203
•교신저자:문두건, 고려대학교 의과대학 비뇨기과학교실 서울시 구로구 구로동 80번지
Tel: 02-2626-3201, Fax: 02-2626-1321 E-mail: [email protected]
전체 글
•교신저자:문두건, 고려대학교 의과대학 비뇨기과학교실 서울시 구로구 구로동 80번지
Tel: 02-2626-3201, Fax: 02-2626-1321 E-mail: [email protected]
수치

관련 문서
The extracts of isolated from Coptis Radix conducted an antimicrobial activity against Staphylococcus aureus, Staphylococcus epidermidis, Escherichia coli, Candida
These compounds were tested for the antimicrobial activities using Staphylococcus aureus and Escherichia coli by way of tube dilution method. aureus at
A ll compounds showed fair bacteriostatic activity against Staphylococcus aureus 6538p, Bac.. illus subtilist Escherichia coli, and
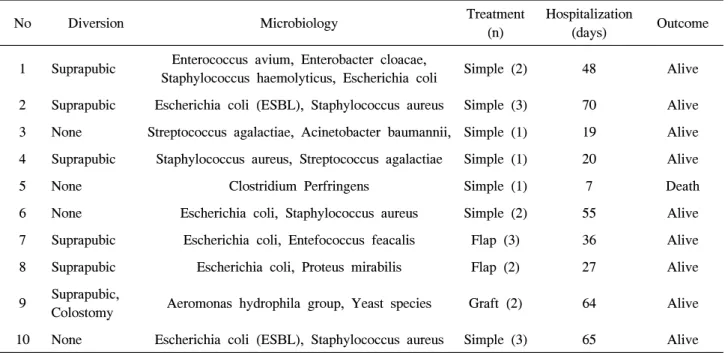
양성 환자에서 CNS (Coagulase-Negative Staphylococcus)균을 제외하고, Type1 환자 5명에서 Staphylococcus aureus, Escherichia coli, Acinetobacter Baumannii,
paper disc FDV-3 Staphylococcus aureus, Escherichia coli, Listeria monocytogenes, Pseudomonas aeruginosa, Salmonella typhimurium, Yersinia enterocolitica 와 Lodderomyces
Major foodborne pathogens, specifically Escherichia coli, Salmonella spp., Listeria monocytogenes, Campylobacter jejuni, Staphylococcus aureus, Vibrio
6종의 Gram 양성균(Clostridium botulinum, Bacillus subtilis, B. cereus, Staphylococcus aureus, Micrococcus luteus, Listeria monocyto- gens), 3 종의 Gram 음성균(Escherichia
There were no significant differences between the 2 groups in bacterial species (Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Pseudomonas aerugi- nosa) and
