Original Article
Dosimetric Evaluation of Plans Converted with the DVH-Based Plan Converter
Minsoo Chun* ,†,‡ , Chang Heon Choi* ,†,‡ , Jung-in Kim* ,†,‡ , Jeongmin Yoon* ,†,‡ , Sung Young Lee* ,† , Ohyun Kwon* ,† , Jaeman Son* ,† , Hyun Joon An* ,† , Seong-Hee Kang ΙΙ , Jong Min Park* ,†,‡,§
*Department of Radiation Oncology, Seoul National University Hospital, † Biomedical Research Institute, Seoul National University Hospital, ‡ Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul, § Center for Convergence Research on Robotics, Advanced Institutes of Convergence Technology, Suwon, ΙΙ Department of Radiation Oncology, Seoul National University Bundang Hospital, Seongnam, Korea
Received 28 November 2018 Revised 14 December 2018 Accepted 14 December 2018
Corresponding author Jong Min Park ([email protected]) Tel: 82-2-2072-2527 Fax: 82-2-2072-2527
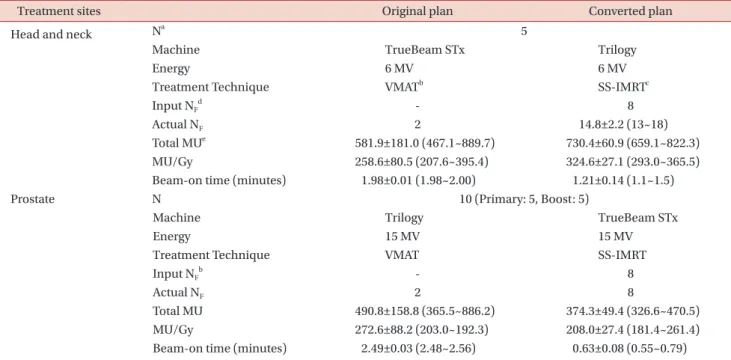
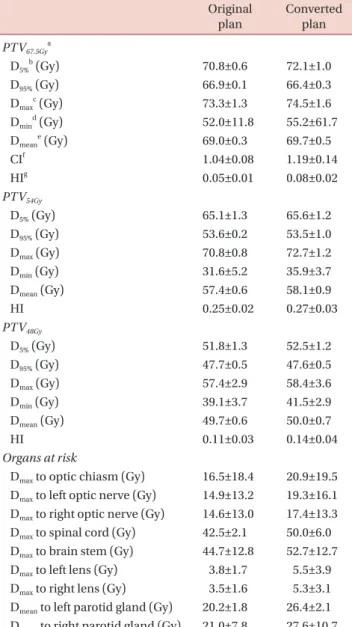
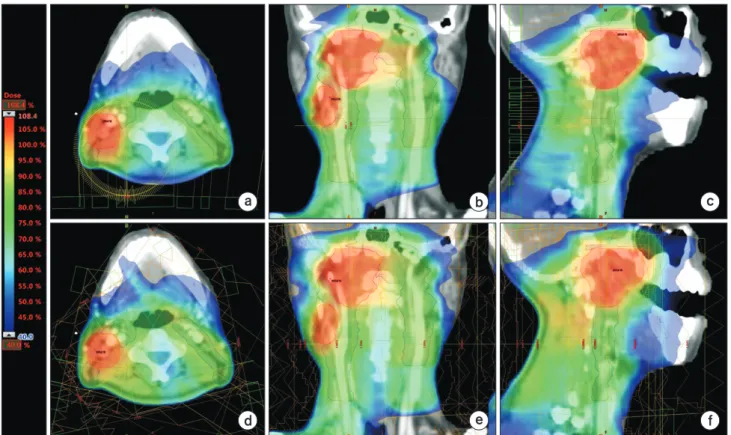
Plans converted using dose-volume-histogram-based plan conversion (DPC) were evaluated by comparing them to the original plans. Changes in the dose volumetric (DV) parameters of five volumetric modulated arc therapy (VMAT) plans for head and neck (HN) cancer and five VMAT plans for prostate cancer were analyzed. For the HN plans, the homogeneity indices (HIs) of the three planning target volumes (PTV) increased by 0.03, 0.02, and 0.03, respectively, after DPC.
The maximum doses to the PTVs increased by 1.20, 1.87, and 0.92 Gy, respectively, after DPC.
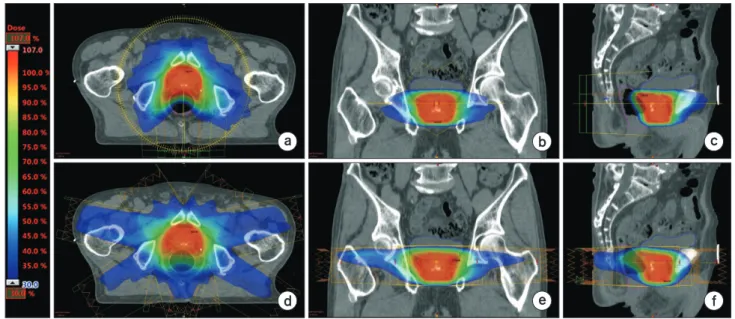
The maximum doses to the optic chiasm, optic nerves, spinal cord, brain stem, lenses, and parotid glands increased after DPC by approximately 4.39, 3.62, 7.55, 7.96, 1.77, and 6.40 Gy, respectively. For the prostate plans after DPC, the HIs for the primary and boost PTVs increased by 0.05 and 0.03, respectively, and the maximum doses to each PTV increased by 1.84 and 0.19 Gy, respectively. After DPC, the mean doses to the rectum and femoral heads increased by approximately 6.19 and 2.79 Gy, respectively, and those to the bladder decreased by 0.20 Gy when summing the primary and boost plans. Because clinically unacceptable changes were sometimes observed after DPC, plans converted by DPC should be carefully reviewed before actual patient treatment.
Keywords: DVH-based plan converter, Volumetric modulated arc therapy, Step-and-shoot IMRT, Dose-volumetric parameters, Plan quality
Copyright © 2018 Korean Society of Medical Physics
CC