pISSN 2234-778X, eISSN 2234-5248 http://dx.doi.org/10.7602/jmis.2013.16.3.34
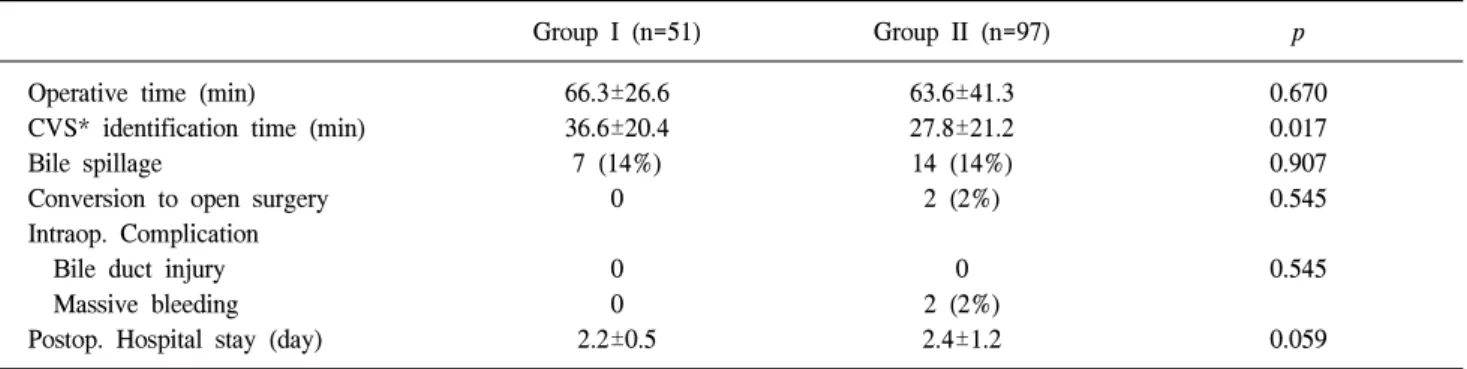
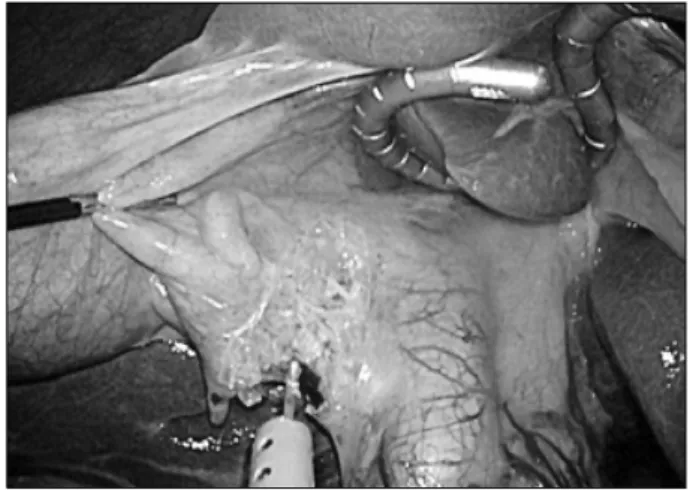
The Effectiveness of a Snake Liver Retractor during Needlescopic Grasper Assisted Sinlge-Incision Laparoscopic Cholecystectomy in the Aspect of Securing a Critical View of Safety
5
0
0
전체 글
(2)
(3)
(4)
(5)
수치

관련 문서
_____ culture appears to be attractive (도시의) to the
It considers the energy use of the different components that are involved in the distribution and viewing of video content: data centres and content delivery networks
After first field tests, we expect electric passenger drones or eVTOL aircraft (short for electric vertical take-off and landing) to start providing commercial mobility
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
The histological course of nonalcoholic fatty liver disease: a longitudinal study of 103 patients with sequential liver biopsies.. McPherson S, Hardy T, Henderson
3) In aspect of occupational attitude, almost half of the students chose their occupation for remuneration in the matter of a woman's holding an occupation
Purpose: The purpose of this study is to report the safety and effectiveness of arthroscopic-assisted implantation of Cartistem®, an articular cartilage
A series of systems for configuring alarm and control functions by monitoring the states of main engine, generator, and auxiliary equipment, for securing the safety
