84
소장폐쇄환자에서 복강경 수술의 유용성
경희대학교 의학전문대학원 외과학교실 김상현ㆍ김범수ㆍ김용호ㆍ최성일
The Feasibility of Laparoscopic Surgery in the Management of Small Bowel Obstruction
Sang Hyun Kim, M.D., Bum Soo Kim, M.D., Yong Ho Kim, M.D., Sung Il Choi, M.D.
Department of Surgery, Kyung Hee University School of Medicine, Seoul, Korea
Purpose: Laparoscopy is being used increasingly for the management of small bowel obstructions (SBOs), but only a few studies have examined the indications and utility of laparoscopic surgery in SBO. This study investigated the feasibility, effectiveness and safety of laparoscopic surgery in SBO, as well as the predictors of the success or failure of laparoscopic surgery.
Methods: From June 2006 to March 2010, 73 patients underwent surgery for SBO at the Department of Surgery, Kyung Hee University Medical Center. The patients treated by laparoscopy were compared with those treated by laparo- tomy in terms of the differences in operative time, postopera- tive hospital stay and return of bowel function, as evidenced by the toleration of a liquid diet, surgical site infection and recurrence rate. A Chi-square test, student’s t-test and ANOVA test were performed to identify the predictors of success or failure of laparoscopic surgery, particularly the preoperative laboratory findings, vital signs, previous abdominal surgery, duration of illness, bowel diameter on abdomen plain film and location of the transition zone on computerized tomography.
Results: Of the 73 cases, 30 cases were in the laparoscopic group (41.1%) and 43 cases were in the laparotomy group (58.9%). The postoperative hospital stay was significantly shorter in the laparoscopic group than in the laparotomy group (8.1±5.8 vs. 15.2±14.9 days, p=0.04), and the period until the return of bowel function was significantly shorter in the laparoscopic group than laparotomy group (4.3±3.1 vs.
6.6±3.6 days, p=0.02). The surgical site infection rate tended to be lower in the laparoscopic group than in the laparotomy group (4.5% vs. 23.3%, p=0.07) and the mean surgery time
tended to be shorter in the laparoscopic group than in the laparotomy group (76.3±28.1 vs. 96.3±55.9 minutes, p=
0.06). There were no differences in the incidence of intra- operative bowel injury between the two groups (0/22 (0%) in the laparoscopic group vs. 2/43 (4.7%) in the laparotomy group, p=0.30), recurrence rate (0/22 (0%) vs. 3/43 (7.1%), p=0.34) and mortality rate (1/22 (4.5%) vs 0/43 (0%), p=0.30 respectively). The rate of conversion to open surgery was 26.7% (8/30). The causes of conversion to open surgery were severe bowel distension (2 cases), severe adhesion (2 cases), no visible cause of obstruction (1 case), iatrogenic bowel injury (1 case), bowel ischemia and perforation (1 case) and hemodynamic instability (1 case). There were no significant differences in the preoperative WBC count, CRP, pulse rate, number of past abdominal surgeries, duration of illness, bowel diameter on plain abdominal film and obstruction site between the successful group and conversion group, except for the significant differences in body temperature and marginal differences in the type of previous surgery.
Conclusion: The laparoscopic approach has been shown to be safe and feasible in the management of SBO for selected patients. There were no pre-operative predictive factors for successful laparoscopy, except for factors such as afebrility and previous gynecological surgery. Nevertheless, larger, randomized prospective trials will be needed to determine the predictors of success or failure of laparoscopic surgery.
Key words: Small bowel obstruction, Laparoscopy, Laparotomy
중심단어: 소장폐쇄, 복강경 수술, 개복 수술
※ 통신저자:최성일, 서울시 강동구 상일동 149 우편번호:134-727
경희대학교 의학전문대학원 외과학교실 Tel:02-440-6136, Fax:02-440-6295 E-mail:[email protected]
INTRODUCTION
Patients with a bowel obstruction represent some of the most difficult and vexing problems that surgeons face with regard
to the correct diagnosis, the optimal timing of therapy, and the appropriate treatment. Etiologies are either intraluminal (ingested foreign bodies, bezoars), extrinsic (postoperative adhesions, incarcerated hernias) or arising from the bowel wall itself (tumor, IBD). Adhesions, particularly after pelvic opera- tions (60%) are the leading cause of bowel obstruction in developed countries. The management of intestinal obstruction is initially conservative, provided that the patient is clinically stable and without signs of systemic toxicity. Traditionally, laparotomy and adhesiolysis have been the treatment of choice
for patients who have failed conservative measures or when clinical and physiologic derangements suggested toxemia and/or ischemia. Small bowel obstruction was initially viewed as a relative contraindication for laparoscopy due to the risk of iatrogenic bowel perforation and decreased visualization due to the distended bowel. At present, laparoscopic surgery is thought to promote faster recovery of bowel function, earlier return to activity, shorter hospital stay and reduced wound-related complications. Furthermore, laparoscopic surgery is associated with fewer postoperative adhesions than open surgery, thus potentially decreasing the recurrence rate of SBO.1 Hence despite its risks, laparoscopy seems to be an effective procedure for managing SBO, and is used increasingly for the manage- ment of SBO. But there are only a few studies on the indications and utility of laparoscopic surgery in SBO. This study not only investigates the feasibility, effectiveness and safety of laparoscopic surgery in SBO, but also the predictors of success or failure of laparoscopic surgery.
MATERIALS AND METHODS
From June 2006 to March 2010, seventy-three patients were submitted to surgery for SBO at the Department of Surgery, Kyung Hee University Medical Center. The diagnosis of SBO was mostly made on the basis of the patient’s history, the clinical examination, blood test and radiologic findings (plain abdominal film and/or contrast-enhanced abdominal CT scan).
Surgical treatment was performed when radiologic signs of bowel ischemia, perforation, peritoneal fluid or massive bowel loop distension as well as failure of medical treatment were observed. Medical treatment was considered as failure that continuous and aggravated pain, increased WBC count and body temperature, aggravation of bowel dilatation on radiologic finding and so on were found nevertheless adequate administration of fluid, electrolyte and prophylactic antibiotics with naso-gastric tube insertion. The decision to operate or not and to use a laparoscopic approach was made by the surgeon on call based on his experience and preference with laparoscopy and the history and current status of the patient.
All patients except anesthesiological contraindications to laparoscopy, severe abdominal distension and sepsis were considered for laparoscopy. Informed consent for laparoscopy with possible conversion was obtained.
For laparoscopy, Hasson’s technique for first port insertion, gentle manipulation with atraumatic graspers and adhesiolysis using scissors, and if needed, cautious electrocoagulation were used to avoid bowel injury. We tried to inspect the small bowel
in a retrograde fashion commencing at the cecum and decompressed bowel until the point of transition is identified whenever possible. If we couldn’t find the IC valve, We used to find the transitional zone directly. Care was taken to manipulate the bowel gently and to avoid holding the bowel itself, but rather to grasp the mesentery. If a band was found that clearly was responsible for the obstruction, it was cut with scissors, sometimes after monopolar coagulation. The small bowel was examined on its entire length until the operating surgeon was convinced that the obstruction was relieved. When difficulties arise in localizing transitional point, presence of dense adhesions or necessity for bowel resection, conversion is performed either to midline laparotomy or minilaparotomy.
Naso-gastric tube insertion and suction was done preoperatively for decompression of distended bowel and prevention of aspiration of gastric contents. Intraoperative bowel decom- pressive procedure was not performed routinely, but if we needed resection and anastomosis of small bowel, we did bowel decompression in extracorporeal method. In the postoperative period, the naso-gastric tube was removed as soon as possible, Liquid diet was resumed after passage of flatus and if tolerable LD, soft diet.
Data obtained included patient demographics (age, sex), previous surgical history, clinical and radiologic presentation (vital signs, duration of illness, laboratory findings, abdominal X-ray and CT scan), intraoperative outcomes (findings, opera- tive time and complications) and postoperative course (time to return of bowel function as evidenced by toleration of a liquid diet, length of hospital stay, surgical site infection and recurrence rate).
Comparisons between quantitative variables were made with student’s t-test and ANOVA test. Comparisons of proportions were made with a Chi-square test; statistical significance was set at p<0.05.
RESULTS
A total of 73 patients underwent surgical therapy for SBO.
Of the 73 cases, 30 cases were in the laparoscopic group (41.1%) and 43 cases were in the laparotomy group (58.9%).
There were 8 open conversion cases (8/30, 26.7%).
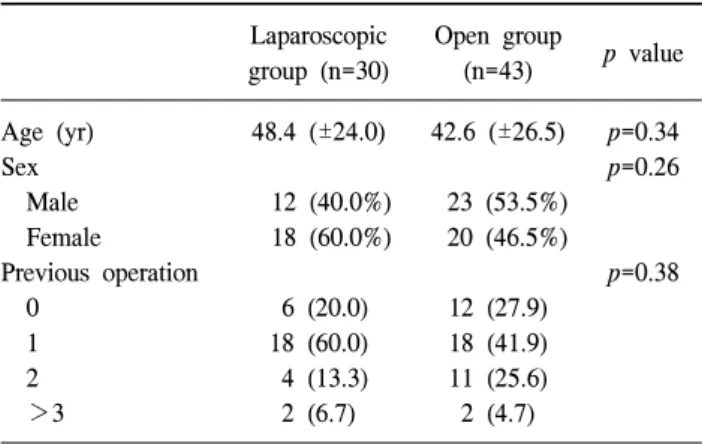
There were no significant differences between age, sex and the number of previous operations in each group (Table 1). The number of previous gynecologic procedures was significantly higher (p=0.01) in the laparoscopic group, while the number of previous colic resection was higher in the laparotomy group (p=0.007) (Table 2). Adhesion was the most common cause of
Table 1. Patient demographic data Laparoscopic group (n=30)
Open group
(n=43) p value Age (yr)
Sex Male Female Previous operation 0
1 2 >3
48.4 (±24.0) 12 (40.0%) 18 (60.0%) 6 (20.0) 18 (60.0) 4 (13.3) 2 (6.7)
42.6 (±26.5) 23 (53.5%) 20 (46.5%) 12 (27.9) 18 (41.9) 11 (25.6) 2 (4.7)
p=0.34 p=0.26
p=0.38
Units for age are = mean (range); Others are = number of patients (% of total n).
Table 2. Previous operations Laparoscopic group (n=30)
Open group
(n=43) p value Appendectomy
Cholecystectomy Gynecologic procedure Colectomy
Small bowel resection Gastrectomy
Hernia repair
Exploratory laparotomy Hepatobiliary-Pancreas- Spleen
5 (16.7) 0 12 (40.0)
1 (3.3) 0 3 (10.0)
0 4 (13.3)
0
7 (16.3) 1 (2.3) 6 (14.0) 12 (27.9) 3 (7.0) 5 (11.6)
2 (4.7) 3 (7.0) 3 (7.0)
p=0.96 p=0.40 p=0.01 p=0.007
p=0.14 p=0.83 p=0.23 p=0.36 p=0.14 Units are = number of patients (% of total n).
Table 3. Causes of bowel obstruction
Laparoscopic group (n=30)
Open group
(n=43) p value Total
Adhesion Neoplasm Hernia
Inflammatory disease (crohn, tuberculosis, parasite) Miscellanous (intussusception, radiation, volvulus) Intraluminal obstruction (bezoar, stone)
Congenital (malrotation, duplication cyst)
15 (50.0) 0 (0) 7 (23.3)
1 (3.3) 5 (16.7)
1 (3.3) 1 (3.3)
25 (58.1) 3 (7.0) 2 (4.7) 0 (0) 11 (25.6)
0 (0) 2 (4.7)
p=0.49 p=0.14 p=0.02 p=0.23 p=0.37 p=0.23 p=0.78
40 (54.8) 3 (4.1) 9 (12.3)
1 (1.4) 16 (21.9)
1 (1.4) 3 (4.1) Units are = number of patients (% of total n).
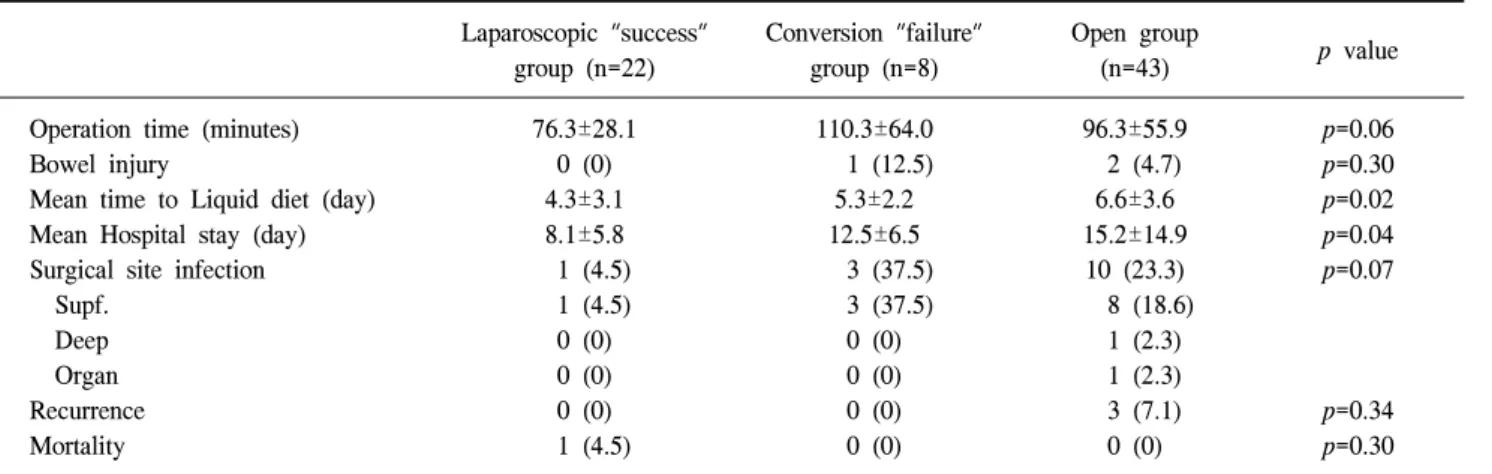
bowel obstruction in all groups. The number of patients with hernia was meaningfully greater in the laparoscopic group (p=0.02). All cases were of internal herniation, and no other type of hernia was seen in these cases (eg. inguinal hernia, ventral hernia) (Table 3). Postoperative hospital stay was significantly shorter in the laparoscopic “success” group than in the laparotomy group (p=0.04) and the period of return to bowel function was significantly shorter in the laparoscopic
“success” group than in the laparotomy group (p=0.02) (Table 4). The incidence of surgical site infection tended to be lower in the laparoscopic “success” group than in the laparotomy group (p=0.07) and the mean operative time tended to be shorter in the laparoscopic “success” group than in the laparotomy group (p=0.06) (Table 4). There were no differences between the two groups in the incidence of intraoperative bowel injury (p=0.30), recurrence rate (p=0.34) and mortality rate (p=0.30) (Table 4). The relatively simple procedure such as adhesiolysis or bandlysis in laparoscopic “success” group were performed meaningfully more than in conversion group or open
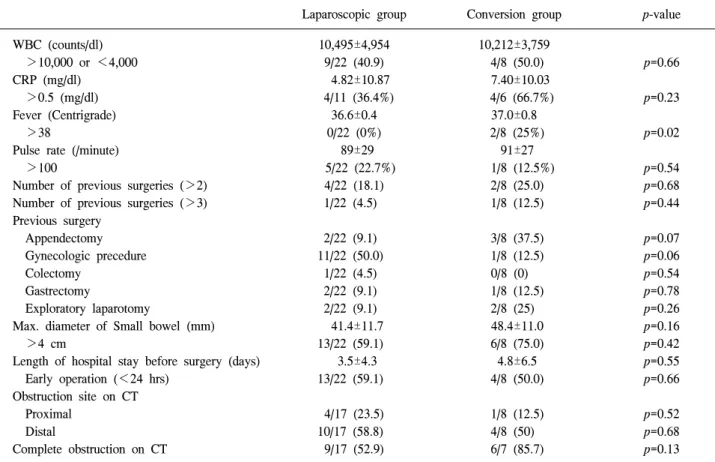
group. But the number of resection or bypass in laparoscopic success group did not differ from in conversion group or open group (Table 5). The rate of conversion to open surgery was 26.7% (8/30). The causes for conversion to open surgery were severe bowel distension (in 2 cases), severe adhesions (in 2 cases), no visible cause of obstruction (in 1 case), iatrogenic bowel injury (in 1 case), bowel ischemia and perforation (in 1 case), hemodynamic instability (in 1 case) (Table 6). There were no significant differences in preoperative WBC count, CRP, pulse rate, number of past abdominal surgeries, duration of illness (length of hospitalization before surgery), bowel diameter on plain abdominal film and obstruction site on CT scan between the successful group and the conversion group.
But, the number of cases of high fever (>38oC) were significantly greater in the conversion group than in the laparoscopic group (p=0.02) and the number of cases with a previous appendectomy were higher in the conversion group than in the laparoscopic group (p=0.07). In contrast, the number of patients with a previous gynecological surgery tended to be
Table 4. Intraoperative & postoperative outcomes
Laparoscopic "success"
group (n=22)
Conversion "failure"
group (n=8)
Open group
(n=43) p value
Operation time (minutes) Bowel injury
Mean time to Liquid diet (day) Mean Hospital stay (day) Surgical site infection Supf.
Deep Organ Recurrence Mortality
76.3±28.1 0 (0) 4.3±3.1 8.1±5.8 1 (4.5) 1 (4.5) 0 (0) 0 (0) 0 (0) 1 (4.5)
110.3±64.0 1 (12.5) 5.3±2.2 12.5±6.5 3 (37.5) 3 (37.5)
0 (0) 0 (0) 0 (0) 0 (0)
96.3±55.9 2 (4.7) 6.6±3.6 15.2±14.9 10 (23.3) 8 (18.6)
1 (2.3) 1 (2.3) 3 (7.1) 0 (0)
p=0.06 p=0.30 p=0.02 p=0.04 p=0.07
p=0.34 p=0.30 Figures are number of patients (% of total n), except those mentioned.
Table 5. Type of surgery for SBO
Laparoscopic "success"
group (n=22)
Conversion "failure"
group (n=8)
Open group
(n=43) p value
Adhesiolysis or bandlysis Primary closure of perforation Small bowel resection Bypass
14 (63.6) 0 (0) 7 (31.8)
1 (4.5)
1 (12.5) 2 (25.0) 4 (50.0) 1 (12.5)
17 (39.5) 0 (0) 21 (48.8) 5 (11.6)
p=0.03 p=0.01 p=0.40 p=0.63 Figures are number of patients (% of total n).
Table 6. Reasons for conversion
n (%) No visible cause of obstruction
Bowel necrosis/perforation Tumor
Iatrogenic perforation Dense adhesions
Technical difficulties d/t severe bowel distension Hemodynamic instability
Total
1 (12.5) 1 (12.5)
0 (0) 1 (12.5)
2 (25) 2 (25) 1 (12.5)
8 Units are = number of patients (% of total n).
higher in the laparoscopic group than in the conversion group (p=0.06) (Table 7).
DISCUSSION
Laparotomy has traditionally been the treatment of choice for patients requiring surgery for intestinal obstruction, although laparotomy itself is an independent risk factor for adhesive SBO.
After laparotomy, recurrence of obstruction is relatively frequent, leading to relaparotomy in up to 15% of the patients.2 Laparoscopy is thought to induce fewer subsequent posto- perative adhesions than laparotomy,3,4 and therefore it appears to be an attractive alternative to laparotomy for the management of acute SBO. In 1991, Bastug et al.5 reported the first laparoscopic lysis of a single adhesive band causing SBO.
However, despite this early report, the acceptance of laparoscopy in the management of SBO has been slow and this is clearly highlighted by the limited number of published studies in the last 15 years. The most likely reason is the paucity of clinical reports, the overall absence of selection criteria, and, perhaps, lack of experience in performing advanced laparoscopy in an emergency setting. In experienced hands, however, laparoscopy is a viable alternative to formal laparotomy. In the only two retrospective comparative studies in the literature, laparoscopic management of SBO appeared to offer the advantages of decreased overall morbidity, earlier return of bowel function, decreased length of hospital stay and faster return to full activity.6,7 Our results lent support to these reports demonstrating that the laparoscopic management of SBO is safe and effective in selected patients.
Table 7. Predictive factors for conversion
Laparoscopic group Conversion group p-value
WBC (counts/dl) >10,000 or <4,000 CRP (mg/dl)
>0.5 (mg/dl) Fever (Centrigrade) >38
Pulse rate (/minute) >100
Number of previous surgeries (>2) Number of previous surgeries (>3) Previous surgery
Appendectomy Gynecologic precedure Colectomy
Gastrectomy
Exploratory laparotomy
Max. diameter of Small bowel (mm) >4 cm
Length of hospital stay before surgery (days) Early operation (<24 hrs)
Obstruction site on CT Proximal
Distal
Complete obstruction on CT
10,495±4,954 9/22 (40.9) 4.82±10.87 4/11 (36.4%)
36.6±0.4 0/22 (0%)
89±29 5/22 (22.7%)
4/22 (18.1) 1/22 (4.5) 2/22 (9.1) 11/22 (50.0)
1/22 (4.5) 2/22 (9.1) 2/22 (9.1) 41.4±11.7 13/22 (59.1) 3.5±4.3 13/22 (59.1)
4/17 (23.5) 10/17 (58.8) 9/17 (52.9)
10,212±3,759 4/8 (50.0) 7.40±10.03 4/6 (66.7%)
37.0±0.8 2/8 (25%)
91±27 1/8 (12.5%)
2/8 (25.0) 1/8 (12.5) 3/8 (37.5) 1/8 (12.5)
0/8 (0) 1/8 (12.5)
2/8 (25) 48.4±11.0 6/8 (75.0) 4.8±6.5 4/8 (50.0) 1/8 (12.5) 4/8 (50) 6/7 (85.7)
p=0.66 p=0.23 p=0.02
p=0.54 p=0.68 p=0.44
p=0.07 p=0.06 p=0.54 p=0.78 p=0.26 p=0.16 p=0.42 p=0.55 p=0.66
p=0.52 p=0.68 p=0.13 WBC = white blood cell; CRP = c-reactive protein.
Adhesive SBO was the most common diagnosis in our series (54.7%) as has been widely reported by others.8-10 Internal hernia, volvulus, intussusception, malignancy, parasitic infec- tion (anisakiasis), bezoars and malrotation of small bowel were the other causes of SBO in our patients. The three leading causes of intestinal obstruction (adhesions, hernia, and malig- nancy) accounted for about 71.2% of cases in our data, which has been established in nearly 90% of cases of SBO in other literature,11 since there were 16 cases (21.9%) of SBO due to miscellaneous causes, and especially, there were 9 cases (12.3%) of ileocolic intussusception in infants. Conversely, the remaining etiologies may be quite diverse, and one must, therefore, be ready to deal with any possibility. When pathology other than adhesions is found on laparoscopy, the surgeon must be prepared to resect the intestine laparosco- pically or perform a small laparotomy incision to remove the cause of the obstruction.
The recurrent nature of adhesive small bowel obstruction (ASBO) represents a major clinical problem. There are clinical data12,13 backed up by several animal studies14 supporting the hypothesis that laparoscopy leads to a decreased rate of
adhesion formation as compared to laparotomy. This should be the main rationale to offer laparoscopy to prospective patients, rather than immediately recognizable benefits. It is not clear, however, if laparoscopic adhesiolysis for SBO would lead to a decrease in recurrence rate. In contrast to open management, which traditionally involves extensive adhesiolysis, no attempt is generally made during laparoscopic management to take down the entire abdominal wall and interloop adhesions.
Instead, only the adhesions impeding exposure and those causing the obstruction are treated. This more limited adhesiolysis may be responsible for the cases of non resolution or early recurrence of the SBO, requiring reoperation. Ghosheh and Salameh15 reported an early recurrence of SBO in 22 (2.1%) of 1,061 patients. No conclusion, however, can be made regarding the true long-term recurrence rate, since adequate follow-up is lacking in most published series. In the largest published multicenter study of 308 patients, the mean follow-up period was only 1.6 months.16 Similar to these reports, the mean follow-up period was only 5.1 months in our study data and most patients visited the outpatient department only once after surgery for SBO. Therefore, we thought that the result of
the recurrence rate between the laparoscopic group and the laparotomy group was meaningless.
In this study, laparoscopy established the cause of obstruction in 41% of patients, and treatment was completed endosco- pically in 73% of cases. Although results from the published, mostly retrospective, individual series vary significantly, the pooled data shows that laparoscopic management of SBO is successful in 66% of cases.15 Reasons for conversion are inability to identify the origin of the obstruction usually in relation to a reduced working space because of intestinal distension, inability to relieve obstruction completely because of adhesions that are too extensive, accidental bowel perforation, bowel necrosis, or need of short operative time because of hemodynamic instability. The decision to operate on a patient with SBO laparoscopically or openly is most often made by the attending surgeon empirically on the basis of his or her experience with laparoscopy and factors related to the patient. Preoperative knowledge of factors that prevent successful laparoscopy in this setting could help in the decision.
In this study, we tried to identify such factors by comparing the patients successfully treated with laparoscopy and those who needed conversion to open surgery.
The influence of the number and the type of previous abdominal procedures on the success of laparoscopic adhesiolysis is controversial. Some authors use this number as a criteria for deciding the choice of approach.16-18 Levard et al.14 represented that the factors significantly facilitated the success of laparoscopic treatments were less than three previous abdominal operations and antecedent appendectomy alone.
Others found that there is no correlation between previous surgery and risk of conversion to open surgery.1,19 Suter et al.1 reported that neither the number nor type of previous operations influenced the need for conversion. However, Mathieu et al.20 stated that the number of previous surgeries for colic resection was significantly higher in the laparotomy group, while the number of previous gynecologic procedures was significantly greater in the laparoscopic group, so the type of surgery previously performed is correlated with the need for conversion.
Navez et al.21 found that patients who had only a previous appendectomy were most likely to be successfully managed with laparoscopy. In our study, a previous appendectomy was predisposed to influence conversion, but the laparoscopic approach tended to be successful for patients with a previous gynecological surgery. Although we could not examine the relationship of the location of previous surgical wound and the laparoscopic surgery because of lack of data, It might be thought that the patients with previous gynecological surgery
had relatively light symptoms, short previous incision scar and loose adhesions in intraoperative field.
The rate of laparoscopic success was reported to be signi- ficantly higher in patients operated on early (<24 hours) and in patients with bands (54%), than in those with adhesions (31%) or with other causes of obstruction (15%).14 But, our study showed that there were no correlations in the length of hospital stay before operation however, it had similarities with the prior study that adhesiolysis or bandlysis in laparoscopic
“success” group were performed meaningfully more than in conversion group or open group. It is great likelihood of selection bias in the choice of patients because patients with little severity of SBO was tended to be treat laparoscopically.
As a result, intra- and postoperative outcomes might be affected by this bias.
7 patients (31.8%) in laparoscopic success group have small bowel resection for bowel ischemia or perforation. Procedure for bowel resection and anastomosis was performed by means of extracorporeal approach, gentle and delicate manipulation was required for the prevention of soiling. There were no significant differences between the portions of small bowel resection in each group, therefore, bowel ischemia or perforation is not the absolute indication of conversion or open surgery.
A significant correlation was found between conversion and presence of peritonitis by both Benoist et al.17 and Suter et al.1 The only preoperative predictor of bowel necrosis was a WBC count exceeding 11×109 per liter, as was shown by Benoist et al.,17 However, Suter et al.1 did not consider an elevated WBC count as a contraindication to laparoscopy. We could not find a correlation between the elevation of WBC count, CRP and pulse rate regarded as the signs of peritonitis and the increased rate of conversion. High fever was identified as the only predictive factor that could increase the failure rate of laparoscopic approach.
Radiology can play a central part in making the correct diagnosis of small bowel obstruction. It is important to consider the bowel diameter, degree of abdominal distention, and location of the obstruction (ie, proximal or distal).22 Bowel diameter can be determined on abdominal plain x-ray films.
Suter et al.1 found that a bowel diameter exceeding 4 cm was associated with an increased rate of conversion: 55% versus 32% (p=0.02). Bowel diameter was not predicting factor on deciding successful laparoscopy in our report. A computed tomography scan of the abdomen and pelvis can provide additional information about the location of the transition point and delineate a complete from a partial obstruction. Patients
with a distal and complete small bowel obstruction have an increased incidence of intra-operative complications and increased risk of conversion.22 However, in this data, there were no significant differences in presence of complete obstruction and obstruction site between the successful group and the conversion group.
CONCLUSION
A laparoscopic approach has been shown to be safe and feasible in the management of SBO for selected patients. In experienced hands, it appears to be a viable and attractive alternative to laparotomy. There were no preoperative predictive factors for successful laparoscopy, except for factors such as afebrility and a previous gynecological surgery. We understand that our study is only a small-scale, retrospective study and so, further randomized prospective larger trials will be required to ascertain these predictors of success or failure of laparoscopic surgery.
REFERENCES
1) Suter M, Zermatten P, Halkic N, Martinet O, Bettschart V.
Laparoscopic management of mechanical small bowel obstruction: are there predictors of success or failure? Surg Endosc 2000;14:478-483.
2) Parent S, Tortuyaux J, Deneuville M, Bresler L, Boissel P.
What are the small bowel obstructions to operate and how to do it? Acta Gastroenterol Belg 1996;59:150.
3) De Wilde R. Goodbye to late bowel obstruction after appendi- cectomy. Lancet 1991;338:1012.
4) Garrard C, Clements R, Nanney L, Davidson J, Richards W.
Adhesion formation is reduced after laparoscopic surgery. Surg endosc 1999;13:10-13.
5) Bastug DF, Trammell SW, Boland JP, Mantz EP, Tiley III EH. Laparoscopic adhesiolysis for small bowel obstruction.
Surg Laparosc Endosc 1991;1:259.
6) Chopra R, McVAY C, Phillips E, Khalili TM. Laparoscopic lysis of adhesions. Am Surg 2003;69:966-968.
7) Wullstein C, Gross E. Laparoscopic compared with conven- tional treatment of acute adhesive small bowel obstruction. Br J Surg 2003;90:1147-1151.
8) Szomstein S, Menzo EL, Simpfendorfer C, Zundel N, Rosen- thal RJ. Laparoscopic lysis of adhesions. World J Surg 2006;
30:535-540.
9) Chowbey PK, Panse R, Sharma A, Khullar R, Soni V, Baijal M. Elective laparoscopy in diagnosis and treatment of recu- rrent small bowel obstruction. Surg Laparosc Endosc 2006;16:
416.
10) Ellis H. The clinical significance of adhesions: focus on intestinal obstruction. Eur J Surg Suppl 1997:5-9.
11) Franklin M Jr, Gonzalez J Jr, Miter D, Glass J, Paulson D.
Laparoscopic diagnosis and treatment of intestinal obstruction.
Surg Endosc 2004;18:26-30.
12) Gutt C, Oniu T, Schemmer P, Mehrabi A, Buchler M. Fewer adhesions induced by laparoscopic surgery? Surg Endosc 2004;18:898-906.
13) Duepree HJ, Senagore AJ, Delaney CP, Fazio VW. Does means of access affect the incidence of small bowel obstruction and ventral hernia after bowel resection? 1::
Laparoscopy versus laparotomy. J Am Coll Surg 2003;197:
177-181.
14) Reissman P. Adhesion formation after laparoscopic anterior resection in a porcine model: a pilot study. Surg Laparosc Endosc 1996;6:136.
15) Ghosheh B, Salameh J. Laparoscopic approach to acute small bowel obstruction: review of 1061 cases. Surg Endosc 2007;21:1945-1949.
16) Levard H, Boudet MJ, Msika S, Molkhou JM, Hay JM, Laborde Y, et al. Laparoscopic treatment of acute small bowel obstruction: a multicentre retrospective study. ANZ J Surg 2001;71:641-646.
17) Benoist S, De Watteville J, Gayral F. Role of celioscopy in acute obstructions of the small intestine. Gastroenterol Clin Biol 1996;20:357.
18) Agresta F, Piazza A, Michelet I, Bedin N, Sartori C. Small bowel obstruction. Surg Endosc 2000;14:154-156.
19) Borzellino G, Tasselli S, Zerman G, Pedrazzani C, Manzoni G. Laparoscopic approach to postoperative adhesive obstruc- tion. Surg Endosc 2004;18:686-690.
20) Mathieu X, Thill V, Simoens C, Smets D, Ngongang C, Debergh N, et al. Laparoscopic Management of Acute Small Bowel Obstruction: a Retrospective Study on 156 Patients.
Hepatogastroenterology 2008;55:522-526.
21) Navez B, Arimont JM, Guiot P. Laparoscopic approach in acute small bowel obstruction. A review of 68 patients.
Hepatogastroenterology 1998;45:2146-2150.
22) Nagle A, Ujiki M, Denham W, Murayama K. Laparoscopic adhesiolysis for small bowel obstruction. Am J Surg 2004;187:
464-470.