책임저자:전 욱, 서울시 영등포구 영등포동 2가 94-200
150-719, 한림대학교 의과대학 한강성심병원 외과 Tel: 02-2639-5442, Fax: 02-2678-4386
E-mail: [email protected]
전층 화상환자에 있어서 Cryoderm의 임상적 유용성
김영민․양형태․임해준․김도헌․허 준․김종현․조용석․전 욱
한림대학교 의과대학 한강성심병원 외과Clinical Benefit of Cryoderm in Full Thickness Burns
Young Min Kim, M.D., Hyeong Tae Yang, M.D., Hae Jun Lim, M.D., Dohern Kim, M.D., Jun Hur, M.D., Jong Hyun Kim, M.D., Yong Suk Cho, M.D. and Wook Chun, M.D.
Department of Burn Surgery, Hangang Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
Purpose: CryoDerm (CGbio) is derived donated human skin.
After removing epidermis and fibroblast of dermal layer, it preserved with cryo-preservation technique using control rate freezer system. To prevent post burn joint contracture in massive burns, we have used CryoDerm in acute stage.
Methods: From January of 2010 to July of 2012, 50 patients
who undergone CryoDerm graft with split thickness skin graft were reviewed. The operative method was as follows: 1) Early wound excision and or cadaveric allograft skin cover- age was performed within 5 days after burn injury 2) 2∼3 weeks after wound excision, split thickness skin graft was performed with CryoDerm graft. Then graft take rate was in- vestigated by inspection. Follow up duration was 3∼32 months.Results: Mean age of patients was 42.2 (2∼70) years. Mean
percentage of total body surface area burned was 27.22% (1∼61%). Among 50 patients, 98 joints was operated including 14 hands, 4 wrists, 10 shoulders, 23 elbows, 4 necks, 3 hip joints, 31 knee joints and 9 ankles and feet. Total used graft size of Cryoderm was 10,945 cm2. Average take rate was near 100%.
Conclusion: Cryoderm graft with split thickness skin graft
can be used as a safe and effective operative method for one stage operation in acutely burned patients. (J Korean BurnSoc 2012;15:121-126)
Key Words: CryoDerm, CGbio, Artificial dermis, Full thick-
ness burns서 론
진피대체물에는 인체조직인 무세포동종진피와 동물의 콜라겐, 일라스틴 등으로 만든 인공진피가 있다
1). 기존의 무세포동종진피(Acellular Dermal Matrix, ADM)는 대부분 동결건조의 형태로 생산되었지만
2-6), 최근 국내에서 세계최 초로 동결보존무세포동종진피(Cryo-Preserved Acellular Dermal Matrix, CPADM)가 개발되었으며, 이러한 Cryo- Derm (CPADM, CGbio tissue bank)이 이식 인체조직으로서 효과적 제품인지 평가하기 위한 임상실험에 대한 연구이다.
대상 및 방법
1. 환자의 선정
2010년 1월 1일부터 2012년 7월 30일까지 한강성심병원 화상센터에 입원한 환자 중 Cryoderm을 사용한 환자들을 대상으로 환자들의 추적관찰을 통한 전향적인 방법으로 분 석하였다.
2. 화상에 대한 전반적 치료
연구의 대상이 된 모든 환자들은 초기 수액 치료를 시행 하였고, 화상센터 표준 치료방침에 따른 동일한 방법으로 치료하였다. 화상범위에 따라 초기 수액치료는 Parkland formula를 사용하였으며, 국소감염 및 전신감염에 대해 초 기에 경험적 항생제를 투여하였고, 주 2회의 균 배양검사를 통해 균 동정 이후에는 적절한 항생제를 선택하였다.
3. 수술 방법 및 추적 관찰
3도 화상으로 피부결손 부위에 피부이식을 시행하면서 동시에 CryoDerm을 이식하였다.
사용부위는 무세포동종진피가 의료보험적용이 되는 관
절부위로 국한하였다. 중화상환자의 경우에는 조기가피절
제술 및 사체피부이식술 시행 후 2∼4주 경과한 시점에
CryoDerm과 부분층식피술을 동시이식 하였다. 이식 후 3
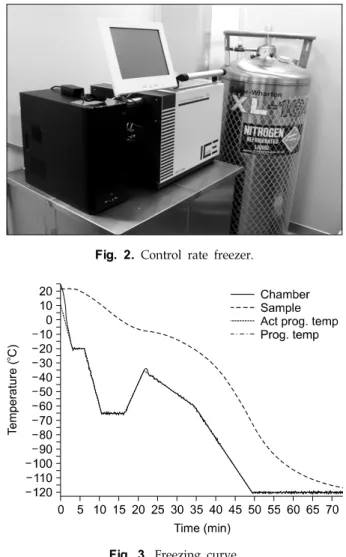
Fig. 1. Cryo-preserved acellular dermal matrix, CPADM. Fig. 3. Freezing curve.
Fig. 4. Proteome profiler human angiogenesis array result for Cryoderm.
Fig. 2. Control rate freezer.
개월에서 32개월 간 외래 추적관찰을 시행하면서 이식성공 률과 부작용을 확인하였다.
결 과
50명의 환자(남자 35명, 여자 15명)에서 시술되었다. 화상 의 평균 넓이는 27.22% TBSA Burned (1∼61%)이며, 환자 들의 평균 나이 42.26세(2∼70세)였다.
수술부위는 수부 14, 손목관절 4, 어깨관절 10, 팔꿈치관절
23, 경부관절 4, 엉덩이관절 3, 무릎관절 31, 족부 및 발목관
절 9 등 총 98관절이었다. 사용된 CryoDerm은 10946 cm
2,
평균 1환자 당 218.9 (20∼577) cm
2, 1관절 당 111.7cm
2사용
되었다. 사용 후 효과적으로 진피대체물의 기능을 수행하
Fig. 6. Case: 50 years male, electrical burn, 30% TBSA burned. (A) 2 days after admission, full thickness burns on, the both hands,
(B) 7 days after escharectomy and allograft, (C) 7 days after STSG with cryoderm, (D) 30 days after STSG with cryoderm, (E, F) Post-operation 2 years later.Fig. 5. Strain-Stress curve of CPADM, FDADM #1, FDADM #2.
CPADM = cryo-preserved acellular dermal matrix, FDADM = freeze dried acellular dermal matrix.
였으며, 이식 성공률은 거의 100%였다. 피부식피편 생착율 도 98% 이상이었지만 3예에서는 부분적으로 부분층식피술 을 재차 시행하였다.
고 찰
중증화상환자에서는 상처 감염에 의한 패혈증을 예방하
기 위해 조기가피절제술, 사체피부이식술을 보통 4∼7일 이내에 시행하게 된다
7-10). 이후 가피 절제 부위에는 시간이 경과함에 따라 신생혈관이 풍부한 콜라겐, 즉 육아조직이 발생하게 된다
11,12). 이 때 피부이식을 시행하며, 콜라겐은 반흔의 원인이기에 최대한 제거한 후, 신생혈관에 식피편 이나 진피대체물을 이식하게 된다. 진피대체물은 미용목적 이나 수술 후 관절운동 장애를 최소화하기 위해 사용된다
13). 진피대체물에는 송아지나 돼지의 콜라겐을 이용해 만든 인 공진피와 기증받은 사람의 피부로 만든 동종진피로 크게 나눌 수 있다.
인공진피를 만들기 위해서는 동물의 콜라겐을 추출한 후 이를 동결건조기를 이용하여 스펀지 구조를 가진 세포담체 (scaffold)를 만들게 된다. 콜라겐의 분해 속도는 가교 (crosslink) 정도에 따라 조절할 수 있다
14-16). 이러한 인공진 피의 공극의 크기는 보통 50마이크론 이하이며, 이곳으로 환자의 섬유아세포(fibroblast) 등이 이동하여 환자 본인의 콜라겐을 만들게 되며, 세포담체는 천천히 분해 흡수 되어 지게 된다
17,18).
반면에 동종진피는 기증받은 사람의 피부로부터 만들어
지는데, 우선 표피를 제거한 후 진피에 있는 세포도 모두
제거하여 영구 이식이 가능토록 한다. 일반적으로 이후에
는 동결건조를 시켜 보관하는 것이 일반적이었지만
19-25),
CryoDerm은 동결보존한 제품이다(Fig. 1). 최적의 동결보
Patient
number Age Sex Cause of burn
% TBSA burned
% Full thickness
burned
Site of cryoderm graft
Cryoderm graft size
(cm2)
Cryoderm graft after cadaevaric
allograft
Take rate (%) (Skingraft)
1 50 F FB 40 30 Lt. shoulder, axilla 158 Y 100
2 43 F SB 6 6 Rt. elbow (antecubital) 138 N 100
3 37 F CoB 1 1 Lt. knee (patella) 35 N 100
4 52 M EB 5 5 Both palm with finger 110 Y 100
5 54 M FB 23 23 Both knee (poplitreal) 486 Y 100
6 8 M CoB 4 4 Rt. knee (lateral side) 75 N 100
7 55 M FB 19 10 Rt. elbow (antecubital) 168 N 100
8 50 M EB 30 25 Both hands (dorsum), neck 282 Y 100
9 4 F SB 50 50 Both inguinal, both elbow (antecubital) 112 Y 100
10 53 M FB 46 40 Both knee (poplitreal) 236 Y 100
11 43 M FB 27 27 Rt. knee, Rt. axilla 490 Y 95
12 21 M EB 50 30 Lt. knee, Lt. ankle 226 Y 100
13 58 M FB 20 20 Lt. knee, Lt. ankle, Lt. foot 510 Y 100
14 43 M FB 27 22 Rt. knee, Rt. ankle, Rt. axilla 305 Y 90
15 5 F SB 14 10 Rt. knee 44 N 100
16 2 M SB 16 14 Rt. elbow (antecubital) 55 Y 95
17 70 F CoB 10 10 Rt. hand (dorsum) 16 Y 100
18 6 M SB 4 4 Lt. elbow, Lt. shoulder 100 N 100
19 43 M FB 32 30 Both ankle, both knee 446 Y 100
20 27 M FB 12 10 Rt. ankle 120 Y 100
21 45 M FB 33 28 Both knee 312 Y 100
22 66 M FB 30 30 Both knee 330 Y 100
23 52 M FB 38 30 Both knee 482 Y 100
24 47 F FB 32 25 Both hands, Rt. elbow 404 Y 100
25 51 F FB 61 55 Both hands 183 Y 100
26 57 F SB 19 19 Rt. elbow 130 N 100
27 39 M FB 27 27 Lt. hand 64 Y 100
28 45 M FB 22 22 Neck, both shoulder, Lt. shoulder 264 Y 100
29 48 F FB 20 20 Rt. shoulder, Rt. elbow 150 N 100
30 36 M SB 14 14 Lt. elbow 119 N 100
31 41 M SpB 29 25 Both elbow 136 Y 100
32 38 M FB 20 20 Lt. knee 145 Y 100
33 54 M FB 46 40 Lt. hand, Lt. elbow 261 Y 98
34 54 M EB 40 20 Rt. wrist 105 Y 100
35 28 M FB 50 45 Rt. elbow 193 Y 100
36 52 F FB 18 15 Neck, Rt. wrist, Rt. shoulder, Lt. elbow 319 Y 98
37 45 M CB 37 30 Both ankle, Rt. knee, Lt. knee 286 Y 100
38 57 M FB 11 11 Both hands (9 fingers) 239 Y 100
39 33 M FB 40 40 Lt. inguinal bone 20 Y 100
40 31 M FB 47 36 Both knee, both elbow 347 Y 90
41 13 M SB 25 20 Lt. elbow & shoulder 280 Y 100
42 55 F SB 45 35 Rt. elbow, both knee 298 Y 100
43 60 M FB 12 12 Lt. hand (5 finger) 97 Y 100
44 42 M FB 35 30 Lt. knee, neck 408 Y 100
45 56 F SB 33 20 Both arm, both shoulder 81 Y 100
46 30 M CoB 20 10 Rt. wrist 28 N 100
47 62 F SB 22 17 Rt. wrist, Rt. elbow 161 Y 100
48 56 M FB 53 45 Both knee 314 Y 100
49 38 M SB 20 20 Lt. knee 89 Y 100
50 58 F SB 26 21 Lt. knee 73 Y 100
Table 1. Summary of Data
존을 위해 많은 기술이 사용되었는데, 프로그램 극저온 동 결기(control rate freezer, CRF)와 동결보호제 등이다. 일반 적으로 물 결정은 영하 130도 이하에서는 그 형태가 유리처 럼 변하게 되며, 세포의 손상을 최소화 할 수 있게 된다. 프 로그램 극저온 동결기는 액체질소를 이용하여 인체조직을 섭씨 영하 180도까지 떨어트릴 수 있는 기계이다(Fig. 2).
인체조직은 온도가 영하로 내려가면서 용융열(heat of fu- sion)이 순간적으로 발생하게 되며, 이로 인해서도 손상 받 을 수 있다. 따라서 극저온 동결기(CRF) chamber의 온도를 용융열이 발생하기 직전에 낮춤으로 동결곡선의 커브를 최 적화할 수 있다(Fig. 3). 생산 시에는 항상 동일한 조건(피부 이식조직과 동결보호제의 혼합비율 등)으로 가공을 해야 하며, 가공조직은행에서는 표준업무지침서에 이를 명시해 놓고 있다.
즉, 동종진피는 동결건조무세포동종진피(Freeze dried acellular dermal matrix, FDADM)와 동결보존무세포동종 진피(Cryo-preserved acellular dermal matrix, CPADM)로 나누어지게 되며, CryoDerm은 후자인 셈이다.
CPADM은 FDADM에 비하여 해부학적 구조가 살아있 는 피부와 매우 유사하며, 이식 성공률을 높이기 위해 고안 되었다. 혈관 구조가 대부분 유지되어 있으므로 창상기저 부(wound bed)와의 혈관연결이 훨씬 빠르게 된다. CryoDerm 은 탄력성이 매우 우수하며, 혈종 흡수력 또한 뛰어나다. 무 엇보다도 촉감과 신축성이 살아있는 피부와 거의 같아, 피 부이식 시에 간편하게 사용할 수 있다. 특히 감염에 매우 강해, 수술부위에 균이 많은 급성기 중화상환자에서 매우 유용하다. 또한 많은 성장인자를 분비하여 창상치유에 도 움을 주게 된다(Fig. 4). CryoDerm은 FDADM에 비해 원형 을 최대한 유지하도록 고안되었기 때문에 장력(tensile strength)도 훨씬 강하게 유지된다(Fig. 5). 또한 최적의 제 품을 만들기 위해, 기증자에서 채취된 피부는 24시간 안에 가공을 시작하게 되며 무균실(class 10)에서 가공을 하게 된 다. 하지만 CPADM은 국내 기증자 피부원재료부터만 만들 수 있어, 원재료 양이 적다거나 너무 얇아 적합하지 않다면 생산이 어렵다는 단점이 있다.
CryoDerm에는 얇은 제품(두께 10∼14/1000 인치)과 두 꺼운 제품(두께 14∼20/1000 인치)이 있으며 이는 기증 피 부의 두께에 따라 결정되게 된다. 3예에서는 CryoDerm은 생착이 잘되었지만, 그 위의 식피편이 일부 괴사되었는데, 모두 두꺼운 제품을 사용한 예였다. 3예 모두 부분적으로 부분층식피술을 재차 시행하였으며 결과는 매우 양호하였 다.
현재 CryoDerm 사용자 중 1년 이상 경과한 환자에서 수 술부위에 대한 관절운동범위 측정, 흉터두께측정, 피부탄력
도 측정, 색소침착도 등의 검사를 진행 중이며 차후에 결과 를 보고할 계획이다(Fig. 6).
결 론
세계 최초로 개발된 동결보존무세포동종진피인 CryoDerm 은 효과적으로 진피대체물의 역할을 수행하고 있으며 (Table 1), 현재 진행 중인 사용부위 반흔 평가 및 기능평가 가 완료된다면 더욱 정확한 기능을 알 수 있을 것이다.
REFERENCES
1) Braye F, Hautier A, Bouez C, Damour O. Skin substitutes reconstructed in the laboratory: application in burn treatment [in French]. Pathol Biol (Paris). 2005;53:613-617.
2) Fang CH, Robb EC, Yu GS, Alexander JW, Warden GD.
Observations on stability and contraction of composite skin grafts: xenodermis or allodermis with an isograft overlay. J Burn Care Rehabil. 1990;11:538-542.
3) Grillo HC, McKhann CF. The acceptance and Evolution of Dermal homografts freed of viable cells. Transplantation.
1964;2:48-59.
4) Ben-Bassat H, Eldad A, Chaouat M. Structural and functional evaluation of modifications in the composite skin graft:
cryopreserved dermis and cultured keratinocytes. Plast Reconstr Surg. 1992;89:510-520.
5) Medalie DA, Eming SA, Tompkins RG, Yarmush ML, Krueger GG, Morgan JR. Evaluation of human skin reconstituted from composite grafts of cultured keratinocytes and human acellular dermis transplanted to athymic mice. J Invest Dermatol. 1996;
107:121-127.
6) Medalie DA, Tompkins RG, Morgan JR. Evaluation of acellular human dermis as a dermal analog in a composite skin graft. Asaio J. 1996;42:M455-M62.
7) Brusselaers N, Hoste EA, Monstrey S. Outcome and changes over time in survival following severe burns from 1985 to 2004. Intensive Care Med. 2005;31:1648-1653.
8) Barret JP, Herndon DN. Effects of burn wound excision on bacterial colonization and invasion. Plast Reconstr Surg.
2003111:744-750.
9) Blot S, Brusselaers N, Monstrey S. Belgian Outcome in Burn Injury Study Group. Development and validation of a model for prediction of mortality in patients with acute burn injury.
Br J Surg. 2009;96:111-117.
10) Brusselaers N, Juhasz I, Erdei I, Monstrey S, Blot S. Evalua- tion of mortality following severe burns injury in Hungary:
external validation of a prediction model developed on Belgian burn data. Burns. 2009;35:1009–1014; doi: 10.1016/
j.burns.2008.1012.1017.
11) Grinnell F. Fibroblasts, myofibroblasts, and wound contrac- tion. J Cell Biol. 1994;124:401-404.
12) van den Bogaerdt AJ, van Zuijlen PP, van Galen M, Lamme
EN, Middelkoop E. The suitability of cells from different tissues for use in tissue-engineered skin substitutes. Arch Dermatol Res. 2002;294:135-142.
13) Brusselaers N, Lafaire C, Ortiz S, Jacquemin D, Monstrey S.
The consensus of the surgical treatment of burn injuries in Belgium. Acta Chir Belg. 2008;108:645-650.
14) Pachence JM. Collagen-based devices for soft tissue repair. J Biomed Mater Res. 1996;33:35-40.
15) de Vries HJ, Middelkoop E, van Heemstra-Hoen M, Wildevuur CH, Westerhof W. Stromal cells from subcutaneous adipose tissue seeded in a native collagen/elastin dermal substitute reduce wound contraction in full thickness skin defects. Lab Invest. 1995;73:532-540.
16) de Vries HJ, Middelkoop E, Mekkes JR, Dutrieux RP, Wildevuur CH, Westerhof H. Dermal regeneration in native non-cross-linked collagen sponges with different extracellular matrix molecules. Wound Repair Regen. 1994;2:37-47.
17) Schulz JT III, Tompkins RG, Burke JF. Artificial skin. Annu Rev Med. 2000;51:231-244.
18) Suzuki S, Kawai K, Ashoori F, Morimoto N, Nishimura Y, Ikada Y. Long-term follow-up study of artificial dermis
composed of outer silicone layer and inner collagen sponge.
Br J Plast Surg. 2000;53:659-66.
19) Grinnell F. Fibroblasts, myofibroblasts, and wound contrac- tion. J Cell Biol. 1994;124:401-404.
20) Wainwright D, Madden M, Luterman A. Clinical evaluation of an acellular allograft dermal matrix in full-thickness burns.
J Burn Care Rehabil. 1996;17:124-136.
21) Characterization of acellular dermal matrices (ADMs) prepared by two different methods. Burns. 1998;24:104-113.
22) Livesey SA, Herndon DN, Hollyoak MA, Atkinson YH, Nag A. Transplanted acellular allograft dermal matrix. Potential as a template for the reconstruction of viable dermis. Trans- plantation. 1995;60:1-9.
23) Kirsner RS, Falanga V, Eaglstein WH. The development of bioengineered skin. Trends Biotechnol. 1998;16:246-249.
24) Rennekampff HO, Hansbrough JF, Woods V Jr, Kiessig V.
Integrin and matrix molecule expression in cultured skin replacements. J Burn Care Rehabil. 1996;17:213-221.
25) Jones I, Currie L, Martin R. A guide to biological skin sub- stitutes. Br J Plast Surg. 2002;55:185-193.