Morera JR, Moya JA, Bernat R. Percutaneous treatment of a ruptured intercostal aneurysm presenting as massive hemothorax in a patient with type I neurofibromatosis. J Thorac Cardiovasc Surg 2002;124:1230-1232
eurysm mimicking aortic dissection. Br Heart J 1977;39:
909-910
6. Miyazaki T, Ohta F, Daisu M, Hoshii Y. Extracranial vertebral artery aneurysm ruptured into the thoracic cavity with neurofibromatosis type 1: case report. Neurosurgery 2004;
54:1517-1520; discussion 1520-1521
7. Salyer WR, Salyer DC. The vascular lesions of neurofibro- matosis. Angiology 1974;25:510-519
8. Lehrnbecher T, Gassel AM, Rauh V, Kirchner T, Huppertz HI.
Neurofibromatosis presenting as a severe systemic vascu-
제1형 신경섬유종증 환자에서 척추동맥 파열에 의한 혈흉에 대한 중재적, 수술적 치료1
이지훈
1· 김동훈
1· 김동현
1· 서홍주
2저자들은 갑작스런 호흡곤란을 호소하는 제1형 신경섬유종증 환자에서 척추동맥 파열에 의한 대량 혈흉을 보이는 증례를 보고하고자 한다. 척추동맥의 가성동맥류는 코일 색전술로 치료하였다. 이후 혈흉은 개흉술을 통해 제거되었다.
조선대학교 의학전문대학원 1영상의학과학교실, 2흉부외과학교실