151
책임저자:남영수, 경기도 구리시 교문동 249-1번지
471-701, 한양대학교 구리병원 외과 Tel: 031-560-2292, Fax: 031-566-4409 E-mail: [email protected]
접수일:2007년 3월 12일, 게재승인일:2007년 5월 23일 본 논문의 요지는 제58차 대한외과학회 추계학술대회에서 구연 되었음.
비전형적 급성충수염 의증 환자에서 컴퓨터단층촬영의 효용
한양대학교 의과대학 외과학교실 김민수ㆍ이강홍ㆍ남영수
The Usefulness of Computed Tomography for Patients with Equivocal Acute Appendicitis
Min Su Kim, M.D., Kang Hong Lee, M.D. and Young Su Nam, M.D.
Purpose: We wanted to determine the usefulness of computed tomography (CT) for patients with clinically-suspected but equiv- ocal acute appendicitis, and we wanted to evaluate the differ- ences of the sensitivity and specificity of CT according to the period of time from onset of the signs and symptoms to the performance of CT.
Methods: A retrospective study was done on 273 patients who visited our hospital for acute abdominal pain from Jan. 2003 to Dec. 2005, and they could not be excluded as suffering from acute appendicitis by their symptoms nor signs.
Results: Forty-three (15.8%) of the 273 patients did not under- go operation because their condition was not diagnosed as acute appendicitis and 190 patients were diagnosed as acute appendicitis by CT. The other 40 patients underwent diagnostic laparotomy because acute appendicitis could not be confirmed and any other diagnosis could not be made. The patients were classified into 6 groups according to the period of time from the onset of symptoms and signs to the performance of CT.
The sensitivity of CT after 48 hours was statistically significantly increased as compared to performing CT before 48 hours (92.3% vs. 75.8%, respectively; P=0.023).
Conclusion: Forty-three (15.8%) of the patients with clinically- suspected but equivocal acute appendicitis avoided unnecessary laparotomy by undergoing CT. The sensitivity was increased for diagnosing acute appendicitis by CT when it was performed af- ter 48 hours from the onset of symptoms and signs, but caution may be needed during interpretation because of the false pos- itives (2 patients;4.7%) could due to secondary change of other diseases. (J Korean Surg Soc 2007;73:151-155)
Key Words: Acute appendicitis, Computed tomography 중심 단어: 급성충수염, 컴퓨터단층촬영
Department of Surgery, Hanyang University College of Medicine, Seoul, Korea
서 론
급성충수염은 수술을 요하는 급성 복증의 가장 흔한 원 인 질환 중 하나이다. 급성충수염 진단은 병력청취와 이학 적 검사가 가장 중요하지만, 급성충수염의 22∼33%는 비전 형적인 증상과 증후를 보이므로 영상적 진단 방법을 이용 하기도 한다.(1,2) 그러나 컴퓨터단층촬영은 급성충수염 진 단에 양성예측도 향상 및 음성 개복률 저하에 도움이 되지 않고 오히려 진단이 늦어짐으로 인한 수술 지연으로 술 후 합병증을 늘릴 수도 있으므로 급성충수염 진단에 컴퓨터단 층촬영의 일상적 활용보다는 선택적 활용을 강조하게 되었 다.(3-8)
급성충수염의 비전형적인 증상, 증후를 보이는 환자에서 컴퓨터단층촬영은 안전하면서도 진단의 정확도를 높여 불 필요한 개복술을 줄일 수 있으며 불필요한 검사 빈도와 입 원 기간을 줄임으로써 환자 치료 및 병원 자원 활용의 효용 성을 높일 수 있다는 보고들이 있다.(6-9) 이에 저자들은 급 성 복증을 주소로 내원한 환자 중, 증상과 증후로 급성충수 염을 배제할 수 없었던 환자에서 컴퓨터단층촬영의 효용성 과 컴퓨터단층촬영 시기에 따른 민감도, 특이도의 차이를 알아보고자 하였다.
방 법
2003년 1월부터 2005년 12월까지 급성 복증을 주소로 내 원한 833명의 환자 중, 403명(48.4%)은 증상과 증후를 토대 로 급성충수염으로 진단하여 충수돌기 절제술을 시행하였 고 273명(32.8%)은 증상, 증후로 급성충수염을 배제할 수 없어 컴퓨터단층촬영을 시행하였다. 컴퓨터단층촬영기는 동일 기종(Giemens 사의 somatom sensation 16 channel)으로 모든 대상 환자는 경구 조영제 없이 혈관 조영제 Schering 사의 ultravist 370를 사용하였으며, 복부 및 골반 촬영이 5
Table 2. Characteristics of abdominal pain
*N †D ‡E §U ∥R ¶L Patients (no.) *N †D ‡E §U ∥R ¶L Patients (no.)
+ + 16 + 14
+ + 3 + 4
+ + 0 + 69
+ + 0 + 18
+ + 1 + + 15
+ 96 + + 8
+ + 29
*N = nausea; †D = diffuse abdominal pain; ‡E = epigastric pain; §U = periumbilical pain; ∥R = right lower quadrant pain; ¶L = lower abdominal pain.
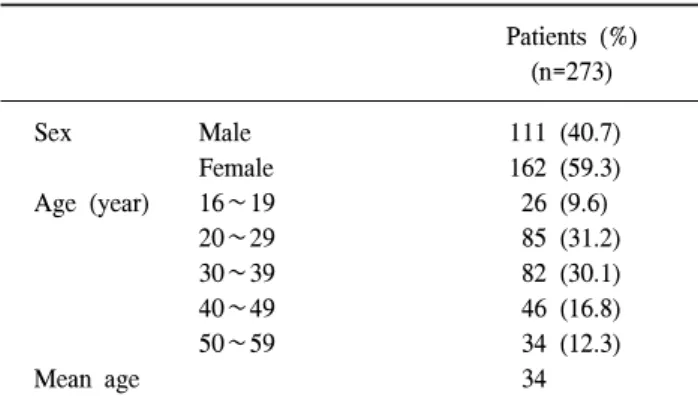
Table 1. Characteristics of the patients Patients (%)
(n=273)
Sex Male 111 (40.7)
Female 162 (59.3)
Age (year) 16∼19 26 (9.6)
20∼29 85 (31.2)
30∼39 82 (30.1)
40∼49 46 (16.8)
50∼59 34 (12.3)
Mean age 34
Table 3. Interpretation of computed tomography (CT) and treatment
Patients (%)
CT interpretation Treatment
(n=273)
Acute appendicitis excluded 43 (15.8) No operation Acute appendicitis 190 (69.6) Appendectomy Non-specific 40 (14.6) Explo-laparotomy mm 간격으로 이루어졌다.
이 연구는 273명의 의무기록을 후향적으로 분석하였다.
임산부는 제외하였고, 정확한 증상 및 증후를 표현하기 힘 든 15세 이하 및 고령으로 인한 동반 질환 감별을 위해 컴퓨 터단층촬영을 시행하는 60세 이상도 제외하였다. 전형적 급성충수염 증상과 증후란 오심을 동반한 심와부 통증이 배꼽주위로 이동한 후 우하복부로 이동하며 진찰 소견상 우하복부 압통이 있는 경우로 정의하였다.
내원한 환자들의 컴퓨터단층촬영 시행 여부는 외과 전공 의가 결정하였고, 3년차 이상의 방사선과 전공의 혹은 방사 선과 전문의가 판독하였고, 대상 환자들의 수술 및 퇴원 여 부는 외과 4년차 전공의나 외과 전문의가 결정하였다.
수술을 시행하였던 환자의 진단은 조직학적 소견에 기초 하였고, 급성충수염이 아니었던 경우는 수술 전후 및 수술 소견을 종합하여 진단하였다. 수술을 시행하지 않은 경우 는 입원 기간 중이나 퇴원 시의 임상적 증상과 컴퓨터단층 촬영 소견을 기초로 하였다. 컴퓨터단층촬영에서 급성충수 염의 진단기준은 충수돌기 벽의 비후 및 조영 증가가 있으 면서 충수돌기의 직경이 6 mm 이상으로 확장되거나 결석을 동반하는 경우를 기준으로 하였다. 컴퓨터단층촬영의 소견 은 급성충수염, 다른 질환, 비특이적인 경우(급성충수염 및 타 질환으로 명확히 진단하지 못한 경우)로 분류하였다.
환자의 증상 발현 후 컴퓨터단층촬영 검사까지의 시간에 따라 컴퓨터단층촬영의 민감도나 특이도의 차이가 있을 것 이라는 가정하에, 환자들을 증상과 증후 시작부터 컴퓨터 단층촬영 시행까지 8시간 이내, 8∼16시간, 16∼24시간, 24
∼48시간, 48∼72시간, 72시간 이상의 6군으로 나누었다.
각 군에 대한 컴퓨터단층촬영의 민감도, 특이도, 정확도 를 산출하였고 통계학적 분석은 SPSS 12.0 for Windows program 중 Mann-Whitney U test를 이용하여 각 군 간의 차 이를 비교하였고, 유의수준은 95%로 정의하였다.
결 과
1) 대상 환자의 인구학적 특성 및 증상
대상 환자는 273명이었고 평균 연령은 34세(16∼59세)이 고 성별은 남자 111명, 여자 162명(남:녀=1:1.5)이었다 (Table 1). 대상 환자 모두에서 진찰 소견상 우하복부 압통 은 있었고, 각 증상 양상은 Table 2에 제시하였다(Table 2).
2) 컴퓨터단층촬영 판독 및 치료
증상과 증후로 급성충수염을 배제할 수 없어 컴퓨터단층 촬영을 시행했던 273명 환자들 중, 43명(15.8%)은 타 질환 으로 진단되어 수술을 시행하지 않았다(Table 3). 43명 중 골반염이 28명(65.1%), 게실염이 7명(16.3%), 장염이 5명 (14.7%)이었으며, 난소 낭종, 자궁 내막증, 자궁 근종이 각 각 1명(2.9%)이었다(Table 4). 190명(69.6%)은 급성충수염으
Table 4. Diagnosis in patients which acute appendicitis was excluded in CT
Diagnosis Patients (%) (n=43)
Pelvic inflammatory disease 28 (65.1)
Diverticulitis 7 (16.3)
Colitis 5 (14.7)
Ovarian cyst 1 (2.9)
Endometriosis 1 (2.9)
Uterine myoma 1 (2.9)
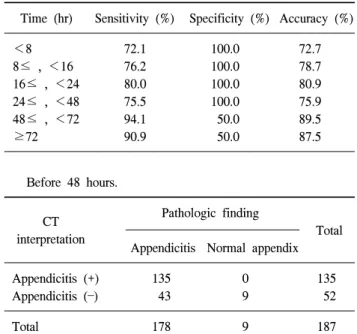
Table 8. Sensitivity, specificity, accuracy according to time of performing CT
Time (hr) Sensitivity (%) Specificity (%) Accuracy (%)
<8 72.1 100.0 72.7
8≤ , <16 76.2 100.0 78.7
16≤ , <24 80.0 100.0 80.9
24≤ , <48 75.5 100.0 75.9
48≤ , <72 94.1 50.0 89.5
≥72 90.9 50.0 87.5
Before 48 hours.
Pathologic finding
CT Total
interpretation
Appendicitis Normal appendix
Appendicitis (+) 135 0 135
Appendicitis () 43 9 52
Total 178 9 187
Sensitivity: 75.8%, Specificity: 100.0%, Accuracy: 77.0%.
After 48 hours.
Pathologic finding
CT Total
interpretation
Appendicitis Normal appendix
Appendicitis (+) 36 2 38
Appendicitis () 3 2 5
Total 39 4 43
Sensitivity: 92.3%, Specificity: 50.0%, Accuracy: 88.4%.
<48 hr >48 hr P-value
Sensitivity (%) 75.8 92.3 0.023
Specificity (%) 100.0 50.0
Accuracy (%) 77.0 88.4
Table 5. Diagnosis after explo-laparotomy in patients with non-specific finding in CT
Diagnosis Patients (%) (n=40)
Acute appendicitis 29 (72.5)
Non-specific 9 (22.5)
Pelvic inflammatory disease 2 (5.0)
Table 6. Sensitivity, specificity, accuracy of CT Pathologic finding
CT Total
interpretation
Appendicitis Normal appendix
Appendicitis (+) 171 2 173
Appendicitis () 46 11 57
Total 217 13 230
Sensitivity: 171/217×100=78.8%, Specificity: 11/13×100=84.6%, Accuracy: 182/230×100=79.1%.
Table 7. Time from onset of symptom to the performance of CT in patients who underwent operation
Time (hr) Patients (%) (n=230)
<8 44 (19.1)
8≤ , <16 47 (20.4)
16≤ , <24 42 (18.3)
24≤ , <48 54 (23.5)
48≤ , <72 19 (8.3)
≥72 24 (10.4)
로 진단하고 충수돌기 절제술을 시행하였는데, 188명 (98.9%)은 병리학적으로 급성충수염이 확인되었고, 2명 (1.1%)은 각각 게실염, 복막중피종이었다. 나머지 40명 (14.6%)은 급성충수염으로 확신할 수는 없었으나 다른 진 단도 확신할 수 없어 진단적 개복술을 시행하였는데, 29명
(72.5%)는 급성충수염이었으며 11명(27.5%)은 급성충수염 이 아니었다. 2명은 골반염으로, 9명은 특정 진단을 확정할 수 없었고 수술 후 증상 호전이 있어 퇴원하였다(Table 5).
수술을 시행한 230명에서 컴퓨터단층촬영의 민감도는 78.8%였고, 특이도는 84.6%, 정확도는 79.1%였다(Table 6).
230명의 환자들을 증상과 증후 시작부터 컴퓨터단층촬영 시행까지 시간에 따라 6군으로 나누었을 때, 각 시간대별 환자 수는 44명(19.1%), 47명(20.4%), 42명(18.3%), 54명 (23.5%), 19명(8.3%), 24명(10.4%)이었다(Table 7). 각 시간대 별 컴퓨터단층촬영의 민감도, 특이도, 정확도를 산출하여
군 간 비교해 본 결과, 증상과 증후 발현 48시간 이후에 시 행하는 경우와 이전에 시행하는 경우에 민감도가 92.3%, 75.8%로 유의한 차이가 있었다(P=0.023)(Table 8). 컴퓨터단 층촬영이 위양성으로 나타난 경우는 증상, 증후 발현 후 검 사 시행하기 48시간 이전에는 없었으나 48시간 이후에는 2 명(4.7%)이었다.
고 찰
급성충수염은 응급 개복술을 시행하는 흔한 원인 중 하 나지만, 복통을 유발하는 다른 원인과 감별이 어려울 때가 있고 음성 개복률이 15∼30%로 보고되고 있다.(3,7) 급성충 수염 진단은 환자의 자세한 병력 청취와 이학적 검사가 가 장 중요하다.(10) 특히, 급성충수염 환자 중 50∼60% 경우 에는 전형적인 증상, 증후를 보이므로 영상 검사 없이 임상 적 진단만으로 수술을 결정하고 있다.(1,5) 하지만 비전형적 인 증상, 증후를 보이는 환자는 다른 진단법의 도움 없이 임상적 진단만으로 수술을 결정하기는 쉽지 않다. 급성충 수염 의증 환자에서 임상적 진단법만을 사용한 경우의 음 성 개복률(24%)보다 컴퓨터단층촬영을 시행한 경우의 음성 개복률(16%)이 유의하게 낮았다는 보고가 있다.(11,12) 컴 퓨터단층촬영을 시행하지 않고 환자의 증상이 뚜렷해질 때 까지 경과를 지켜보는 것 또한 추천되지 않는데, 이는 충수 돌기 천공률을 높혀 술 후 합병증을 증가시키고 불필요한 환자 비용을 늘리며 병원 자원의 효율적 이용이 어려워진 다.(7)
급성충수염 진단에 도움이 될 수 있는 검사로는 혈액검 사(백혈구 수 측정, C-reactive protein 검사), 임상적 점수제, 컴퓨터단층촬영과 초음파를 포함한 각종 영상검사, 진단적 복강경 등이 있다. 하지만 혈액검사, 임상적 점수제 등은 비 특이적일 수 있고 확진을 위한 검사로 한계가 있다. 급성충 수염 의증 환자에서 임상적 점수제, 혈액검사, 단순 복부 촬 영, 바륨 조영 등의 검사법들의 한계점을 언급하면서, 컴퓨 터단층촬영이 정확도와 판독 신뢰도가 높고 짧은 시간에 가능하여 비용-효율성면에서 타 검사들보다 우월하다는 보 고가 있다. 이런 이유로 급성충수염 의증 환자에서 일상적 으로 컴퓨터단층촬영을 시행하여 불필요한 수술을 피하고 신속한 진단을 통해, 환자의 치료 향상과 병원 자원의 효율 적 활용을 언급하고 있다.(8,13) 컴퓨터단층촬영은 증상, 증 후가 비특이적인 환자들에서 음성 개복률을 줄이고, 빠른 진단을 통해 수술과 퇴원을 조기에 결정할 수 있는 장점이 있다.(6-8,11) 본 조사에서도 15.8% 환자들이 컴퓨터단층촬 영을 통해 불필요한 수술을 피할 수 있었다. 다른 연구에서 의 민감도(90∼95%), 특이도(97∼100%), 정확도(95∼98%) 에 비해 본 연구에서는 민감도(78.8%), 특이도(84.6%), 정확 도(79.1%)가 비교적 낮게 산출되어 결과 해석에 한계가 있 긴 하지만, 증상, 증후 발현부터 48시간 이후에는 민감도
(92.3%)가 그 이전(75.8%)에 비해 유의하게 높기 때문에 효 용성이 더욱 높다고 볼 수 있다. 하지만 48시간 이후에는 컴퓨터단층촬영이 타 질환에 의한 염증 파급으로 위양성이 나타날 수 있다.
결 론
증상, 증후로 급성충수염을 배제할 수 없었던 환자에서 컴퓨터단층촬영은 43명(15.8%)의 경우에 불필요한 개복술 을 피할 수 있었다. 증상과 증후 시작부터 48시간 이후에는 이전에 비해 컴퓨터단층촬영이 급성충수염 진단하는 데 민 감도가 증가하여 추천되는 검사법이지만, 타 질환에 의한 2차적 변화로 위양성이 나올 수 있으므로 해석에 신중을 요한다.
REFERENCES
1) Poh AC, Lin M, Teh HS, Tan AG. The role of computed to- mography in clinically-suspected but equivocal acute appen- dicitis. Singapore Med J 2004;45:379-84.
2) Wijetunga R, Tan BS, Rouse JC, Bigg-Wither GW, Doust BD.
Diagnostic accuracy of focused appendiceal CT in clinically equivocal cases of acute appendicitis. Radiology 2001;221:
7647-53.
3) Lee SL, Walsh AJ, Ho HS. Computed tomography and ultra- sonography do not improve and may delay the diagnosis and treatment of acute appendicitis. Arch Surg 2001;136:556-60.
4) Hong JJ, Cohn SM, Ekeh AP, Newman M, Salama M, Leblang SD. A prospective randomized study of clinical assessment versus computed tomography for the diagnosis of acute appendicitis. Surg Infect 2003;4:231-9.
5) Bendeck SE, Nino-Murcia M, Berry GJ, Jeffrey RB Jr.
Imaging for suspected appendicitis: negative appendectomy and perforation rates. Radiology 2002;225:131-6.
6) Jacobs JE. CT and sonography for suspected acute appen- dicitis. Am J Roentgenol 2006;186:1094-6.
7) Rao PM, Rhea JT, Novelline RA, Mostafavi AA, McCabe CJ.
Effect of computed tomography of the appendix on treatment of patients and use of hospital resources. N Engl J Med 1998;338:141-6.
8) Wilson EB, Cole JC, Nipper ML, Cooney DR, Smith RW.
Computed tomography and ultrasonography in the diagnosis of appendicitis: When are they indicated? Arch Surg 2001;136:
670-5.
9) Birnbaum BA, Wilson SR. Appendicitis at the millennium.
Radiology 2000;215:337-48.
10) John H, Neff U, Kelemen M. Appendicitis diagnosis today:
clinical and ultrasonic deductions. World J Surg 1993;17:
243-9.
11) McDonald GP, Pendarvis DP, Wilmoth R, Daley BJ. Influence of preoperative computed tomography on patients undergoing
appendectomy. Am Surg 2001;67:1017-21.
12) Ujiki MB, Murayama KM, Cribbins AJ, Angelos P, Dawes L, Prystowsky JB, et al. CT scan in the management of acute appendicitis. J Surg Res 2002;105:119-22.
13) Malik AA, Wani NA. Continuing diagnostic challenge of acute appendicitis: Evaluation through modified Alvarado score.
Aust N Z J Surg 1998;68:504-5.