Address reprint requests to Hee Kyu Kwon, M.D., Ph.D.
Department of Physical Medicine and Rehabilitation, Korea University Anam Hospital Inchon-Ro 73, Seongbuk-Gu, Seoul, Republic of Korea
TEL: 82-2-2-920-5697, FAX: 82-2-929-9951, E-mail: [email protected] 투고일: 2013년 8월 26일, 수정일: 2013년 11월 11일, 게재확정일: 2013년 11월 11일
INTRODUCTION
An intraneural ganglion cyst is a rare non-neoplastic cyst caused by the accumulation of thick mucinous fluid in a dense fibrous capsule within the epineurium of peripheral nerves.
1,2Although the most frequently affect- ed site is the common peroneal nerve, other locations have also been reported, including the radial, ulnar, median, sciatic, tibial, and posterior interosseous nerves.
2Among these, intraneural ganglion cysts involving the tibial nerve are extremely rare. Thus far, less than 15 cases have been reported in the literature since the first report in 1967 by Friedlander.
2-7The most common clini- cal symptoms of this rare condition include leg paresthe- sia, pain, and motor deficit, which are similar to that of
lumbosacral disc disease. This article reports a case of an intraneural ganglion cyst involving the tibial nerve and discusses the diagnostic value of electromyography in this disorder.
CASE REPORT
A 48-year-old woman visited the clinic complaining of persistent pain and paresthesia in the right lower extrem- ity, especially in the sole. She had experienced right lower extremity tingling for over 1 year, and this symp- tom had worsened during the recent 2 months. She could not recall any history of trauma or injury to the right lower extremity, and did not have any history of diabetes mellitus or alcohol abuse. She had dwarfism and her
경골신경을 침범한 신경내 결절낭 - 증례보고 -
고려대학교 의과대학 안암병원 재활의학교실
최태웅∙권희규
– Abstract –
An Intraneural Ganglion Cyst Involving the Tibial Nerve: A Case Report
Tae Woong Choi, M.D., Hee Kyu Kwon, M.D., Ph.D.
Department of Physical Medicine and Rehabilitation, Korea University Anam Hospital, Seoul, Republic of Korea
신경내 결절낭이 경골신경에 발생하는 경우는 드물며, 현재까지 15건 이내로 문헌에서 보고되었다. 신 경내 결절낭은 국소적 통증부터 운동, 감각장애에 이르기까지 다양한 증상을 보일 수 있다. 신경내 결 절낭의 병태생리와 치료에 대해서는 그 동안 몇 가지 보고가 있었다. 저자들은 우측 하지, 특히 발바닥 에 지속되는 통증과 이상감각을 보였고, 경골신경을 침범하는 신경내 결절낭으로 진단 된 48세 여자를 보고한다. 또한 신경내 결절낭의 감별진단, 병태생리, 영상학적 소견, 치료, 근전도 검사의 진단적 가 치에 대해 논의하고자 한다.
Key Words: ganglion cysts, tibial nerve, electromyography
height was about 125 centimeters. The physical exami- nation was performed roughly focusing on the degenera- tive lumbosacral disc disease and demonstrated motor weakness on the right toe flexor (Medical Research Council [MRC]) grade III) and foot invertor (MRC grade II), and paresthesia in the right calf and sole. Deep ten- don reflexes and peripheral circulations were also nor- mal. Plain radiographs showed degenerative changes on multiple lumbar spines. Initially, the condition was con- sidered to be lumbosacral disc disease involving a nerve root. An electrophysiologic study was subsequently per- formed to determine the presumed nerve root lesion, S1
radiculopathy.
Nerve conduction study demonstrated that the conduc- tion of the right tibial, medial plantar sensory, peroneal motor and sural nerves was within normal limit. The tib- ial compound muscle action potential in the right side, however, was of low amplitude compared to the one in the left side. Latencies of F-wave were extremely short, but it could be assumed as being in the normal range considering her height. Latencies of H-reflex showed a borderline prolongation in the right side compared to the left side. (Table 1 and Table 2). Additionally, needle electromyography revealed normal motor unit action
– 99 – Table 1. Results of the Nerve Conduction Study (Motor Nerve)
Motor nerve Stimulation Recording Latency Amplitude Distance Velocity F-wave H-reflex
site site (ms) (mV) (cm) (m/s) latency (ms) latency (ms)
Right peroneal Ankle EDB 3.6 13.5 14 56.0 30.1
Fibular head EDB 6.1 13.5 17 58.3
Popliteal fossa EDB 7.3 13.2
Right tibial Ankle AH 3.1 12.8 17 51.5 30.8
Popliteal fossa AH 6.4 10.5 19.5
Left tibial Ankle AH 3.4 20.6 17 50.0 30.5
Popliteal fossa AH 6.8 19.6 18.4
EDB, extensor digitorum brevis; AH, abductor halluces.
Table 2. Results of the Nerve Conduction Study (Sensory Nerve)
Sensory nerve Stimulation Recording Onset latency Peak latency Amplitude Distance
site site (ms) (mV) (μV) (cm)
Right sural Calf Ankle 1.9 2.4 35 10
Right medial plantar Ankle Sole 1.9 2.5 20 10
Left medial plantar Ankle Sole 1.8 2.4 28 10
Table 3. Results of Needle Electromyography
Side Muscle Insertional activity Spontaneous Fib/PSW MUAP Recruitment
Right Tensor fascia lata N None N F
Vastus lateralis N None N F
Tibialis anterior N None N F
Peroneus longus N None N F
Gastrocnemius medialis N None N F
Soleus N abundant polyphasic discrete
Flexor hallucis longus N abundant No MUAP
Flexor digitorum longus N abundant polyphasic 2 MUAP
Tibialis posterior N abundant No MUAP
Abductor hallucis N few polyphasic R
Flexor digitorum brevis N few polyphasic R
L4/5, L5/S1 paravertebral muscle N None
Left Flexor digitorum longus N None N F
Gastrocnemius medialis N None N F
Flexor digitorum brevis increased None N F
L4/5, L5/S1 paravertebral muscle N None
Fib: fibrillation potential, PSW: positive sharp wave, MUAP: motor unit action potential, N: normal, F: full, R: reduced.
potentials with full recruitment patterns in the muscles routinely screened for radiculopathy (vastus lateralis, tib- ialis anterior, peroneus longus, tensor fascia lata and gas- trocnemius muscles). However, when the right flexor digitorum longus muscle was examined, abundant posi- tive sharp waves, fibrillation potentials, and only two motor unit action potentials were found in needle elec- tromyography. Then, needle electromyography was per- formed along the right tibial nerve innervated muscles, including the soleus, tibialis posterior, flexor hallucis longus, abductor hallucis, and flexor digitorum brevis muscles. Abnormal spontaneous activities similar to those found in the flexor digitorum longus muscle were detected in these muscles (Table 3), even though the abnormal spontaneous activities and recruitment patterns were relatively less in the abductor hallucis and flexor digitorum brevis muscles. Thus, the patient was diag-
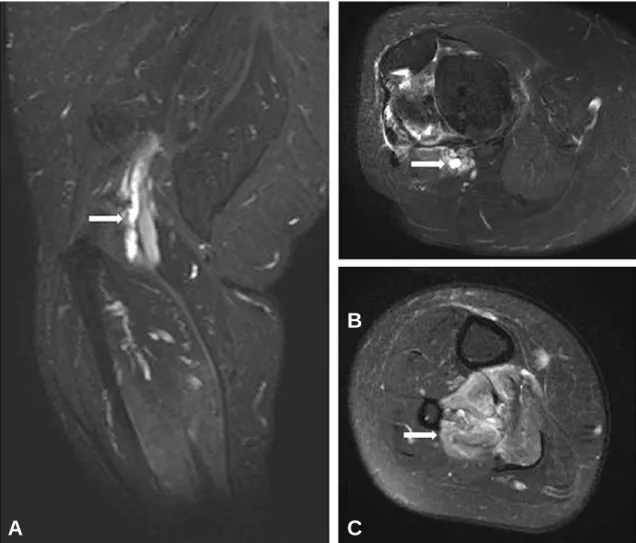
nosed as having right tibial neuropathy with partial axonotmesis distal to the branch to the gastrocnemius muscle. Magnetic resonance imaging (MRI) demonstrat- ed a perineural cystic lesion along the course of the distal sciatic and proximal tibial nerves in the right lower extremity. This elongated lesion measured approximately 8 cm in length and 0.6 cm in maximum diameter, and it appeared to have no direct connection with the knee joint or superior tibiofibular joint. Edema and mild atrophy in the right tibialis posterior, flexor digitorum longus, and soleus muscles were also noted, which were compatible with the tibial nerve denervation (Fig. 1). Together, the clinical symptoms, electrophysiologic findings, and radi- ologic features supported a diagnosis of an intraneural ganglion cyst involving the tibial nerve. She was then referred to an orthopedist for surgery, but she refused surgery and did not show up again. Three months after
Fig. 1. MRI (T2 weighted image) of the right lower extremity. (A) Perineural elongated shaped cystic lesion (arrow) along the course of the distal sciatic and proximal tibial nerves is demonstrated. The size of the cyst is 8 cm in length and 0.6 cm in maximum diameter. (B) The ganglion cyst (arrow) cause eccentric displacement of the nerve fascicles making signet ring sign. (C) Denervation of the right tibialis posterior and flexor digitorum longus muscles (arrow) are noted
A
B
C
her last visit, during a telephonic interview, she stated that she still had paresthesia over her right lower leg and felt no great difference since her last visit.
DISCUSSION
An intraneural ganglion cyst involving the tibial nerve is an extremely rare condition among ganglion cysts or popliteal masses. It has diverse clinical symptoms and commonly presents as a tender mass with local or radiat- ing pain and motor and sensory deficits.
Because of the rarity of this disease, it is crucial to dif- ferentiate it from other common disorders, including Baker’s cyst, meniscal cyst, bursitis, nerve sheath tumor and lumbosacral disc disease. Differential diagnoses can be achieved by physical examination and imaging stud- ies, such as ultrasonography and MRI. An electrophysio- logic study can help define the extent of nerve damage and distinguish it from lumbosacral disc disease, which has similar symptoms. A misdiagnosis of this condition as lumbar disc disease leading to an unsuccessful surgery was reported before.
8Numerous hypotheses have been proposed for the pathogenesis of intraneural ganglion cysts. A localized degenerative process of connective and perineural tissues secondary to the chronic mechanical irritation has been proposed earlier.
8A less convincing theory suggests that these cysts could arise from cystic degeneration of for- mer solid tumors.
9In addition, an intraneural hemorrhage secondary to trauma has also been proposed as a mecha- nism,
10even though the presence of hemosiderin deposits has not been a common finding. Recently, based on the analyses of clinical, surgical, and radiologic observa- tions, the unified articular theory has been brought up.
6It proposes that synovial joint fluid dissects through capsu- lar defects along the path with the least resistance and extends intra-epineurally along articular nerve branches.
6In case of an intraneural ganglion involving the tibial nerve, the cyst most commonly arises from the posterior aspect of the superior tibiofibular joint.
6Unfortunately, the connection with any nearby joint was not found in this case, suggesting that it does not support this unified articular theory.
Typical MRI findings in the intraneural ganglions have been described previously. Some of these findings sup- port the unified articular theory, which include the “tail sign” (identification of a narrow pedicle connection with a nearby joint), the “popliteus sign” (denervation and
atrophy of the popliteus muscle), and the “signet ring sign” (the eccentric displacement of the nerve fascicles by the intraneural cystic lesions).
The symptomatic intraneural ganglion cyst can be ini- tially treated by minimal invasive decompression, which reduces the tibial nerve compression and secondary mus- cle denervation. Percutaneous needle aspiration and steroid injection under ultrasound guidance can also be performed.
2However, long-term follow-up study is needed to determine the recurrence. In cases resistant to minimal invasive decompression, an open surgical approach is usually considered. It surgically removes the intraneural ganglion cyst and disconnects the articular branch, if present.
3-7The patient in this case, however, did not receive any treatment.
In spite of the proximal location of the cyst (up to the distal sciatic nerve) in our patient, she showed character- istics of tibial neuropathy with complete sparing of the gastrocnemius muscle. Additionally, the relatively less involved findings on needle electromyography of some distal muscles (abductor hallucis and flexor digitorum brevis) and nerve conduction studies of the tibial motor, sural, and medial plantar nerves imply the variable involvement of the nerve fascicles within the same tibial nerve, distinct from the processes in traumatic or com- pressive radiculopathies.
CONCLUSION
In conclusion, patients with intraneural ganglion cysts involving the tibial nerves may come to outpatient clin- ics complaining of affected leg pain and paresthesia. The similar clinical symptoms with lumbosacral disc diseases may lead to misdiagnoses resulting in unnecessary surg- eries. Precise needle electromyography is valuable in distinguishing tibial neuropathy caused by nerve com- pression from lumbosacral radiculopathy. MRI can be used to pinpoint the exact lesion location of an intraneur- al ganglion cyst.
REFERENCES
1. Brooks DM: Nerve compression by simple ganglia. J Bone Joint Surg Br 1952:34-B:391-400
2. Jose J, Fourzali R, Lesniak B, Kaplan L: Ultrasound-guid- ed aspiration of symptomatic intraneural ganglion cyst within the tibial nerve. Skeletal Radiol 2011:40:1473-1478 3. Adn M, Hamlat A, Morandi X, Guegan Y: Intraneural
– 101 –
ganglion cyst of the tibial nerve. Acta Neurochir (Wien) 2006:148:885-889:discussion 889-890
4. Friedlander HL: Intraneural ganglion of the tibial nerve. A case report. J Bone Joint Surg Am 1967:49:519-522 5. Patel P, Schucany WG: A rare case of intraneural ganglion
cyst involving the tibial nerve. Proc (Bayl Univ Med Cent) 2012:25:132-135
6. Spinner RJ, Mokhtarzadeh A, Schiefer TK, Krishnan KG, Kliot M, Amrami KK: The clinico-anatomic explanation for tibial intraneural ganglion cysts arising from the supe- rior tibiofibular joint. Skeletal Radiol 2007:36:281-292 7. Tseng KF, Hsu HC, Wang FC, Fong YC: Nerve sheath
ganglion of the tibial nerve presenting as a Baker's cyst: a case report. Knee Surg Sports Traumatol Arthrosc 2006:
14:880-884
8. Lang CJ, Neubauer U, Qaiyumi S, Fahlbusch R: Intraneur- al ganglion of the sciatic nerve: detection by ultrasound. J Neurol Neurosurg Psychiatry 1994:57:870-871
9. Scherman BM, Bilbao JM, Hudson AR, Briggs SJ: Intra- neural ganglion: a case report with electron microscopic observations. Neurosurgery 1981:8:487-490
10. Gurdjian ES, Larsen RD, Lindner DW: Intraneural cyst of the peroneal and ulnar nerves. Report of two cases. J Neu- rosurg 1965:23:76-78