DOI : 10.3341/jkos.2009.50.4.510
= 증례보고 =
접수번호 : 09-16라섹수술 후 각막 및 앞방의 변화: Pentacam 분석
박진형
1⋅강자헌
2⋅진경현
1경희대학교 의과대학 안과학교실1, 경희대학교 동서신의학병원2
목적: 술 후 잠재성 각막확장증 여부를 알기 위해서 Pentacam을 이용하여 라섹(LASEK) 수술 전후의 각막 및 앞방의 변화를 알아보고자 하였다.
대상과 방법: 36명 71안을 대상으로 라섹수술을 시행하였다. 수술 전 및 수술 후 1개월째에 Pentacam (Oculus, Germany)을 이용하여 각막 앞, 뒷면의 비구면도(Q-value) 및 전위도, 중심각막두께, 앞방 깊이, 앞방 부피를 측정하였다.
결과: 수술 전후 각막 뒷면의 비구면도 및 전위도는 유의한 차이를 보이지 않았다(p=0.668, p=0.101). 수술 후 앞방 깊이, 앞방각 및 부피는 각각 0.088 mm, 0.983°, 7.21 mm3 감소하였다(p=0.000). 수술 전후 중심각막두께, 각막 앞면의 비구면도 및 전위도는 유의한 차이를 보였다(p=0.000).
결론: Pentacam을 이용하여 라섹수술 전후 전방 및 각막의 변화를 비교한 결과, 1개월 째 각막 앞면은 유의한 변화를 보이는 반면, 각막 뒷면은 유의한 변화를 보이지 않았고, 앞방 깊이, 앞방 각 및 부피가 감소하는 변화를 보였지만 장기간 경과 관찰이 필요할 것으로 생각된다.
<대한안과학회지 2009;50(4):510-517>
■ 접 수 일: 2008년 9월 18일 ■ 심사통과일: 2008년 12월 3일
■ 통 신 저 자: 진 경 현
서울시 동대문구 회기동 1 경희대학교병원 안과
Tel: 02-958-8451, Fax: 02-966-7340 E-mail: [email protected]
* 본 논문의 요지는 2008년 대한안과학회 제99회 춘계학술대회에서 포스터로 발표되었음.
LASEK (Laser subepithelial keratomileusis: LASEK) 은 LASIK (Laser in situ keratomileusis: LASIK)에서 나 타날 수 있는 각막절편 유리, 각막절삭기의 불완전한 통과, 각막절편의 주름, 각막확장증 등의 합병증과 PRK 후에 나 타날 수 있는 통증, 유루, 시력회복 지연을 줄일 수 있어 널 리 사용되고 있다.1 굴절교정수술이 흔하게 시행되어짐에 따라 굴절교정수술 후 각막 형태 변화에 대하여 많은 연구 가 이루어지고 있다.2
Pentacam은 비침습적으로 앞방각, 앞방깊이, 앞방부피를 측정할 수 있는 검사기구로 앞방척도를 측정하는데 있어서 높은 신뢰도를 가지며,3A-scan 초음파,4AC-Master (Carl Zeiss Meditech, Jena, Germany),5IOL Master (Carl Zeiss Meditech, Jena, Germany)6와 유사한 측정치를 보인다. 그 러나 Elbaz et al7은 Pentacam은 앞방깊이 측정에 있어 A-scan 초음파와 IOL master와 다른 측정결과를 보여 호환이 불가능하다고 하였다. 하지만 Shanker et al8은 Pentacam은 앞방측정에 있어서 높은 신뢰도와 더불어 뛰어난 재현성을 보인다고 하였다.
Pentacam은 각막 뒷면 측정에 있어 높은 재현성을 보여,9 각막 뒷면의 상승을 평가하여 원추각막, 잠재성 원추각막을 정상 각막과 감별하는데 유용하며, 이는 LASIK 수술 후 각 막확장증 예방에 도움이 된다.10,11 또한, Emre et al12은 Pentacam을 이용한 측정결과 원추 각막이 진행함에 따라 가장 얇은 각막두께가 얇아지고, 각막부피가 작아지며, 앞방척도들이 작아지는 변화를 보인다고 하였다.
굴절교정수술 후 각막 및 앞방의 변화에 대한 이전의 연구 에서 LASIK 수술 후 각막의 비구면도가 증가하며,13Ciolino et al14은 Pentacam을 이용하여 LASIK 수술 후 단기, 장기간 추적 결과 각막 뒷면의 유의한 전방 전위는 보이지 않으며, 이 결과는 이전의 Orbscan을 이용한 결과와는 다른 양상을 보인다고 하였다.
Hashemi and Mehravaran15은 굴절교정수술 후 각막 뒷면 의 전위 정도 평가에 있어 Orbscan과 Pentacam의 결과가 다 르며, Orbscan의 결과가 다소 과장된 결과를 보인다고 하였 다. 또한, 앞방깊이 측정에 있어 두 검사 결과에 차이를 보인 다고 하였다.
LASEK 수술 등의 굴절교정수술 후 추적 관찰 시 Placido- disc 각막 지형도, Orbscan, Pentacam, 고속 전안부 빛간섭 단층촬영계 등을 이용하여 술 후 각막확장증 유무, 각막절 삭면의 위치 등을 관찰하게 된다. 또한, 굴절교정수술 후 각 막 앞뒤면의 변화 및 안압의 변화에 관해서는 많은 연구가 있지만, 앞방의 변화에 관한 연구는 흔하지 않다. 본 연구에 서는 근시안에서 가장 흔하게 사용되고 있는 LASEK 수술을
Preoperative ashpericity (Q-value)
-1.20 -0.80 -0.40 0.00 0.40 0.80 1.20 1.60 2.00 2.40 2.80 3.20 3.2
2.6
2.4
2.0
1.6
1.2
0.8
0.4
0.0
-0.4
-0.8
-1.2
A
Preoperative ashpericity (Q-value)
-0.40 -0.20 0.00 0.20 0.40 0.60 0.80 1.00 1.00
0.80
0.60
0.40
0.20
0.00
-0.20
-0.40 B
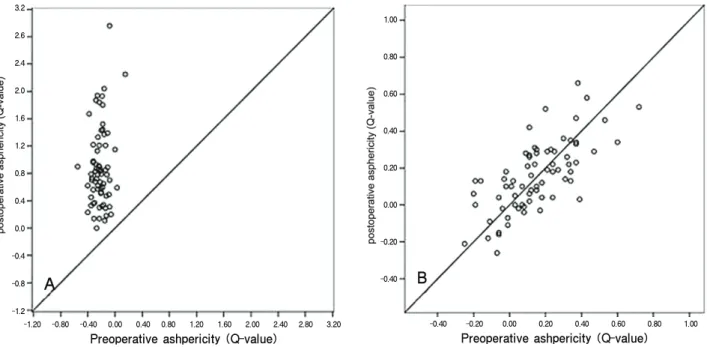
Figure 1. The scatterplots for corneal asphericity between preoperative and postoperative states (at 1 month after operation). (A) Anterior corneal surface. A prolate anterior corneal surface had changed into an oblate surface after operation. (B) Posterior corneal surface. An asphericity of the posterior cornea was unchanged after operation.
Preoperative-Q* Postoperative-Q†
Mean±SD‡(range) Mean±SD (range) p-value
Anterior corneal surface -0.2196±0.1084 (-0.55 to 0.15) 0.8800±0.5770 (0.00 to 3.00) 0.000 Posterior corneal surface 0.1493±0.1951 (-0.25 to 0.72) 0.1569±0.1896 (-0.26 to 0.66) 0.668
*Preoperative-Q=Preoperative asphericity (Q-value); †Postoperative-Q=Postoperative asphericity (Q-value) (at l month after operation); ‡SD=Standard deviation.
Table 1. The comparison of anterior and posterior corneal asphericity (Q-value) between preoperative and post- operative state (at 1 month after operation)
받은 환자를 대상으로 하여 Pentacam으로 측정한 LASEK 수술 전 후의 각막 및 앞방의 변화를 알아보고자 하였다.
대상과 방법
대상
2007년 7월부터 2008년 4월까지 본원 안과에서 LASEK 수술을 받은 근시 외에 안과적 이상이 없는 환자들 36명 71안을 대상으로 하였다.
술 전 검사
술 전에 안압, 나안시력, 세극등현미경검사, 조절마비제 점안 후 타각적굴절검사, 초음파각막두께측정계 검사(DGH
500BPL, DGH Technology, Inc., Pennsylvania, USA), Scheimpflug 영상 검사(Pentacam, Oculus Inc., Dutenhofen, Germany)를 시행하였다.
수술방법
증류수로 희석시킨 20% 알코올과 epithelial micro-hoe 를 이용하여 각막상피를 부드럽게 벗겨낸 후 엑시머레이저 (Mel 70 G-scan, Asclepion Meditec, Germany) 조사하 였다. 각막기질을 평형염류용액으로 충분히 세척하고 관류 용주사바늘(irrigation needle)을 이용하여 조심스럽게 원 위치시키고 치료용 콘택트렌즈를 덮었다.
수술 직후 0.5% moxifloxacin (Vigamox®, Alcon, USA) 과, 0.01% fluorometholone (오큐메토론®, 삼일제약)을 한 방울씩 점안하였고 술 후 1주일간 각막상피의 재생이 끝날
Preoperative thickness Postoperative thickness
Mean±SD†(range) Mean±SD (range) p-value
CCT* (μm) 545.73±30.35 (485 to 618) 459.90±41.18 (381 to 549) 0.000
*CCT=central corneal thickness; †SD=standard deviation.
Table 2.The comparison of central corneal thickness between preoperative and postoperative state (at 1 month after operation) (Pentacam parameter)
때까지 0.5% moxifloxacin (Vigamox®, Alcon, USA)과 0.01% fluorometholone(오큐메토론®, 삼일제약)을 6시간마 다 점안하였으며 그 후 2주간은 0.01% fluorometholone(오 큐메토론®, 삼일제약)을 12시간마다 점안하였다. 이후 각막 혼탁 정도에 따라 0.01% fluorometholone 점안 횟수를 조절 하였다.
술 후 검사
술 후 1개월에 안압, 나안시력, 세극등현미경검사, 타각 적굴절검사, Scheimpflug 영상 검사(Pentacam, Oculus Inc., Dutenhofen, Germany)를 시행하였다. LASEK 수술 전, 술 후 1개월째 Pentacam을 이용하여 측정한 각막 앞면과 뒷면 의 비구면도(Q-value), 중심 상승(Central elevation), 중심 각막두께, 앞방깊이, 앞방각, 앞방부피를 비교하였고, 수술 전 초음파각막두께측정치와 수술 전 Pentacam 각막두께 측정치를 비교하였다.
분류 및 통계방법
통계분석은 SPSS version 13.0을 각막 앞면과 뒷면의 비구 면도(Q-value), 중심 상승(Central elevation), 중심각막 두께, 앞방깊이, 앞방각, 앞방부피를 Paired sample
t
-test를 사용하여 비교하였고, 수술 전 초음파각막두께측정치와 수 술 전 Pentacam 각막두께측정치를 Paired samplet
-test를 사용하여 비교하였다.p
<0.05를 통계적으로 유의한 결과로 보았다.결 과
대상
환자의 진료기록을 후향적으로 분석하였다. 총 36명 71안 으로 남자가 7명 14안, 여자가 29명 57안이었고 환자들의 평 균나이는 28.3세였다. 술 전 평균 구면대응치는 -5.87±2.61 디옵터(범위 -1.75~-13.00)였고 초음파 각막두께측정계를 이용하여 측정한 중심각막두께는 547.15±29.30 μm였다.
비구면도(Q-value)
Pentacam을 이용하여 측정한 술 전과 술 후 1개월째 각 막 앞면의 비구면도는 통계적으로 유의한 차이를 보였다 (
p
=0.000)(Table 1). 각막 앞면의 비구면도는 술 전 평균 -0.2196에서 술 후 1개월째 평균 0.8800으로 변화하여 편 장한(Prolate)면이 편원의(Oblate)면으로 변화하는 양상을 보였다(Fig. 1). 술 전과 술 후 1개월째 각막 뒷면의 비구면 도는 통계적으로 유의한 차이가 없었다(p
=0.668)(Table 1). 각막 뒷면의 비구면도는 편원의 타원 형태가 유지되는 양상을 보였다(Fig. 1).중심각막두께
Pentacam을 이용하여 측정한 술 전과 술 후 1개월째 중심 각막두께는 술 전에 비해 중심각막두께가 얇아지는 양상을 보 였으며 통계적으로 유의한 차이를 보였다(
p
=0.000)(Table 2).각막중심 상승도
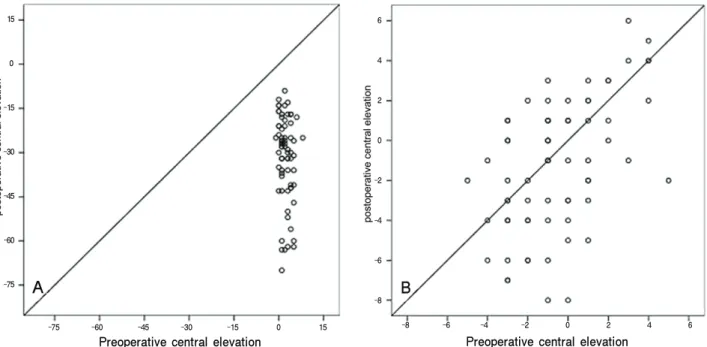
술 전과 술 후의 비교를 위하여 기준 best-fit sphere (BFS)를 술 전의 BFS로 고정하였다. Pentacam을 이용하 여 측정한 술 전과 술 후 1개월째 각막 앞면의 전위 정도는 통계적으로 유의한 차이를 보였다(
p
=0.000)(Table 3). 각 막 앞면의 전위 정도는 각막 앞면이 후방 전위하는 양상을 보였다(Fig. 2). 술 전과 술 후 1개월째 측정한 각막 뒷면의 전위 정도는 통계적으로 유의한 차이를 보이지 않았다(p
= 0.240)(Table 3)(Fig. 2).앞방척도
Pentacam을 이용하여 측정한 술 전과 술 후 1개월째 앞 방각, 앞방깊이, 앞방부피는 통계적으로 유의한 차이를 보 였다(
p
=0.001,p
=0.000,p
=0.000)(Table 4). 앞방각이 좁아지고, 앞방깊이가 얕아지며, 앞방부피가 줄어드는 양상 을 보였다(Fig. 3).Preoperative central elevation
-75 -60 -45 -30 -15 0 15 15
0
-15
-30
-45
-60
-75 A
-8 -6 -4 -2 0 2 4 6 6
4
2
0
-2
-4
-6
-8 B
Preoperative central elevation
Figure 2. The scatterplots for corneal central elevation between preoperative and postoperative states (at 1 month after operation). (A) Anterior corneal surface. Central elevation of anterior corneal surface was lower after operation.
(B) Posterior corneal surface. Central elevation of posterior corneal surface was unchanged after operation.
Preoperative-CE* Postoperative-CE†
Mean±SD∏(range) Mean±SD (range) p-value
A-CE‡(μm) 2.24±1.83 (-1 to 8) -31.75±14.41 (-70 to 9) 0.000
P-CE§ (μm) -0.48±2.25 (-5 to 5) -1.06±3.41 (-8 to 7) 0.101
*Preoperative-CE=Preoperative central elevation; †Postoperative-CE=Postoperative central elevation (at l month after operation); ‡A-CE=anterior central elevation; §P-CE=posterior central elevation; ∏SD=standard deviation.
Table 3.The comparison of anterior and posterior corneal central elevation between preoperative and postoperative state (at 1 month after operation)
고 찰
각막 앞면은 안구 전체에서 굴절력을 결정하는 가장 중 요한 요소로서 정상인에서 각막 앞면은 전체 굴절력의 80%를 이루고 있다. 각막은 구형이 아닌 비구면의 형태를 띠고 있으며, 이의 형태를 수치화하여 비구면도라 한다. 이 중 Q-value는 대표적인 비구면도를 나타내는 형태 요소 로서 Q-value가 0이면 원을 의미하고, -1에서 0 사이일 경우 편장한(prolate) 타원, Q-value가 -1이면 포물선 (parabola), -1보다 작은 경우 쌍곡선(hyperbola), 0보다 큰 경우 편원의 타원을 의미한다.16 본 연구에서 술 전의 각막 앞면의 Q-value가 평균 -0.2196, 각막 뒷면의 Q- value가 평균 0.1493로 앞면은 편장한 타원의 형태, 뒷면은 편원의 타원의 형태를 보이고 있다.
p
-factor는 비구면도를 나타내는 형태 요소로서p
-factor 는 Q-value에 1을 더한 값을 가진다.16 Anera et al13은LASIK 수술 후 각막의 비구면도 변화를
p
-factor를 이용하 여 측정하였다. 술 전 평균p
-factor는 0.88, 술 후 1개월 째 평균p
-factor는 1.65였다고 보고하였다. 본 연구에서 각막 앞면의 Q-value는 평균 -0.2196에서 0.8800로 변화 하여 편장한 타원이 편원의 타원 형태로 변하여 Anera et al 과 상응하는 결과를 보였다. 또한, 본 연구에서 각막 뒷면의 Q-value를 측정한 결과, 각막 뒷면의 Q-value는 평균 0.1493에서 0.1569로 변화하여 편원의 타원의 형태가 유지 되는 결과를 보였다.굴절교정수술 후 각막확장증에서 각막 뒷면이 앞쪽으로 전위되는 데, 이 전의 Orbscan을 이용한 연구에서 LASIK 수술 후 각막 뒷면이 앞쪽으로 전위 되는 양상을 보이며, 이는 LASIK 후 잠재성 각막확장증을 나타낸다고 하였으나, 최근 Pentacam을 이용한 연구에서 굴절교정수술 후 각막 뒷면의 유의한 앞쪽 전위는 나타나지 않는다고 하였다.14,15 Ciolino et al14은 LASIK 수술 후 각막 뒷면이 1개월 째 평
Preoperative value Postoperative value
parameter Mean±SD§(range) Mean±SD (range) p-value
ACD* (mm) 3.286±0.198 (2.80 to 3.80) 3.198±0.200 (2.72 to 3.75) 0.000
ACA† (°) 41.359±4.856 (32.9 to 53.9) 40.376±4.816 (31.0 to 52.5) 0.000
ACV‡ (mm3) 194.20±22.37 (134 to 251) 186.99±23.90 (124 to 242) 0.000
*ACD=anterior chamber depth; †ACA=anterior chamber angle; ‡ACV=anterior chamber volume; §SD=standard deviation.
Table 4. The comparison of anterior chamber parameter between preoperative and postoperative state (at 1 month after operation)
A
2.6 2.8 3.0 3.2 3.4 3.6 3.8 4.0 4.00
3.80
3.60
3.40
3.20
3.00
2.80
2.60
Preoperative anterior chamber depth
260
240
220
200
180
160
140
120 C
120 140 160 180 200 220 240 260
Preoperative anterior chamber volume
B
30.0 35.0 40.0 45.0 50.0 55.0 55.0
50.0
45.0
40.0
35.0
30.0
Preoperative anterior chamber angle
Figure 3. The scatterplots for anterior chamber para- meters between preoperative and postoperative states (at 1 month after operation). (A) Anterior chamber depth.
Anterior chamber depth had become shallow after operation. (B) Anterior chamber angle. Anterior chamber angle had become narrow after operation. (C) Anterior chamber volume. Anterior chamber volume had shrunk after operation.
균 -2.64 μm, 14개월째 -0.47 μm 앞쪽으로 전위한다고 하였다. 본 연구에서 각막 뒷면은 술 전 -0.48 μm에서 술 후 1개월째 -0.92 μm로 전위하여 통계적으로 유의한 차이를 보이지 않지만 Ciolino et al14의 연구와 달리 LASEK 수술
후 각막 뒷면이 미세하게 뒤쪽으로 전위하였다. 본 연구의 결과에서도 LASEK 수술 후 잠재성 각막확장증의 양상은 보이지 않았다.
Beijing eye study에서 중심각막이 두꺼우면 앞방깊이가
A B C D
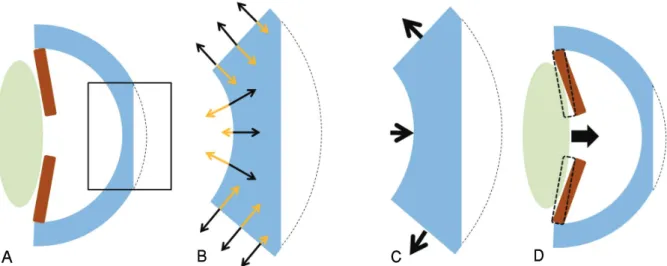
Figure 4.The schematic figures of change of the cornea after LASEK surgery. (A) Section of cornea during LASEK surgery. (B) Magnification of section plane and free body diagram. (C) Magnification of section plane and net force of free body diagram. Net force of free body diagram was directed posterior to anterior through axial plane. (D) Change of cornea and anterior chamber after LASEK surgery. Posterior cornea was not displaced and the anterior cornea was displaced posteriorly. Because of tensile strength, the iris was displaced anteriorly resulting in the anterior chamber angle, volume, and depth was decreased.
얕고, 앞방각이 좁다고 하였다.17본 연구에서 LASEK 수술 후 중심각막두께가 얇아지며 모든 앞방 척도들이 감소하였 는데, 이는 정상안과 굴절교정수술 후 상태는 다른 요인이 관여하기 때문일 것으로 보인다.
굴절교정수술 후 안압을 골드만 안압계로 측정 시 실제 보다 낮게 측정되며 이는 얇아진 중심각막두께와 관련이 깊다고 알려져 있다.18,19각막 기질의 세포외기질이 각막의 물리학적 특성을 대부분 결정하고 이는 각막 콜라겐 섬유 소원의 배열에 따라 달라진다.18Tamburrelli et al18은 굴절 교정수술 후 콜라겐 섬유소원 배열이 변하여 조직의 기계 적 세기가 달라지고 이는 안구 전체의 강도와 무관하게 각 막의 강도와 탄성에 영향을 주어 안압이 낮게 측정될 수 있 다고 하였다. Svedberg et al19은 보우만 층의 결여와 얇은 각막두께가 안압이 낮게 측정되는 원인이며 안압 측정 하 강의 정도는 절제 정도보다 수술 방법의 차이가 더욱 큰 영 향을 주어, PRK나 LASEK보다 LASIK 수술에서 안압이 더 욱 낮게 측정된다고 하였다. 이는 LASIK 수술은 PRK나 LASEK과 달리 각막 상피-보우만 층 복합체가 유지되어 각막 창상 치유과정에 변화를 주고 각막의 특성에 영향을 주기 때문이라고 하였다.
Tsukiyama et al20은 orthokreatology 렌즈 착용 후 각막 의 형태는 변하지만 앞방 깊이는 유의한 변화를 보이지 않 는다고 하였다. Emre et al21은 Pentacam을 이용한 연구에 서 외안근 절제 와 후전 동시 수술 후 중심각막두께는 변화 가 없지만, 앞방깊이가 얕아지고 앞방부피가 감소하는 경향
이 있다고 하였다. 즉, 안구 전체의 강도 및 장력의 변화는 앞방깊이에 영향을 줄 수 있다고 보여진다. 본 연구에서 술 후 각막 후면은 전위도는 변화하지 않고 앞방깊이가 얕아 지고 앞방각이 좁아지며 앞방부피가 감소하는 통계적으로 유의한 변화를 보였는데, 이는 LASEK 수술 후 중심각막두 께가 얇아지게 되면 자유물체도에 따라 각막 중심부에 응 력집중이 발생하며 안구 자체의 일정한 압력에 의해 각막 중심부에는 바깥쪽 방향의 힘이 증가하면서 안구 전체의 축에 따른 장력이 증가하게 되지만 각막 자체의 위치는 이 동하지 않고 홍채가 앞쪽으로 당겨지며 앞방척도가 변화하 는 것으로 보여진다(Fig. 4).
Wong et al22은 근시는 녹내장의 선행요인이라 하였으며, LASEK 수술은 굴절교정수술의 발전과 함께 젊은 연령에 서 흔하게 시행되고 있다. 본 연구에서 LASEK 수술 후 앞 방깊이가 얕아지고 앞방각이 좁아지며 앞방부피가 감소하 였는데, 근시 환자가 LASEK 수술을 시행 받고, 추후 녹내 장 검사를 시행하게 될 경우 앞방척도의 변화도 녹내장 검 사의 고려사항이 되어야 할 것이다.
결론적으로 장기적인 관찰이 필요하겠지만 Pentacam을 이용하여 LASEK 수술 후 1개월 째 각막과 앞방의 변화를 알아본 결과, 각막 앞면의 비구면도와 전위도가 변하는 반 면, 각막 뒷면의 비구면도와 전위도는 변화하지 않았다. 앞 방척도는 앞방깊이가 얕아지고 앞방각이 좁아지며 앞방부 피가 감소하였다. Pentacam은 각막 앞뒤 면과 함께 앞방척 도를 비침습적으로 손쉽게 측정할 수 있는 굴절교정수술
전 흔하게 시행되는 검사이므로, LASEK 수술과 같은 굴절 교정수술 전 Pentacam을 이용하여 측정한 결과 앞방각이 좁고, 앞방깊이가 얕은 환자는 앞방척도 또한 술 전에 고려 하여야 할 것으로 생각된다.
참고문헌
1) Kim ES, Jin KH. Evaluation of prophylactic use of mitomycin to inhibit haze formation after LASEK. J Korean Ophthalmol Soc 2007;48:623-9.
2) Swartz T, Marten L, Wang M. Measuring the cornea: the latest developments in corneal topography. Curr Opin Ophthalmol 2007;18:325-33.
3) Rabsiber TM, Khoramnia R, Auffarth GU. Anterior chamber measurement using Pentacam rotating Scheimpflug camera. J Cataract Refract Surg 2006;32:456-9.
4) Nemeth G, Vajas A, Kolozsvari B, et al. Anterior chamber depth measurements in phakic and pseudophakic eyes: Pentacam versus ultrasound device. J Cataract Refract Surg 2006;32:1331-5.
5) Buehl W, Stojanac D, Sacu S, et al. Comparison of three methods of measuring corneal thickness and anterior chamber depth. Am J Ophthalmol 2006;141:7-12.
6) Reuland MS, Reuland AJ, Nishi Y, Auffarth GU. Corneal radii and anterior chamber depth measurments using the IOLmaster versus the Pentacam. J Refract Surg 2007;23:368-73.
7) Elbaz U, Barkana Y, Gerber Y, et al. Comparison of different techniques of anterior chamber depth and keratometric measure- ments. Am J Ophthalmol 2007;143:48-53.
8) Shanker H, Taranath D, Santhirathelagan CT, Pesudovs K.
Anterior segment biometry with the Pentacam: Comprehensive assessment of repeatability of automated measurements. J Cataract Refract Surg 2008;34:103-13.
9) Chen D, Lam AK. Intrasession and intersession repeatability of the Pentacam system on posterior corneal assessement in the normal human eye. J Cataract Refract Surg 2007;33:448-54.
10) Sanctis UD, Loiacono C, Richiardi L, et al. Sensitivity and speci- ficity of posterior corneal elevation measured by Pentacam in discriminating keratoconus/subclinical keratoconus. Ophthalmo- logy 2008;9:1-6.
11) Ho JD, Tsai CY, Tsai RJ, et al. Validity of keratometric index:
evaluation by the Pentacam rotating Scheimpflug camera. J Cataract Refract Surg 2008;34:137-45.
12) Emre S, Doganay S, Yologlu S. Evaluation of anterior segment parameters in keratoconic eyes measured with the Pentacam system. J Cataract Refract Surg 2007;33:1708-12.
13) Anera RG, Jiménez JR, del Barci LJ, et al. Changes in corneal asphericity after laser in situe keratomileusis. J Cataract Refract Surg 2003;29:762-8.
14) Ciolino JB, Khachikian SS, Cortese MJ, Belin MW. Long-term stability of the posterior cornea after laser in situ keratomileusis. J Cataract Refract Surg 2007;33:1366-70.
15) Hashemi H, Mehravaran S. Corneal changes after laser refractive surgery for myopia: comparison of Orbscan II and Pentacam findings. J Cataract Refract Surg 2007;33:841-7.
16) Calossi A. Corneal asphericity and spherical aberration. J Refract Surg 2007;23:505-14.
17) Xu L, Cao WF, Wang YX, et al. Anterior chamber depth and chamber angle and their associations with ocular and general parameters: the Beijing eye study. Am J Ophthalmol 2008;145:
929-36.
18) Tamburrelli C, Giudiceandrea A, Vaiano AS, et al. Underestimate of tonometric reading after photorefractive keratectomy increases at higher intraocular pressure levels. Invest Ophthalmol Vis Sci 2005;46:3208-13.
19) Svedberg H, Chen E, Hamberg-Nyström H. Changes in corneal thickness and curvature after different excimer laser photo- refractive procedure and their impact on intraocular pressure measurements. Graefes Arch Clin Exp Ophthalmol 2005;243:
1218-20.
20) Tsukiyama J, Miyamoto Y, Higaki S, et al. Changes in the anterior and posterior radii of the corneal curvature and anterior chamber depth by orthokeratology. Eye Contact Lens 2008;34:
17-20.
21) Emre S, Çankaya C, Demirel S, Doganay S. Comparison of preoperative and postoperative anterior segment measurements with Pentacam in horizontal muscle surgery. Eur J Ophthalmol 2008;18:7-12.
22) Wong TY, Klein BE, Klein R, et al. Refractive errors, intraocular pressure, and glaucoma in a white population. Ophthalmology 2003;110:211-7.
=ABSTRACT=
Changes in the Cornea and Anterior Chamber After LASEK:
Pentacam Findings
Jin-Hyoung Park, MD
1, Ja-Hun Kang, MD, PhD
2, Kyung-Hyun Jin, MD, PhD
1Department of Ophthalmology, KyungHee University Medical Center1, Seoul, Korea Department of Ophthalmology, KyungHee University East-west Neo Medical Center2, Seoul, Korea
Purpose: We evaluated changes in the cornea and anterior chamber after LASEK using Pentacam to search for signs of subclinical keratectasia occurrence.
Methods: Seventy-one eyes of 36 patients who had received LASEK were enrolled in this study. All eyes were examined for asphericity of the anterior and posterior cornea (Q-value), anterior and posterior corneal displacement, central corneal thickness, anterior chamber depth, angle, and volume using Pentacam before surgery and again one month after the operation.
Results: The postoperative changes in the asphericity of the posterior cornea and posterior corneal displacement were not statistically significant(p=0.668, p=0.101). The anterior chamber depth, angle, and volume decreased by 0.088 mm, 0.983°, 7.21 mm3 after LASEK, respectively. (p=0.000) The postoperative changes in asphericity of the anterior cornea, anterior corneal displacement, and central corneal thickness were statistically significant(p=0.000).
Conclusions: In this study, we compared changes in the anterior chamber and cornea after LASEK using Pentacam. Changes in the anterior cornea were significant; however, the posterior cornea did not change significantly. The anterior chamber depth, anterior chamber angle, and volume were decreased one month after the operation, although further long-term follow-ups will be necessary to verify these findings.
J Korean Ophthalmol Soc 2009;50(4):510-517
Key Words: Anterior chamber, Cornea, LASEK, Pentacam
Address reprint requests to Kyung-Hyun Jin, MD, PhD Department of Ophthalmology, KyungHee University Hospital
#1 Hoegi-dong, Dongdaemun-gu, Seoul 130-702, Korea
Tel: 82-2-958-8451, Fax: 82-2-966-7340, E-mail: [email protected]