882
목 적: 본 연구의 목적은 인공 슬관절 전치환술시 대퇴골 삽입물의 회전 정렬과 관련된 여러 가지 해부학적 지표들의 관계 를 계측하고, posterior condylar axis를 회전 정렬의 척도로 적용할 때 고려해야 할 점을 제시하고자 함이다.
대상 및 방법: 건강한 지원자 40명(남자 20명, 여자 20명)의 40 슬관절을 대상으로 슬관절 신전위(0°)에서의 원위 대퇴골 축상면의 자기 공명 영상에서 임상적 transepicondylar axis (TEA), 외과적 transepicondylar axis, posterior condylar axis (PCA), 대퇴 전-후 축(AP axis)들의 관계를 계측하였으며, 퇴행성 관절염의 모델로 대퇴 후과의 내, 외측 연골의 마모가 다른 경우를 가정하여 PCA와 TEA사이의 각도 변화를 계측하였다.
결 과: 여러 척도 중 임상적 TEA는 AP axis과 수직의 관계를 보였으며 임상적 TEA와 PCA사이의 각도는 평균 5.4°였고 남 자군은 평균 4.3°, 여자군은 평균 6.5°로 여자군에서 통계적으로 유의하게 큰 값을 보였다. 임상적 TEA와 외과적 TEA사이 의 차이는 남자는 평균 3.2°, 여자는 평균 3.8°였다. 대퇴 후과 중 내측의 연골은 모두 마모되고 외측의 연골은 모두 보존 된 상태를 가정하여 계측한 PCA에 의한 회전 정렬은 정상에 비하여 1.9°의 외회전이 추가됨을 알 수 있었다.
결 론: 임상적 TEA와 외과적 TEA는 3° 이상 차이를 보이는 회전 정렬의 척도로서 수술 시 혹은 연구 논문에서 명확히 구 별하여 적용되어야 할 것으로 사료된다. TEA와 PCA사이의 각도는 성별간 유의한 차이를 보이나 이는 추가의 검증이 필 요할 것으로 사료된다. PCA를 이용하여 회전 정렬을 정하는 경우 관절 연골의 마모 정도의 차이에 따라 대퇴 치환물의 회 전의 각도가 변하게 되므로 수술시 이점을 고려를 해야 한다.
색인 단어: 회전 정렬, 대퇴 치환물, 인공 슬관절 전치환술
Purpose: We evaluated the relationship among the various rotational reference axes of femoral compo- nent in TKA, and the potential change in rotational alignment when a posterior condylar axis (PCA) was used as a reference for different cartilage erosions between the medial and lateral posterior femoral con- dyles.
Materials and Methods: The study subjects included twenty male and twenty female volunteers. Axial MR image of the distal femur were used to measure the angles among the clinical transepicondylar axis (cTEA), surgical transepicondylar axis (sTEA), the PCA, and the AP axis. We then evaluated the difference in the amount of rotation between a normal and osteoarthritic model when the PCA was used as a rotation- al reference.
Results: The mean angle between cTEA and PCA was 5.4 degrees, and it was significantly greater in the female (6.5 degrees) than in the male group (4.3 degrees). The cTEA demonstrated a perpendicular rela-
Department of Orthopedic Surgery, Seoul National University College of Medicine, Seoul, Korea
Chong Bum Chang, M.D., Sang Cheol Seong, M.D., Sahnghoon Lee, M.D., Jae Ho Yoo, M.D., Seung Hwan Rhee, M.D., and Myung Chul Lee, M.D.
Anatomical Assessment of Distal Femur for Optimal Femoral Component Rotational Alignment in TKA
882
인공 슬관절 전치환술에서 대퇴 삽입물의 회전 정렬을 위한 원위 대퇴골의 해부학적 계측
장종범ㆍ성상철ㆍ이상훈ㆍ유재호ㆍ이승환ㆍ이명철
서울대학교 의과대학 정형외과학교실
882 882 통신저자 : 이 명 철
서울시 종로구 연건동 28
서울대학교 의과대학 정형외과학교실 TEL: 02-2072-3212∙FAX: 02-2072-2718 E-mail: [email protected]
*본 논문의 요지는 2003년도 대한정형외과학회 춘계학술대회에서 발표되었음.
Address reprint requests to Myung Chul Lee, M.D.
Department of Orthopaedic Surgery, Seoul National University College of Medicine, 28 Yongon-dong, Chongno-gu, Seoul 110-774, Korea
Tel: +82.2-2072-3212, Fax: +82.2-2072-2718 E-mail: [email protected]
성공적인 인공 슬관절 전치환술을 위한 여러 가지 요소 중 대퇴 치환물의 회전 정렬은 인공 슬관절 전치환술 후 대퇴-슬개 관절 운동 역학에 중요한 영향을 미치며, 또 한 굴곡 간격의 형태와 균형에 직접적인 영향을 미치는 요소로 알려져 있어, 적절한 대퇴 치환물의 회전 정렬을 정하는 것은 인공 슬관절 전치환술의 과정 중 매우 중요 한 단계라고 할 수 있다1-6,12,16-24). 대퇴 치환물의 회전 정 렬의 척도는 대퇴 내, 외측 후과를 연결하는 선(posteri- or condylar axis, PCA)과 대퇴 내, 외상과를 연결하는 선(transepicondylar axis, TEA), Whiteside 등이 제 시한 대퇴 전-후 축(anteroposterior axis, AP axis) 등이 알려져 있다4,7,27). 이들 중 TEA는 다시 대퇴 내, 외 상과의 정점을 연결하는 소위 임상적(clinical) TEA와, 대퇴 외상과와 내상과의 고랑(sulcus)을 연결하는 외과 적(surgical) TEA로 구분된다7,10).
여러 연구자들은 대퇴치환물의 회전 정렬을 TEA에 평 행하도록 만드는 것이 대퇴-슬개 관절 역학이나 균형 잡 힌 굴곡 간격을 만드는 가장 적절한 방법임을 제시하고 있으나, 임상적 TEA와 외과적 TEA의 의미에 대하여 이 견이 있으며2,7,8,18,20-22), 둘 사이를 구분하지 않은 많은 연 구들에서‘TEA’의 의미는 저자마다 일관되지 않게 사용 되고 있다8,11,13-15,18,20-22)
. 또한 둘 중 어느 것이 재현성 있는 척도인가에 대하여도 서로 반대되는 의견들이 제시되었
으며7,26,27), 이와 관련된 최근 보고는 임상적 TEA와 외과
적 TEA 모두 관찰자간 혹은 관찰자내 변이가 매우 커서 척도로서의 재현성이 부족함을 시사하였다13,14).
실제로 수술자가 연부조직에 덮여있는 내, 외상과를 직 접 만져서 도시하게 되는 TEA와는 달리, 대부분의 인공 슬관절 전치환술 기기들은 PCA를 이용하여 대퇴 치환물 의 회전 정렬을 정할 수 있는 guide를 제공하고 있으며,
통상 PCA에 대하여 3° 외회전을 하도록 고안되어 있다.
하지만 PCA에 의한 회전 정렬은 퇴행성 관절염에서 대 퇴 후과의 해부학적 변화에 영향을 받게 되는데, 특히 대 퇴 후과의 내, 외측 연골의 마모 정도가 다른 경우는 수술 시 흔히 접하게 되는 경우이며, 이러한 경우 실제로 3° 외 회전이 아닌 다른 각도의 회전 정렬이 만들어 질 수 있음 이 예상된다.
본 연구의 목적은 첫째, 건강한 남, 여 20명의 자기 공 명 영상(magnetic resonance imaging, MRI)을 통 하여 임상적 TEA와 외과적 TEA를 포함한 대퇴 치환물 의 회전 정렬과 연관된 기준선들의 관계를 계측하는 것 과, 둘째, 내, 외측 연골의 마모가 다른 경우를 가정하여 PCA와 TEA 사이의 각도 변화를 계측하고 이를 통하여 PCA를 회전 정렬의 척도로 임상에 적용할 때 적절한 회 전 정렬의 지침을 제시하고자 함이다.
연구 대상 및 방법
이전에 슬관절에 외상이나 감염 등 특별한 병력이 없으 며, 이학적 검사상 슬관절에 특별한 이상이 없는 40명의 건강한 자원자를 대상으로 하였다. 남, 여 각각 20명이 었으며 남자는 평균 22.1세(20-24세), 평균 신장 174 cm (164-184 cm), 평균 체중 68 kg (58-86 kg), 여 자는 평균 25.8세(23-31세), 평균 신장 163 cm (157- 173 cm), 평균 체중 51 kg (42-66 kg)였다. 모든 환자 에서 동일한 방법으로 슬관절 신전상태에서 슬관절용 코 일을 이용하여 대퇴골 원위부의 축상면 영상을 촬영하였 다. 촬영은 1.5tesla 자기 공명 영상 장치(Symphony�, Siemens AG, Munich, Germany)를 이용하여 T1강 조 영상(repetition time msec/echo time msec, 750/
20)으로 시행하였으며, 보다 정밀한 계측을 위하여 고해 tionship with the AP axis in both groups. The average angles between cTEA and sTEA were 3.2 degrees in the male group and 3.8 degrees in the female group. When we assumed complete erosion of the carti- lage on the medial posterior condyle with preservation on the lateral side, the angles between the cTEA and PCA decreased by an average of 1.9 degrees in both groups.
Conclusion: This study suggests that the two transepicondylar axes, which demonstrated greater than 3 degrees in angle-difference, should be defined clearly in scientific reports and in their application as rota- tional references in TKA. Some significant gender differences in the rotational profile were noted. When the PCA is used as a rotational reference, potential errors caused by the different amounts of cartilage ero- sion between the medial and lateral posterior condyles should be considered.
Key Words: Rotational alignment, Femoral component, Total knee arthroplasty
상도(512*256-512*512 픽셀)와 얇은 절편(2 mm)으로 촬영하였다. 계측은 의료영상 저장 전송 시스템(picture achieving and communication system, PACS)상 의 프로그램인 M-view (Marotech�, Seoul, Korea) 를 이용하여, 판독용 21인치 모니터에서 시행하였다.
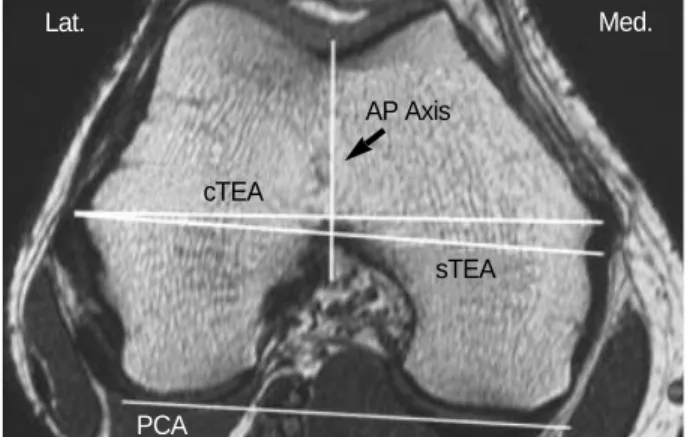
슬관절 신전에서의 축상면 MR 영상에서 외과적 및 임 상적 TEA와 PCA 사이의 각도, AP axis과 외과적 및 임 상적 TEA사이의 각도를 계측하였다. 임상적 TEA는 MR 영상에서 대퇴골 내상과와 외상과의 정점을 연결하는 선 으로, 외과적 TEA는 외상과의 정점과 내상과의 고랑을 연 결하는 선으로, AP axis은 슬개골 고랑(patellar groo-
ve)의 가장 깊은 점과 대퇴과간 절흔(intercondylar no- tch)의 정점을 잇는 선으로, PCA는 양측 대퇴후과의 관 절 연골의 정점을 잇는 선으로 각각 계측하였다(Fig. 1).
대다수의 퇴행성 관절염 환자들이 내측 연골의 마모가 외측에 비하여 심한 내반 변형을 보이므로, 이러한 상황 의 재현 모델로서 대퇴 후과 내측의 연골은 모두 닳아 없 어지고 외측의 연골은 모두 보존된 상태를 가정하여 임상 적 TEA와 PCA 사이의 각도를 계측하였고, 연골의 마모 정도와 각도의 변화 사이의 관계를 계산하였다(Fig. 2).
모든 측정을 시행할 때 기준선의 각 정점들이 하나의 이미지에 존재하지 않는 경우가 대부분이므로 각각의 적 합한 이미지에서 정점들을 표시한 후 한 화면에 모아 측 정을 시행하였다. 저자들은 이러한 각각의 정점을 투시 하는 방법이 정확하고 재현성 있는 계측을 시행하는데 매우 중요한 요소라고 생각하며, 그 이유는 슬관절의 회 전 정렬의 결과 값들은 몇도의 오차에도 결과해석에 큰 영향을 미칠 수 있기 때문이다.
측정은 저자 중 한 명에 의하여 모두 시행되었고, 측정 의 관찰자내 신뢰성(intraobserver reliability) 검사를 위하여 1주 이상의 간격으로 총 3회 측정하였으며, 3회 측정 값의 평균치를 참 값(true value)으로 정의 하였다.
측정의 관찰자내 신뢰성 평가는 intraclass correlation coefficient (ICC)를 이용하였다. ICC는 0에서 1사이 의 값을 가지며, 일반적으로 0.75 이상인 경우, 측정값 간의 좋은 일치도(good agreement)를 의미하며 0.40 이하인 경우 나쁜 일치도(poor agreement)를 의미한다.
남녀 간의 차이에 대한 통계처리는 SPSS (version Fig. 1.An MRI scan demonstrates a transverse view of the distal
femoral condyle. cTEA: clinical transepicondylar axis-a line con- necting the medial and lateral epicondylar prominences. sTEA:
surgical transepicondylar axis-a line connecting the sulcus of the medial epicondyle and lateral epicondylar prominences. PCA:
posterior condylar axis-a line connecting the posterior aspects of the femoral condyles. AP axis: a line through the deepest part of the patellar groove anteriorly and the center of the intercondy- lar notch.
Lat. Med.
AP Axis
PCA cTEA
sTEA
A B
Fig. 2.The change of rotational alignment related to the amount of cartilage erosion. (A) PCA was drawn assuming the preservation of cartilage of the lateral and medial (arrow heads) condyles. (B) PCA was drawn assuming the complete erosion of the medial side cartilage (arrow heads) with a preserved lateral side.
cTEA
PCA
cTEA
PCA
10.7; SPSS, Chicago, IL)을 이용하여 Mann-Whit- ney test를 통하여 시행하였다.
결 과
1.임상적 및 외과적TEA와PCA임상적 TEA와 PCA 사이의 각도는 평균 5.4°였으며 남 자군은 평균 4.3° (2.3-6.2°, SD: 1.2), 여자군은 평균 6.5° (4.3-8.8°, SD: 1.3)로 여자군에서 통계적으로 유 의하게 큰 값을 보였다(p<0.001). 외과적 TEA와 PCA 사이의 각도는 평균 1.8°였으며 남자군은 평균 1.1° (-0.9
~2.8°, SD: 1.1), 여자군은 평균 2.7° (0.4-4.8°, SD:
1.2)로 역시 여자군에서 통계적으로 유의하게 큰 값을 보 였다(p<0.001). 임상적 TEA와 외과적 TEA 사이의 각 도는 비교적 일정한 값을 보였으며 남자는 평균 3.2° (2.5 -3.8°, SD: 0.4), 여자는 평균 3.8° (3.0-4.5°, SD 0.4) 였고 이를 내상과 부위에서의 거리로 환산해보면 남자는 평균 5 mm, 여자는 평균 4.9 mm로 결국 임상적 TEA 와 외과적 TEA의 차이를 결정하는 내상과의 정점에서 고 랑 사이의 간격은 약 5 mm 임을 알 수 있었다(Table 1).
2.임상적 및 외과적TEA와AP
axis
임상적 TEA와 AP axis 사이의 각도는 남자의 경우 평 균 90.0° (84.9-94.1°, SD 2.4), 여자의 경우 평균 90.5°
(86.1-93.4°, SD 2.0)였으며 외과적 TEA와 AP axis 사이의 각도는 남자는 평균 93.2° (88.4-97.0°, SD 2.2), 여자는 평균 94.1° (89.7-98.1°, SD 2.1)로 남녀 간의 유의한 차이는 없었다. AP axis과 임상적 TEA와는 비 교적 직각에 가까운 각도를 보여 AP axis에 수직으로 회전을 시키면 임상적 TEA에 평행하도록 되며, 외과적 TEA에 비하여 더 외회전되는 결과가 된다(Table 2).
3.연골의 마모 정도에 따른PCA와TEA사이의 각도 변화
퇴행성 관절염의 하나의 모델로서 내측의 연골은 모두 닳아 없어지고 외과의 연골은 모두 보존된 상태를 가정하 여 계측한 임상적 TEA와 PCA사이의 각도는 남자군은 평균 2.4°, 여자군은 평균 4.6°로 남녀 모두 각각 1.9°가 감소하였다. MR영상에서 계측된 내측 대퇴 후과의 연골 의 평균 두께는 남자 1.8 mm, 여자 1.6 mm로 연골의 마모 정도에 따른 각도의 변화를 계산해보면 대퇴 후과 의 내측의 연골이 외측 연골에 비하여 1 mm 더 닳았을 경우 TEA와 PCA사이의 각도는 남자가 약 1.1°, 여자가 약 1.2°의 감소가 발생하여 결국 양측 대퇴후과의 연골의 정점을 연결하는 PCA를 척도로 삼아 회전 정렬을 정하 는 기기에서는 연골 두께 1 mm당 약 1°의 회전정렬의 변 화가 생기게 됨을 알 수 있었다.
고 찰
현재까지의 많은 연구에서 대퇴 치환물의 회전을 TEA 에 평행하게 만드는 것이 가장 적합하다고 보고하고 있지
만2,8,18,20-22), 저자들에 따라 임상적 TEA와 외과적 TEA의
유용성에는 이견이 있다1,7,15,25,26,28). 임상적 TEA와 외과 적 TEA 중 어느 것이 슬관절의 기능적 축인가에 대하여, Hollister 등11)이 사체의 슬관절을 이용한 연구에서 슬관 절의 굴곡-신전은 하나의 축을 중심으로 이루어지며, 그 축은 내측 측부인대의 기시부와 외측 측부인대의 기시부 를 연결하는 선, 즉 외과적 TEA라고 기술하였으나, Chu- rchill 등8)은 유사한 연구에서 임상적 TEA가 굴곡-신 전의 축과 근접해있음을 보고하여 대퇴 치환물을 임상적 TEA에 평행하도록 회전시키는 것이 생역학적으로 유리 함을 시사하였다. 또한 Akagi 등2)은 퇴행성관절염 환자 를 대상으로 시행한 연구에서 임상적 TEA가 원위 대퇴 부의 전-후 축 즉, AP axis과 수직인 관계를 이루고 있 어 대퇴-슬개 관절의 기능적 축에 가까울 것임을 시사하
Male
Reference axes Female ICC p
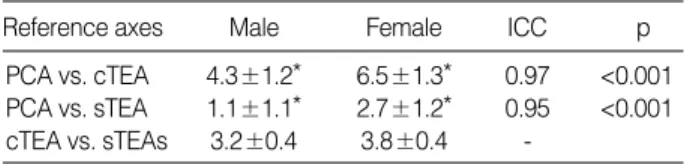
PCA vs. cTEA 4.3±1.2* 6.5±1.3* 0.97 <0.001 PCA vs. sTEA 1.1±1.1* 2.7±1.2* 0.95 <0.001 cTEA vs. sTEAs 3.2±0.4 3.8±0.4 -
Table 1.The angles among the clinical TEA, surgical TEA, and PCA (Mean±SD, Degrees) and reliability for the angles (Intraclass Correlation Coefficient=ICC)
PCA, posterior condylar axis; cTEA, clinical transepicondylar axis; sTEA, surgical transepicondylar axis.
*Denotes significant difference between the two groups (p<0.001)
Male
Reference axes Female ICC p
AP axis vs. cTEA 90.0±2.4 90.5±2.0 0.93 0.401 AP axis vs. sTEA 93.2±2.2 94.1±2.1 0.92 0.137 Table 2.The angles among the clinical TEA, surgical TEA and AP axis (Mean±SD, Degrees) and reliability for the an- gles (Intraclass Correlation Coefficient=ICC)
AP axis, anteroposterior axis of the femur; cTEA, clinical transepicondylar axis; sTEA, surgical transepicondylar axis.
였으며, 외과적 TEA의 경우 내상과의 고랑이 소실된 경 우가 25% 이상이어서 척도로서의 재현성이 떨어진다고 기술하였다.
어느 축이 굴곡 간격을 가장 적합하게 만드는 가에 대 한 연구 역시 이견이 있는데, Olcott와 Scott21)은 인공 슬관절 전치환술을 시행한 환자를 대상으로 한 수술장 측 정에서 TEA (아마도 외과적 TEA)에 평행하게 회전정렬 을 맞추는 것이 균형 잡힌 굴곡 간극을 가장 잘 재현한다 고 하였지만, Matsuda 등16)은 MRI를 이용한 연구에서 경골의 역학적 축의 수직선과 비교하여 보면 외과적 TEA 보다는 임상적 TEA가 평행한 관계를 보여 임상적 TEA 가 균형 잡힌 굴곡 간격을 만드는데 유리하다고 하였다.
하지만 많은 회전 정렬에 관한 연구들에서 TEA는 구별 하여 기술되지 않았으며8,11,13-15,18,20-22)
, 저자들마다‘TEA’
를 외과적 TEA로 제시하는 경우와 임상적 TEA로 제시 하는 경우들이 혼재되어 있다. 본 연구 결과에서 제시한 대로 임상적 TEA와 외과적 TEA는 3° 이상의 차이를 보 이는 축이어서 반드시 그 의미가 구별되어야 될 것으로 사료되며, 본 연구의 결과만으로는 임상적 TEA와 외과
적 TEA중 어느 것이 더 바람직한 척도인지 제시하기는 어 려우나 남, 여 두 그룹 모두에서 임상적 TEA가 AP axis 와 수직인 관계를 보여 임상적 TEA가 대퇴-슬개 관절의 기능적 축으로서는 좀더 유리할 가능성을 시사하였다2).
임상적 TEA와 외과적 TEA의 척도로서의 재현성에 대하여 Berger 등7)은 내상과의 고랑(sulcus)이 명확하 고 재현성 있게 확인되는 구조물이며, 이곳과 외상과의 정점을 연결하는 외과적 TEA가 대퇴 치환물의 회전 정 렬의 지침으로 유용한 척도임을 처음으로 기술하였지만, 다른 저자들은 덮여 있는 연부조직 때문에 수술장에서 내 상과의 고랑의 위치를 잡는 것이 매우 어렵고, 또한 퇴행 성 관절염 환자에서 내상과의 고랑이 소실되어 명확히 구 분되지 않는 경우가 있어 외상과의 정점과 내상과의 정점 의 연결선인 임상적 TEA가 더 유용한 척도라고 기술하
였다26,28). 하지만 최근 보고에서는 실제 수술장에서 외과
적 TEA를 도시함에 있어 관찰자간 변이(inter-observer variation)가 최대 23°의 차이를 보여 재현성이 매우 떨 어짐이 보고된 바 있으며14), 임상적 TEA에 대하여도 관 찰자간 변이가 평균 9° (최대 15°), 관찰자내 변이(intra-
A B
Fig. 3.Femoral component rotational guide (A) and its applica- tion (B). The two bars of the guide were rested on the medial and lateral posterior condyles to establish the rotational angle.
(C) The reference line (arrows) was drawn assuming preserva- tion of the cartilage of the lateral and medial (arrow head) con- dyles using the femoral component rotational guide. (D) Anoth- er reference line (white arrows) was drawn assuming preserva- tion of the cartilage of the lateral condyle and erosion of the me- dial (arrow head) condylar cartilage (thickness of 2 mm) using the femoral component rotational guide. The difference in the angle between the two lines was 2.4 degrees.
C
D
observer variation) 역시 평균 5° (최대 15°) 이상 차이 가 나서 TEA의 유용성에 의구심을 제시한 바 있다13).
반면 PCA는 수술시 명확히 구분되는 척도로서 실제로 많은 인공 슬관절 전치환 기기들에 PCA guide가 포함되 어 있고, 이에 대하여 3° 외회전 시키는 것을 대퇴 치환물 의 회전 정렬의 기준으로 삼도록 고안되어 있다. 하지만 PCA를 기준으로 한 회전 정렬은 대퇴 후과의 개인별 해 부학적 변이와 퇴행성 관절염에 의한 해부학적 변화들에 의하여 영향을 받을 수 있다는 것이 문제점으로 알려져
있다21,27). AP axis도 수술시 연부조직의 방해 없이 도시
할 수 있으며, 특히 외반 변형이 동반된 퇴행성 관절염의 슬관절에서 유용한 척도로 보고되었으나27), 이 역시 슬개 골 고랑(patellar groove)의 이형성(dysplasia)이 있는 경우나 대퇴과간 절흔(intercondylar notch)의 퇴행성 변화로 인한 변형 등에 의해 영향을 받을 수 있는 것으로 알려져 있다22).
본 연구의 경우 TEA와 PCA사이의 각도는 남, 여 각 각 최대 약 4° 및 4.5°의 개인별 편차를 보인 반면, TEA 와 AP axis는 이보다 큰 최대 약 9°의 편차를 보여, PCA 가 AP axis에 비하여 좀더 재현성 있는 척도 임을 시사 하였지만, 이는 정상인에서의 결과이며 퇴행성 슬관절염 환자의 경우에 대하여는 추가의 연구가 뒷받침되어야 할 것이다. 한 가지 주목할 만한 결과는 남, 여의 TEA와 PCA사이의 각도가 유의한 차이를 보여준다는 것이며, 이는 PCA를 회전 정렬의 척도로서 사용시 성별에 따라 다른 값을 적용해야 함을 시사한다. 그러나 본 연구와 유 사하게 여성군의 PCA와 TEA사이의 각도가 남성군에 비 하여 유의하게 큰 값을 보고한 연구들도 있고7,15), 유의한 차이가 없는 보고도 있으며9,22), 본 연구가 남, 여 각각 20 명만을 대상으로 한 연구여서 성별에 대한 회전 정렬의 해 부학적 차이는 추가의 검증이 필요할 것으로 사료되었다.
퇴행성 관절염에 의한 해부학적 변화에 의한 영향에 대 하여 고려해야 할 사항들 중 하나는 양측 대퇴 후과의 연 골의 마모 정도가 다를 때, PCA를 회전 정렬의 기준으로 삼을 경우 원하는 각도와 다른 회전이 만들어 질 가능성 이 있다는 점이다. 특히 수술시 대퇴 후과의 양측 연골 면 을 기준으로 삼아 외회전을 하도록 고안되어 있는 PCA guide의 경우 guide의 bar가 닿는 부위의 연골 면의 마 모 상태가 현저하게 차이를 보이면 정해진 회전 각도와 는 차이가 나는 회전 정렬이 이루어 질 수 있는데, 본 연
구 결과에서처럼 내측 후과의 연골이 모두 마모되고 외측 연골은 보존되어 있는 경우를 가정하면 guide에 정해져 있는 회전보다 약 2° 정도의 외회전이 추가되기 때문에 3° 외회전만을 시켜도 5°의 외회전이 일어날 수 있으며, 반대의 경우에는 3°의 외회전을 시켜도 약 1°만의 외회전 이 만들어 질 것으로 예측된다(Fig. 3). 따라서 대퇴 후 과 양측 연골 면의 마모 상태가 현저하게 차이를 보일 경 우 이러한 면을 고려하여 적절한 회전정렬을 정해야 할 것으로 사료된다.
결 론
임상적 TEA와 외과적 TEA는 3° 이상 차이를 보이는 회전 정렬의 척도로서 수술시 혹은 연구 논문에서 명확히 구별하여 적용되어야 할 것으로 사료된다. TEA와 PCA 사이의 각도는 성별간 유의한 차이를 보이나 이는 추가의 검증이 필요할 것으로 사료된다. PCA를 척도로 하는 경 우 대퇴 후과 관절 연골의 마모 정도의 차이에 따라 대퇴 치환물의 회전의 각도가 변하게 되므로 수술시 이점을 고 려를 해야 한다.
참고문헌
1. Akagi M, Matsusue Y, Mata T, et al: Effect of rotational align- ment on patellar tracking in total knee arthroplasty. Clin Orthop Relat Res, 366: 155-163, 1999.
2. Akagi M, Yamashita E, Nakagawa T, Asano T and Naka- mura T:Relationship between frontal knee alignment and refer- ence axes in the distal femur. Clin Orthop Relat Res, 388: 147-156, 2001.
3. Anouchi YS, Whiteside LA, Kaiser AD and Milliano MT:
The effects of axial rotational alignment of the femoral component on knee stability and patellar tracking in total knee arthroplasty demon- strated on autopsy specimens. Clin Orthop Relat Res, 287: 170- 177, 1993.
4. Arima J, Whiteside LA, McCarthy DS and White SE: Fe- moral rotational alignment, based on the anteroposterior axis, in total knee arthroplasty in a valgus knee. A technical note. J Bone Joint Surg, 77-A: 1331-1334, 1995.
5. Barrack RL, Schrader T, Bertot AJ, Wolfe MW and Myers L:
Component rotation and anterior knee pain after total knee arthro- plasty. Clin Orthop Relat Res, 392: 46-55, 2001.
6. Berger RA, Crossett LS, Jacobs JJ and Rubash HE: Malro- tation causing patellofemoral complications after total knee arthro- plasty. Clin Orthop Relat Res, 356: 144-153, 1998.
7. Berger RA, Rubash HE, Seel MJ, Thompson WH and Cros- sett LS:Determining the rotational alignment of the femoral com- ponent in total knee arthroplasty using the epicondylar axis. Clin Orthop Relat Res, 286: 40-47, 1993.
8. Churchill DL, Incavo SJ, Johnson CC and Beynnon BD: The transcondylar axis approximates the optimal flexion axis of the knee.
Clin Orthop Relat Res, 356: 111-117, 1998.
9. Griffin FM, Insall JN and Scuderi GR: The posterior condylar angle in osteoarthritic knees. J Arthroplasty, 13: 812-815, 1998.
10. Griffin FM, Math K, Scuderi GR, Insall JN and Poilvache PL:Anatomy of the epicondyles of the distal femur: MRI analysis of normal knees. J Arthroplasty, 15: 354-359, 2000.
11. Hollister AM, Jatana S, Singh AK, Sullivan WW and Lu- pichuk AG: The axes of rotation of the knee. Clin Orthop Relat Res, 290: 259-268, 1993.
12. Insall JN, Scuderi GR, Komistek RD, Math K, Dennis DA and Anderson DT:Correlation between condylar lift-off and femoral component alignment. Clin Orthop Relat Res, 403: 143- 152, 2002.
13. Jenny JY and Boeri C: Low reproducibility of the intra-operative measurement of the transepicondylar axis during total knee replace- ment. Acta Orthop Scand, 75: 74-77, 2004.
14 Jerosch J, Peuker E, Philipps B and Filler T: Interindividual reproducibility in perioperative rotational alignment of femoral com- ponents in knee prosthetic surgery using the transepicondylar axis.
Knee Surg Sports Traumatol Arthrosc, 10: 194-197, 2002.
15. Mantas JP, Bloebaum RD, Skedros JG and Hofmann AA:
Implications of reference axes used for rotational alignment of the femoral component in primary and revision knee arthroplasty. J Arthroplasty, 7: 531-535, 1992.
16. Matsuda S, Miura H, Nagamine R, Urabe K, Mawatari T and Iwamoto Y:A comparison of rotational landmarks in the distal femur and the tibial shaft. Clin Orthop Relat Res, 414: 183- 188, 2003.
17. Matsuda S, Matsuda H, Miyagi T, Sasaki K, Iwamoto Y and Miura H:Femoral condyle geometry in the normal and varus knee.
Clin Orthop Relat Res, 349: 183-189, 1998.
18. Miller MC, Berger R, Petrella AJ and Rubash HE: Optimiz- ing Femoral Component Rotation in total knee arthroplasty. Clin Orthop Relat Res, 392: 38-45, 2001.
19. Nagamine R, Miura H, Inoue Y, et al: Reliability of the antero- posterior axis and the posterior condylar axis for determining rota- tional alignment of the femoral component in total knee arthroplas- ty. J Orthop Sci, 3: 194-198, 1998.
20. Olcott CW and Scott RD: Femoral component rotation during total knee arthroplasty. Clin Orthop Relat Res, 367: 39-42, 1999.
21 Olcott CW and Scott RD: A comparison of 4 intraoperative me- thods to determine femoral component rotation during total knee arthroplasty. J Arthroplasty, 15: 22-26, 2000.
22. Poilvache PL, Insall JN, Scuderi GR and Font-Rodriguez DE:Rotational landmarks and sizing of the distal femur in total knee arthroplasty using the epicondylar axis. Clin Orthop Relat Res, 331: 35-46, 1996.
23. Rhoads DD, Noble PC, Reuben JD, Mahoney OM and Tul- los HS:The effect of femoral component position on patellar tracking after total knee arthroplasty. Clin Orthop Relat Res, 260: 43-51, 1990.
24. Singerman R, Pagan HD, Peyser AB and Goldberg VM:
Effect of femoral component rotation and patellar design on patel- lar forces. Clin Orthop Relat Res, 334: 345-353, 1997.
25. Tanavalee A, Yuktanandana P and Ngarmukos C: Surgical epicondylar axis vs anatomical epicondylar axis for rotational align- ment of the femoral component in total knee arthroplasty. J Med Assoc Thai, 84 (Suppl): S401-408, 2001.
26. Uehara K, Kadoya Y, Kobayashi A, Ohashi H and Yamano Y:Bone anatomy and rotational alignment in total knee arthroplas- ty. Clin Orthop Relat Res, 402: 196-201, 2002.
27 Whiteside LA and Arima J: Anteroposterior axis of femoral rota- tional alignment in a valgus total knee arthroplasty. Clin Orthop Relat Res, 321: 168-172, 1995.
28. Yoshino N, Takai S, Ohtsuki Y and Hirasawa Y: Computed tomography measurement of the surgical and clinical transepicondy- lar axis of the distal femur in osteoarthritic knees. J Arthroplasty, 16: 493-497, 2001.