Vol. 9, No. 1, March, 2002
자가조혈모세포이식을 이용한 불응성 류마티스 관절염의 치료
가톨릭대학교 의과대학 류마티스 센터, 조혈모세포이식 센터*, 신경과학교실* *
민도준・민창기*・양동원* *・윤종현・김완욱・이상헌・김동욱*
이종욱*・조철수・김호연・김춘추*
─A b s t r a c t─
Autologous Hematopoietic Stem Cell Transplantation for Treatment of Refractory Rheumatoid Arthritis
Do-June Min, M.D., Chang-Ki Min, M.D.*, Dong Won Yang, M.D.**, Chong-Hyeon Yoon, M.D., Wan-Uk Kim, M.D., Sang-Heon Lee, M.D.,
Dong Wook Kim, M.D.*, Jong Wook Lee, M.D.*, Chul-Soo Cho, M.D., Ho-Youn Kim, M.D., Chun Choo Kim, M.D.*
The Center for Rheumatic Diseases, Catholic Hemopoietic Stem Cell Transplatation Center*, Department of Neurology**, Catholic University Medical College, Seoul, Korea
O b j e c t i v e : To investigate the safety and efficacy of immunoablation and subsequent autologous hematopoietic stem cell transplantation (HSCT) in refrac- tory rheumatoid arthritis (RA).
M e t h o d s : Three patients with severe, refractory RA were treated. We mobilized autologous hematopoietic stem cells (HSCs) with cyclophosphamide (Cy) and granulocyte colony-stimulating factor. HSCs were collected and enriched ex vivo using CD34-positive immunoselection. Two different immunoablative conditioning regimens were employed; fludarabine-Cy-anti-thy- moayte glonulin (ATG) in patients whose disease activity was transiently ame- liorated in response to Cy used in stem cell mobilization, or fludarabine-busul- fan-ATG in those who didn’t show any response to that.
<접수일 : 2001년 12월 23일, 심사통과일 : 2002년 1월 31일>
※통신저자 : 민이도이준
서울특별시 영등포구 여의도동 62번지 가톨릭대학교 의과대학 성모병원 내과학교실
Tel : 02) 3779-1663, Fax : 02) 780-3132, E-mail : [email protected]
서 론
류마티스 관절염(rheumatoid arthritis, RA)은 전신적 자가면역질환으로서, 이의 치료를 위하여 다 양한 방법이 사용되고 있으나, 일부 환자들은 치료 에 불응하여 심각한 장애 또는 수명 단축이 초래된 다1 ). 최근, 기존의 치료에 불응하여 예후가 불량할 것으로 예측되는 자가면역질환 환자에서 고용량 면 역억제 및 조혈모세포이식이 새로운 대안으로 제시 되고 있다2 , 3 ). 자가면역질환에서의 조혈모세포이식은 고용량 화학요법 또는 화학・방사선요법으로 골수 및 면역세포를 제거한 뒤, 조혈모세포를 주입하여 새로운 면역세포로 분화하게 함으로써 면역체계를 재구성하는 방법이다. 이 치료법이 도입된 배경은, 자가면역질환 동물 모델에서 동종(allogeneic), 동 계(syngeneic) 및 자가(autologous) 골수이식 후 완전관해가 유도되는 고무적인 결과가 보고된 바 있
었고4 , 5 ), 혈액 질환의 치료 목적으로 골수이식을 받
은 환자들에서 동반된 자가면역질환의 관해가 관찰 된 된 것이 계기가 되었다6 - 9 ). 그러나 동종골수이식 은 높은 치료관련 사망률 및 이식편대숙주반응 등과 같은 합병증으로 인하여 자가면역질환의 치료에 적 용되기 어려운 문제점을 내포하고 있으므로, 현재로 서는 자가조혈모세포이식이 권장되고있다1 0 , 1 1 ).
1 9 9 6년 European League against Rheumatism
( E U L A R )와 European Group for Blood and Marrow Transplantation (EBMT)를 중심으로 International Autoimmune Disease Stem Cell P r o j e c t가 발족되어 자가면역질환에서 고용량 면역억 제요법 및 조혈모세포이식의 안전성 및 치료 효과에 대한 연구가 진행되어, 현재까지 2 0개국 6 4센터에서 8 0여명의 RA 환자를 비롯한 5 0 0여명의 자가면역질환 환자들이 이 치료를 받았으며1 2 , 1 3 ), 국내에서는 저자 등 이 다발성 경화증 및 RA 환자 각 1명에서 자가조혈모 세포이식을 시행하여 보고한 바 있다1 4 ). 본 연구에서는 이 임상 시험의 일환으로, 이전에 보고했던 환자의 추 적 관찰을 포함하여 3명의 불응성 RA 환자들을 대상 으로 고용량 면역억제에 이은 자가조혈모세포이식을 시행한 후 그 안전성과 치료 효과를 조사하였다.
대상 및 방법
1. 대상환자 선정 기준
연령이 6 0세 이하이고, 미국 류마티스학회( A m e r i- can college of rheumatology, ACR)에서 1 9 8 7년에 제정한 류마티스 관절염 진단기준1 5 )에 합당하며, 혈청 류마티스 인자 양성이면서, 두 가지 이상의 항류마티 스제(disease-modifying anti-rheumatic drugs, DMARDs) 치료에 실패한 환자를 대상으로 하였다.
DMARDs 치료 실패의 정의는 종창관절 수 ≥6 ( 6 6개 관절 중)이면서, 침범관절(종창, 압통, 운동 시 통증, R e s u l t s : Median time to engraftment with an absolute neutrophil count greater than 500/μl and nontransfused platelet count greater than 20,000/μl was 15 days (range 12-16) and 9 days (range 7-13), respectively. Regimen-related toxicity was minimal. Two patients were markedly improved at 2 or 3 months after HSCT, repectively. In another patient, disease activity was transiently subsided, but relapsed at 2 months after HSCT, which led to reinstitution of anti-rheumatic medications. This resulted in subsequent marked improvement of disease activity whereas her disease had been refractory to these medications.
C o n c l u s i o n s : These results underscore the feasibility and potential efficacy of intensive immunosuppression followed by autologous HSCT for treatment of refrac- tory rheumatoid arthritis. The durability of remission remains to be clarified.
Key Words : Autologous hematopoietic stem cell transplantation, Immunoablation, Rheumatoid arthritis
운동범위 제한) 수가 ≥3 0 ( 6 8개 관절 중)이거나 2 0 Health Assessment Questionnaire (HAQ) 문항 중 어려움 없이 수행할 수 있는(without any diffi- culty) 문항이 <7 5 %인 경우로 하였다1 6 ).
2. 말초혈액 조혈모세포 가동화 및 채집
Cyclophosphamide (Cy) 4g/m2정맥 투여 후 7 일째부터 granulocyte colony stimulating factor (G-CSF) 10μg / k g / d a y를 피하 주사하였다. Flow cytometry (FACSCaliburTM, Becton Dickin- son, San Jose, Calif., USA) 검사 상 말초혈액 CD34+ 세포 수가 2 0 /μl 을 초과하는 날부터 백혈구 반출술을 시행하여 단핵세포를 채집하였으며, 면역자 기적 방법(immunomagnetic method)으로 C D 3 4 + 세포를 순수 분리하였다(CliniMACS system, Mil- tenyi Biotec, Bergisch Gladbach, Germany).
채집된 조혈모세포는 - 7 0°C에서 냉동 저장되었다.
3. 전처치
전처치는 f l u d a r a b i n e과 anti-thymocyte globulin ( A T G )를 근간으로 하여, 말초혈액 조혈모세포 가동화 에 사용된 고용량의 C y에 의한 질병 활성도 완화 여부 에 따라 Cy 또는 b u s u l f a n을 병합하였다. 즉, 조혈모 세포 가동화 후 ACR 20% 반응 기준1 7 )을 만족시키는
호전을 보일 경우, fludarabine 30mg/m2/day (day -8 to -4), ATG 1.25mg/kg/day (day-8, -6, -4, - 2 )에 Cy 60mg/kg/day (day-3 to -2)를 병합하였고, 그렇지 않을 경우 C y을 제외하고 f l u d a r a b i n e 30mg/m2/day (day -7 to -2), ATG 2.5mg/
kg/day (day-4 to -1) 및 busulfan 4g/kg/day (day-6 to -5) 병합요법을 사용하였다. ATG를 투여 하는 동안 혈청병(serum sickness)을 예방하기위해 methylprednisolone 125mg/day를 정맥 주사하였다.
4. 이식 전후의 보조요법
전처치 시작 전 공기여과시설을 갖춘 병실( l a m i n a r air flow room by HEPA filter)에 입원하여 멸균 식과 선택적 장내무균화를 위한 경구 항생제 및 항진 균제 그리고 항바이러스제를 투여 받았다. DMARDs 및 비스테로이드성 항염제는 이식 전에 모두 중단하였 으며, 스테로이드는 이식 후 서서히 감량하였다.
5. 세포표면항원 flow cytometry
조혈모세포 이식 전후에 말초혈액의 CD4+ 및 C D 8 + 림프구 아형 분포의 변화를 조사하였다. Phycoery- thrin (PE)에 결합된 mouse monoclonal antibody (anti-CD4, anti-CD8)로 single staining을 시행하 였으며, flow cytometer FACSCaliburT M ( B e c t o n Table 1. Characteristics of the patients before hematopoietic stem cell transplantation (HSCT)
Patient 1 Patient 2 Patient 3
Age, years 2 3 4 0 3 7
S e x F F F
Diseae duration, years 6 3 3
Treatment just prior to HSCT* M T X+B U C M M T X+H C Q+B U C M M T X+A Z P+H C Q
Previous treatment* M T X+A Z P
M T X+B U C M M T X+C S A M T X+H C Q+g o l d
M T X+H C Q+S S Z M T X+H C Q+S S Z M T X+H C Q
M T X+H C Q M T X+H C Q+g o l d
RF, IU/ml
(normal values < 15 IU/ml) 1 3 2 3 1 0 2 0 7
Radiologic finding of RA Y e s Y e s Y e s
No. of tender/Swollen joints 2 7 / 1 2 2 4 / 1 2 3 9 / 1 4
No. of “without any difficulty”in HAQ 4 2 1
M T X=methotrexate; BUCM=bucillamine; HCQ=hydroxychloroquine; AZP=azathioprine; CSA=
cyclosporin A; SSZ=sulfasalazine; RF=rheumatoid factor; RA=rheumatoid arthritis, HAQ=H e a l t h Assessment Questionnaire
*All patients were also taking nonsteroidal anti-inflammatory drugs and low dose corticosteroid.
Dickinson, San Jose, Calif., USA)를 이용하여 분 석하였다.
결 과
1. 대상 환자의 특성
세 환자 모두 1987 ACR 진단 기준에 합당하였 고, 혈청 류마티스 인자 양성이었으며, 특징적인 방 사선 소견(관절주위 골감소증, 관절간격 협소, 골 미 란)을 보이는 활동성의 RA 환자이었다. 모든 환자 에서 4 종류 이상의 다양한 DMARDs 및 스테로이 드와 비스테로이드성 항염제 등이 지속적으로 투여 되어왔으나, 이에 반응하지 않고 기능적 장애 및 방 사선 소견이 진행하는 양상을 보였다. 이식 전 3 환 자 모두 2 0문항의 HAQ 중 “without any diffi- c u l t y”반응이 4문항 이하이었다(표 1 ) .
2. 이식의 특성
채집한 단핵세포에서 CD34+ 세포의 분리 후, CD34+ 세포 수는 환자 1, 2, 3에서 각각 2 9 . 7×
1 06/ k g (전체 단핵세포의 99.76%), 3.7×1 06/ k g (99.50%), 3.8×1 06/kg(99.50%) 이었다. 또한 CD3+ 세포 수는 1 . 9×1 04/ k g (전체 단핵세포의 0.07%), 0.5×1 04/kg(0.15%), 0.5×1 04/ k g (0.09%) 이었다(표 2 ) .
전처치로, 환자 1은 C y가 투여된 조혈모세포 가 동화 후에도 질병 활성도가 전혀 호전되지 않아, f l u d a r a b i n e과 A T G에 b u s u l f a n을 병합하였으며, 환자 2와 3은 조혈모세포 가동화 후 ACR 20% 반 응 기준을 만족시키는 호전을 보여, fludarabine - ATG-Cy 병합요법을 사용하였다.
3. 생착
이식된 조혈모세포의 생착은 모든 환자에서 성공 Table 2. Transplant Characteristics
Patient 1 Patient 2 Patient 3
C D 3 4+c e l l s ,
29.7 (99.76) 3.7 (99.50) 3.8 (99.50)
×1 06/ k g ( % ) C D 3+c e l l s ,
0.019 (0.07) 0.005 (0.15) 0.005 (0.09)
×1 06/ k g ( % )
C o n d i t i o n i n g F l u+B u+A T G F l u+C y+A T G F l u+C y+A T G F l u=fludarabine; Bu=busulfan; ATG=anti-thymocyte globulin; Cy=c y c l o p h o s p h a m i d e
Fig. 1. Clinical course of patients after hematopoietic stem cell transplantation (HSCT). A, Number of tender joints; B, Number of swollen joints. Patient 1 was treated with antirheumatic medica- tions since 3 months after HSCT.
A B
적으로 이루어졌다. 환자 1, 2, 3에서 이식 후 호중 구가 5 0 0 /μl 이상으로 회복되는 시점은 이식일로부 터 각각 1 5일, 16일, 9일째이었고, 혈소판은 각각 9. 13, 7일째에 2 0 , 0 0 0 /μl 이상으로 회복되었다.
4. 부작용 및 합병증
오심 및 탈모는 모든 환자에서 발생하였다. 환자 1 은 말초혈액 조혈모세포 가동 후 배부에 대상포진이 발생하였으며, famciclovir를 7일간 경구 투여 후 호전되었다. 환자 3은 이식 직후 중심정맥 카테터 삽 입부에 정맥혈전이 발생하여 항응고치료를 받았다.
환자 2의 경우 이식 1개월 후 cytomegalovirus 항 원혈증이 발견되어, ganciclovir를 2주간 투여받은 후 혈액에서 항원이 음전환 되었다. 그 외에 중증 감 염을 비롯한 심각한 독성은 발생하지 않았다.
5. 치료 효과
조혈모세포이식 1개월 후에 3환자 모두 A C R 50% 반응 기준을 만족시키는 뚜렷한 호전을 보였다 (그림 1). 환자 1은 1개월째 관절통 및 조조강직을 호소하지 않았고, 압통은 1관절, 종창은 2관절에만 남아있었다. 그러나 2개월째부터 관절염 활성이 다 시 나타나기 시작하여 3개월째에는 압통관절 수가 15, 종창관절 수가 9이었으며, 이 때부터 다시 DMARD (methotrexate, MTX; 7.5mg/week) 를 투여하기 시작하였다. 이식 전에는 고용량의
M T X를 포함한 DMARDs 병합요법에도 반응하지 않은데 비해, 이식 후 저용량의 M T X에 뚜렷이 반 응하여 6개월째에 ACR 50 기준을 만족시켰으며, 9 개월째에는 관절압통 및 종창이 관찰되지 않았다.
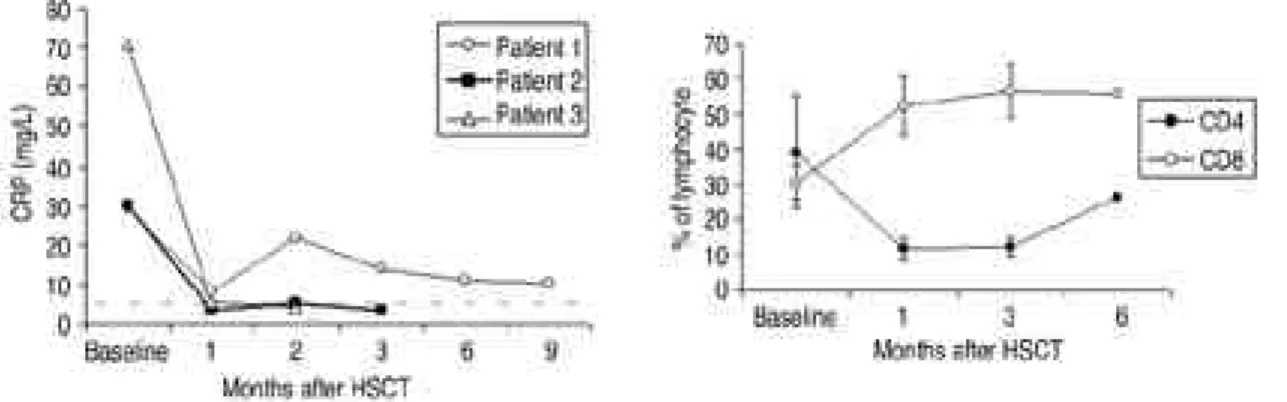
환자 2는 이식 1주후 관절 압통 및 종창이 완전히 소실되었으며, 관해 상태가 3개월까지 유지되고있 다. 혈청 C -반응단백(C-reactive protein, CRP) 역시 이식 직후부터 정상화되어 유지되었다(그림 2). 비스테로이드계 항염제 및 D M A R D s는 이식 전에 모두 중단하였고, 이식 3개월 후 현재 p r e d- nisolone 5mg/day 만 복용 중이며 점차 감량하여 중단할 계획이다.
환자 3 역시 이식 후 뚜렷한 반응을 보여, 1개월 후에 ACR 50을 만족시켰으며, 2개월 후 압통은 4 관절에만 경미하게 남아있었고 종창은 관찰되지 않 았다(ACR 70). 이식 직후 혈청 C -반응단백( C - reactive protein, CRP)은 정상화되었고, 류마티 스 인자가 음전환 되었다. 이식 2개월 후 현재 prednisolone 5mg/day 만 복용 중이다.
6. 면역재구성
세포표면 항원에 대한 flow cytometry 분석 상, 세 환자 모두에서 이식 전에는 CD4+ 세포가 C D 8 + 세포에 비하여 우세하였으나, 이식 후에 C D 4 : C D 8 비가 역전되어 유지되는 것이 관찰되었다(그림 3 ) . Fig. 2. Serum C-reactive protein (CRP) levels
before and after HSCT. Horizontal dashed line indicates the cut-off value. Patient 1 was treated with antirheumatic medica- tions since 3 months after HSCT.
Fig. 3. Kinetics of CD4+ and CD8+ lymphocyte subsets following HSCT. Values represent the mean and SD.
고 찰
저자들은 기존의 치료에 불응하여 진행하는 류마 티스 관절염 환자들에서 고용량 면역억제에 이은 자 가조혈모세포이식을 시행하여, 모든 환자에서 심각 한 독성 없이 질병 활성이 뚜렷이 호전됨을 관찰하 였다. 2명의 환자에서는 이식 후 각각 2개월 및 3개 월 후까지 관절염의 활성이 소실되었다. 다른 1명에 서는 일시적으로 호전된 뒤 질병 활성의 재발이 관 찰되었으나, 이전에 반응하지 않던 항류마티스 약제 에 두드러진 반응을 보여 현저히 호전되는 질병 감 쇠(disease attenuation) 효과를 나타내었다.
자가면역질환에서 조혈모세포이식의 방법은 아직 정립되지 않았으나, 조혈모세포의 근원으로는 말초 혈액이 선호되고 있다. 말초혈액 조혈모세포는 골수 세포에 비하여 생착이 빠르고, 전신마취 및 골수천 자로 인한 합병증을 피할 수 있는 장점이 있다. 말초 혈액으로의 조혈모세포 가동화를 위한 방법은 몇 가 지가 있으나 최근에는 Cy 및 G-CSF 투여가 널리 사용된다. Cy를 투여하는 목적은 말초혈액내의 조혈 모세포 비율을 증가시키고, 자가면역질환의 활성을 1차적으로 조절하기 위함이다. 류마티스 관절염 환 자에서도 4 g / m2의 Cy 및 G - C S F를 이용한 가동화 가 비교적 안전하며, 가동화를 위한 Cy 투여만으로 6개월 이상 임상적 호전이 지속될 수 있는 것으로 보고된 바 있다1 8 ). 본 환자들에서도 이 방법으로 말 초혈액 내로 조혈모세포를 가동하였으며 중증의 독 성 없이 충분한 양의 조혈모세포 채집이 가능하였 다. 세 환자 중 2명에서 가동화를 위한 Cy (7g, 4 g / m2) 투여 후 관절염이 호전되었으며, 특히 환자 2는 일시적으로 관절염 활성이 완전 소실되었다.
조혈모세포 채집 시 T 세포를 제거하지 않고 재주 입시 자가면역질환이 조기에 재발하였다는 보고 이후
1 9 ), 채집한 단핵세포로부터 림프구를 제거하고 조혈
모세포만을 재주입하는 방법이 권장되고있다. 조혈모 세포를 분리하는 방법은 T 세포 및 B 세포를 제거하 는 방법(negative depletion) 또는 CD34 양성 세 포를 순수 분리하는 방법(positive selection)이 있
으며2 0 ), 후자가 널리 사용되고 있고 저자들도 후자의
방법을 이용하였다. 그러나 이러한 림프구 제거 조작 이 치료 성적 향상과 결부되는 지는 입증되지 않았
고, 림프구 감소 상태를 장기화하여 감염에 대한 감 수성을 증가시킬 수 있다는 우려도 있다2 1 ).
자가면역질환에서의 조혈모세포이식 전처치는 C y 단독 투여 또는 A T G와의 병합요법, Cy+전신 방사 선 조사요법, Cy+busulfan 등 C y을 근간으로 한 요법 및 BEAM (BCNU+e t o p o s i d e+c y t o s i n e a r a b i n o s i d e+melphalan) 화학요법 등이 널리 사 용되고 있으나, 질환별로 최적의 전처치 방법이 정 립되지 않았다2 2 ). 류마티스 관절염의 경우 루푸스나 전신성 경화증 등의 다른 자가면역질환들에 비하여 질환 자체에 의한 사망률이 높지 않은 이유로, 전처 치 요법 중 비교적 독성이 적은 Cy 단독 요법 혹은 C y+ATG 병합요법이 주로 사용되어 왔다. 그러나 상당 수 환자에서 이식 후 재발이 보고되어1 6 ), 저자 들은 fludarabine 및 A T G를 근간으로 하는 전처 치를 사용하였다. Fludarabine은 n u c l e o t i d e a n a l o g인 9 -β- D - a r a b i n o f u r a n o s y l a d e n i n e의 불 소화 유도체로서 림프구 억제효과가 강하여 알킬화 제에 불응하는 혈액질환의 치료에 사용되어왔으며, 최근에 류마티스 관절염 및 루푸스 등의 자가면역질 환에도 치료효과가 있는 것으로 보고된 바 있다2 3 - 2 5 ). 또한 자가조혈모세포이식을 위한 말초혈액 가동화에 고용량의 C y이 투여되며, 상당 수의 류마티스 관절 염 환자가 이에 반응하여 일시적이지만 뚜렷한 호전 을 나타낸다는 점에 착안하여2 6 ), 저자들은 C y에 대 한 반응 여부에 따라 전처치 요법을 결정하였다. 즉, 환자 2와 3의 경우, 조혈모세포 가동을 위한 C y에 반응하였으므로 fludarabine, ATG에 C y을 병합 하였고, 환자 1의 경우 고용량(총 6 g )의 C y가 투여 되었음에도 불구하고 질환 활성도는 전혀 호전되지 않아 C y에 불응하는 것으로 판단되어, 이식 전처치 로 C y을 제외하고 b u s u l f a n을 병합하였다. Flu- darabine, ATG 및 b u s u l f a n의 병합요법은 m i n i - t r a n s p l a t a t i o n의 전처치로 널리 사용되는 방 법으로, ATG의 T 세포 억제효과와 b u s u l f a n의 골 수계세포(myeloid lineage) 억제효과를 조합할 수 있는 장점이 있다2 7 ). 향후 각 질환에 따른 최적의 시 술법을 정립하기 위한 비교연구가 계속 진행되어야 할 것이다.
고용량 화학요법에 이은 자가조혈모세포 이식 후 류마티스 관절염의 관해 또는 호전이 유도되는 기전 은 불분명하다. 이는 단지 강력한 면역억제의 결과일
수 있으며, 극단적으로 질환을 유발하는 작동세포 (effector cells) 및 기억세포(memory cells)의 완 전한 제거에 의할 가능성도 있다. 반면 병적인 림프 구가 미량 잔존하더라도, 림프구를 중심으로 하는 세 포간 상호작용에 의한 염증 증폭의 악순환을 강한 면 역억제에 의하여 차단함으로써 관용( t o l e r a n c e )이 유도될 수 있는 기회를 제공하고, 주입된 조혈모세포 가 분화됨에 따라 면역성( i m m u n i t y )과 관용 사이 의 균형이 전환되어 면역체계의 근본적인 변화를 유 도할 수도 있다. 이는 이론적으로 clonal exhaus- tion, 비토세포(veto cells), 억제세포( s u p p r e s s e r cells), 그 밖의 자가조절세포들( a u t o r e g u l a t o r y cells), 면역무관심(immune indifference), idio- typic network, 사이토카인 균형의 변화, T 세포 및 B 세포 수용체 r e p e r t o i r e의 변화 등에 의해 일 어날 수 있다2 8 ). 이와 관련되어 조혈모세포이식 후 장기간 지속되는 CD4+ 림프구의 결핍 및 C D 4 : C D 8 비의 역전이 면역체계의 중요한 변화 중 하나로 제시 되고 있다2 3 ). 본 환자들에서도 역시 이식 후에 C D 4 + 림프구가 감소되고 CD4:CD8 비가 역전되어 유지되 는 것이 관찰되었다. CD4+ 림프구의 회복 이후에도 질환 호전상태가 유지되는 지에 대한 장기적인 관찰 및 관해와 재발 전후 다양한 면역학적 변화에 관한 연구가 면역 재구성과 질환 호전과의 인과 관계를 밝 히고 궁극적으로 자가면역질환의 발병 기전을 규명하 는 데에 일조할 것으로 사료된다.
결 론
기존의 치료에 불응하는 류마티스 관절염 환자에서 고용량 면역억제 및 자가조혈모세포이식은 적은 독성 으로 높은 초기 치료 효과를 나타내었다. 향후 치료 반응의 지속성 및 질병 진행 억제 여부를 판정하고, 최적의 시술법을 정립하기 위하여, 보다 많은 환자군 에서의 장기적인 연구가 필요할 것으로 사료된다.
R E F E R E N C E S
11 ) Pincus T, Brooks RH, Callahan LF. Prediction of long-term mortality in patients with rheumatoid arthritis according to simple ques- tionnaire and joint count measures. Ann Intern
Med 1994;120:26-34.
12 ) Maromont AM, Van Bekkum DW. Stem cell transplantation for severe autoimmune dis- eases: new proposals but still unanswered ques- tions. Bone Marrow Transplant 1995;16:497-8.
13 ) Tyndall A, Gratwohl A. Hemopoietic stem and progenitor cells in the treatment of severe autoimmune diseases. Ann Rheum Dis 1996;55:
1 4 9 - 5 1 .
14 ) Van Gelder M, Kinwel-Bohre EP, Van Bekkum DW. Treatment of experimental allergic encephalomyelitis in rats with total body irradiation and syngeneic BMT. Bone Marrow Transplant 1993;11:233-41.
15 ) Knaan-Shanzer S, Houben P, Kinwel-Bohre EPM, Van Bekkum DW. Remission induction of adjuvant arthritis in rats by total body irra- diation and autologous bone marrow transplan- tation. Bone Marrow Transplant 1991;8:333-8.
16 ) Jacobs P, Vincent MD, Mantel RW. Pro- longed remission of severe refractory rheuma- toid arthritis following allogeneic bone marrow transplantation for drug-induced aplastic ane- mia. Bone Marrow Transplant 1996;1:237-9.
17 ) Yin JA, Jowitt SN. Resolution of immune- mediated diseases following allogenic bone mar- row transplantation for leukemia. Bone Marrow Transplant 1992;9:31-3.
18 ) Lowenthal RM, Cohen ML, Atkinson K, Biggs JC. Apparent cure of rheumatoid arthritis by bone marrow transplantation. J Rheumatol 1993;
2 0 : 1 3 7 - 4 0 .
19 ) McAllister LD, Beatty PG, Rose J. Allogeneic bone marrow transplant for chronic myeloge- nous leukemia in a patient with multiple scle- rosis. Bone Marrow Transplant 1997;19:395-7.
1 0 ) Snowden FA, Biggs JC, Brooks PM. Autolo- gous blood stem cell transplantation for autoimmune disease. Lancet 1996;348:1112-3.
1 1 ) Sullivan KM, Furst DE. The evolving role of blood and marrow transplantation for the treat- ment of autoimmune diseases. J Rheumatol 1 9 9 7 ; 2 4 : 1 - 4 .
1 2 ) Tyndall A, Grattwohl A. Blood and marrow stem cell transplants in auto-immune disease:
a consensus report written on behalf of the Europian League against Rheumatism (EULAR) and the Europian Group for Blood and Marrow transplantation (BMT). Bone
Marrow Transplant 1997;19:643-5.
1 3 ) Tyndall A. Autologous hematopoietic stem cell transplantation for severe autoimmune disease with special reference to rheumatoid arthritis.
J Rheumatol. 2001;28(Suppl 64):5-7.
1 4 ) 민도준, 양동원, 민창기, 김완욱, 이상헌, 박성환 등.
불응성 자가면역질환에서의 자가조혈모세포이식. 대한 조혈모세포이식 학회지. 2001;6:1-9.
1 5 ) Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American rheumatism association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988;31:315-24 1 6 ) Burt RK, Georganas C, Schroeder J, Traynor
A, Stefka J, Schuening F, et al. Autologous hematopoietic stem cell transplantaion in refractory rheumatoid arthritis. Arthritis Rheum 1999;42:2281-5.
1 7 ) Felson DT, Anderson JJ, Boers M. American college of rheumatology preliminary definition of improvement in rheumatoid arthritis.
Arthritis Rheum 1995;38:727-35.
1 8 ) Breban M, Dougados M, Picard F, Zompi S, Marolleau JP, Bocaccio C, et al. Intensified dose (4 gm/m2) cyclophosphamide and granu- locyte colony-stimulating factor administration for hematopoietic stem cell mobilization in refractory rheumatoid arthritis. Arthritis Rheum 1999;42:2275-80.
1 9 ) Euler HE, Marmont AM, Bacigalupo A, Fas- tenrath S, Dreger P, Hoffknecht M, et al.
Early recurrence or persistence of autoimmune diseases after unmanipulated autologous stem cell transplantation. Blood 1996;88:3621-5.
2 0 ) Brugger W, Scheding S, Ziegler B, Buhring HJ, Kanz L. Ex vivo manipulation of hematopoietic stem and progenitor cells. Semin Hematol 2000;37(Suppl 2):42-9.
2 1 ) Tyndall A, Fassas A, Passweg J, Ruiz de Elvi- ra, Attal M, Brooks P, et al. Autologous
haematopoietic stem cell transplants for autoimmune disease-feasibility and transplant- related mortality. Bone marrow transplant 1 9 9 9 ; 2 4 : 7 2 9 - 3 4 .
2 2 ) McSweeney PA, Furst DE, West SG. High- dose immunosuppressive therapy for rheuma- toid arthritis: some answers, more questions.
Arthritis Rheum 1999;42:2269-74.
2 3 ) Bhalla KN, Gerson SL, Grant S, Sullivan DM.
Pharmacology and molecular mechanism of action or resistance of antineoplastic agents. In : Hoffman R, Benz EJ Jr., Shattil SJ, Furie B, Cohen HJ, Silberstein LE, McGlave P.
Hematology basic principles and practice, p928, USA, Churchil Livingstone, 2000.
2 4 ) Davis JC, Fessler BJ, Tassiulas IO, McInnes IB, Yarboro CH, et al. High dose versus low dose fludarabine in the treatment of patients with severe refractory rheumatoid arthritis. J Rheumatol 1998;25:1694-704.
2 5 ) Boumpas DT, Tassiulas IO, Fleisher TA, Vaugh- an E, Piscitelli S, Kim Y, et al. A pilot study of low-dose fludarabine in membranous nephropa- thy refractory to therapy. Clin Nephrol 1 9 9 9 ; 5 2 : 6 7 - 7 5 .
2 6 ) Verburg RJ, Kruize AA, van den Hoogen FH, Fibbe WE, Petersen EJ, Preijers F, et al. High- dose chemotherapy and autologous hematopoietic stem cell transplantation in patients with rheumatoid arthritis. Arthritis Rheum 2001;44:
7 5 4 - 6 0 .
2 7 ) 박수정, 민우성, 김희제, 박은정, 엄기성, 민창기 등.
F l u d a r a b i n e을 근간으로 한 저용량 전처치 동종 조 혈모세포 이식. 대한조혈모세포이식학회지 2 0 0 0 ; 5 : 1 - 1 2 .
2 8 ) Burt RK, Brenner M, Burns W, Courier E, Firestein G, Hahn B, et al. Gene-marked autologous hematopoietic stem cell transplanta- tion of autoimmune disease. J Clin Immunol 2 0 0 0 ; 2 0 : 1 - 9 .