대한소화기학회지 2008;52:69-79 □ REVIEW □
연락처: 김광하, 602-739, 부산시 서구 아미동 1가 10 부산대학교 의학전문대학원 내과학교실 Tel: (051) 240-7869, Fax: (051) 244-8180 E-mail: doc0224@chol.com
Correspondence to: Gwang Ha Kim, M.D.
Department of Internal Medicine, Pusan National University School of Medicine, 10, Ami-dong 1-ga, Seo-gu, Busan 602- 739, Korea
Tel: +82-51-240-7869, Fax: +82-51-244-8180 E-mail: doc0224@chol.com
위식도역류질환의 식도 외 증상
부산대학교 의학전문대학원 내과학교실
김 광 하
Extraesophageal Manifestations of Gastroesophageal Reflux Disease
Gwang Ha Kim, M.D.
Department of Internal Medicine, Pusan National University School of Medicine, Busan, Korea
Gastroesophageal reflux disease (GERD) often presents as typical symptoms such as heartburn or acid regurgi- tation. However, a subgroup of patients presents a collection of symptoms and signs that are not directly related to esophageal damage. These are known collectively as the extraesophageal manifestations of GERD, such as non-cardiac chest pain, laryngitis, chronic cough, hoarseness, asthma or dental erosion. They have a common pathophysiology, involving microaspiration of acid into the larynx and pharynx, and vagally mediated broncho- spasm and laryngospasm. The role of extraesophageal reflux in such disorders is underestimated due to often si- lent symptoms and difficult confirmation of diagnosis. Endoscopy and pH monitoring are insensitive and therefore not useful in many patients as diagnostic modalities. Thus, anti-secretory therapy by proton pump inhibitor is used as both a diagnostic trial and as a therapy in the majority. Attention to optimizing therapy and judicious use of endoscopy and reflux monitoring are needed to maximize treatment success. (Korean J Gastroenterol 2008;52:69-79)
Key Words: Gastroesophageal reflux disease; Extraesophageal manifestation
서 론
최근 발표된 위식도역류질환의 Montreal 정의와 분류에서 는 가슴쓰림과 산 역류와 같은 전형적인 증상 외에도 이와 연관되어 나타날 수 있는 비전형적인 증상들에 대한 연관성 을 따로 나누어 분류함으로써 과거에 간과되었던 식도 외 증상들에 대한 관심도가 증가되고 있다(Fig. 1).1
실제로 위식도역류질환의 식도 외 증상과 징후는 실제 임 상에 있어 진단과 치료 방침 결정에 종종 어려움을 준다. 환 자가 인후두 증상이나 호흡기 증상을 호소하여 내원한 경우
에 불필요한 검사를 최소화하고 만족스러운 치료 효과를 얻 기 위해서는 신중한 접근이 필요하다. 이러한 환자에서 가 슴쓰림과 같은 전형적인 증상이 없는 경우가 많기 때문에, 병력 청취만으로 위식도역류와의 연관성을 의심하기는 쉽 지 않다. 내시경 검사를 하더라도 이상 소견이 없는 경우가 상당수이므로, 이러한 일반적인 검사방법은 크게 유용성이 없다. 또한 24시간 보행 식도 pH 검사나 임피던스 검사가 위식도역류와 식도 외 증상과의 연관성을 파악하는 데에는 도움이 되지만, 양자펌프억제제와 같은 항역류 치료의 성공 여부에 대한 예측에는 유용성이 떨어진다는 한계점을 가지
70 대한소화기학회지: 제52권 제2호, 2008
Fig. 1. The Montreal definition of gastroesophageal reflux dis- ease and its constituent synd- romes.
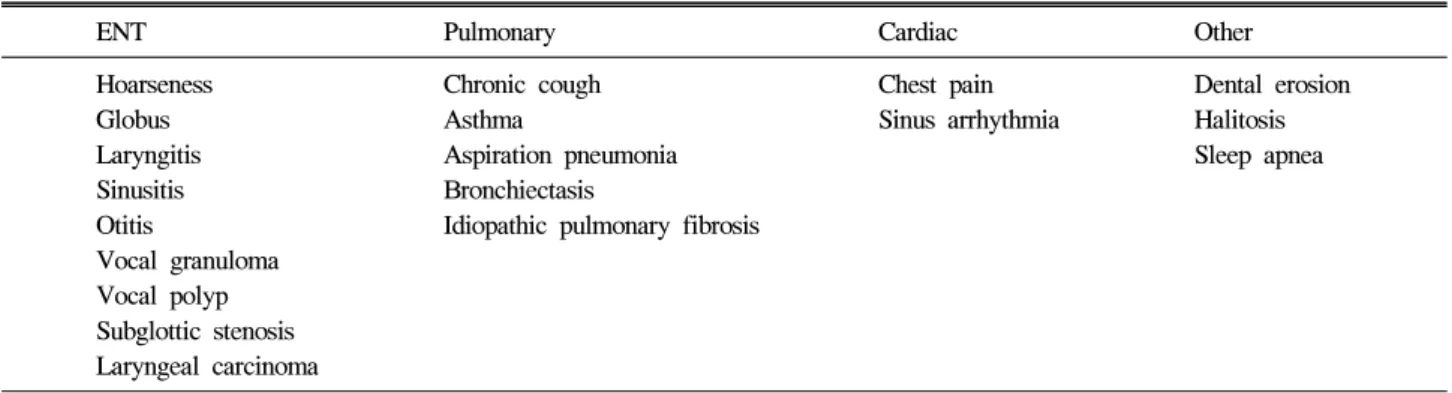
Table 1. Extraesophageal Manifestations of Gastroesophageal Reflux Disease
ENT Pulmonary Cardiac Other
Hoarseness Globus Laryngitis Sinusitis Otitis
Vocal granuloma Vocal polyp Subglottic stenosis Laryngeal carcinoma
Chronic cough Asthma
Aspiration pneumonia Bronchiectasis
Idiopathic pulmonary fibrosis
Chest pain Sinus arrhythmia
Dental erosion Halitosis Sleep apnea
Table 2. Proposed Mechanisms for Extraesophageal Manife- stations of Gastroesophageal Reflux Disease
Direct contact with gastric contents (reflux theory) - microaspiration of acid into the larynx and pharynx Neurally mediated reflex (reflex theory)
- vagovagal reflex triggered by distal esophageal acid reflux 고 있다.
이번 원고에서는 실제 임상 진료에 필요한 식도 외 증상 과 그 기전에 대한 검토와 함께, 이러한 환자들에 대한 진단 과 치료적 접근에 대해 기술하고자 한다.
식도 외 증상과 징후
실제로 위식도역류질환 환자들에서 어느 정도의 빈도로 식도 외 증상이 나타나는가를 살펴보면 Minnesota에 거주하 는 인구를 대상으로 시행한 한 조사에서는 주 1회 이상의 가슴쓰림을 가지고 있는 사람의 80%에서 비전형적인 식도 외 증상을 호소함을 보고하였다.2 유럽에서 시행한 전향 연 구에서도 미란 식도염이 있는 환자의 32.8%에서, 비미란 식 도염 환자의 30.5%에서 비전형적인 증상을 호소하였고,3 국 내에서도 위식도역류질환 환자들에서 쉰 목소리(55%), 인두 구(45%), 만성 기침(25%), 비심인 흉통(20%) 등의 순으로 비 전형적인 증상이 있음을 보고한 바 있다.4
임상에서 위식도역류질환과의 연관성을 고려해야 하는 인후두 증상들은 많으며, 이에 해당하는 증상으로는 만성 기침(chronic cough),5 장기간의 쉰 목소리(hoarseness),6 인두 구(globus pharyngeus),7 잦은 목 청소(throat clearing)8 등이 있 다(Table 1). 많은 환자들은 한 가지 이상의 증상을 같이 호 소하며, 이비인후과 검사에서 흔히 후인두역류 (laryngo- pharyngeal reflux)와 연관성을 시사하는 징후로는 후부 후두
염(posterior laryngitis),9 성대 결절(vocal nodule),10 성대 및 피 골 내벽 부종(vocal fold or arytenoid edema),11 육아종(granu- loma),12 부비동염(sinusitis),13 치아 후식(dental caries)14 등이 있다. 또한 후두암종(laryngeal carcinoma),15 성대문 연축 (laryngospasm),16 후두 협착(laryngeal stenosis)17과의 연관성 도 보고되고 있어 이러한 환자들에서 위식도역류질환이 하 나의 보조인자로 작용할 것으로 보인다.
위식도역류질환과의 연관성이 의심되는 호흡기 증상으로 는 기관지 천식(bronchial asthma),18 만성 기침,5 특발 폐섬유 증(idiopathic pulmonary fibrosis)19이 있으며, 이 외에도 흡인 폐렴(aspiration pneumonia), 만성 기관지염(chronic bronchi- tis), 기관지 확장증(bronchiectasis)도 위식도역류질환과 연관 성이 있는 것으로 알려져 있다.20,21
비심인 흉통의 원인으로서 위식도역류질환의 역할에 대 해서는 많은 연구들에서 보고되고 있으며,22,23 실제 임상에 서도 심장 검사에서 이상이 없는 경우 소화기내과로 의뢰되 는 경우들이 많은 실정이다.
김광하. 위식도역류질환의 식도 외 증상 71
지금부터 각각의 증상과 징후에 대한 구체적인 내용과 그 기전에 대해서 자세히 살펴보고자 한다(Table 1, 2).
1. 비심인 흉통
협심증과 유사한 흉골하 통증이 반복되지만, 심장으로 기 인한 경우가 아닐 때를 비심인 흉통으로 정의하고 있다.24 비심인 흉통을 유발할 수 있는 원인에는 여러 가지가 있는 데, 그 중에서도 가장 주된 원인은 식도에서 기인하며, 특히 위식도역류질환이 비심인 흉통의 가장 흔한 원인질환으로 알려져 있다.22,23 실제로 비심인 흉통 환자에서 24시간 pH 검사 결과 50-60%에서 비정상적인 위식도역류가 있었고, 이 러한 환자에서 위산억제제 투여에 의해 흉통이 호전되었다 고 보고되고 있다.23-25
심장과 식도는 같은 발생학적인 기원을 가지므로 식도에 의한 통증과 심장에 의한 통증이 명확히 구별되지 못하는 것이 당연한 면도 있다. 그러나 위식도역류와 관련된 흉통 은 전형적인 심인 흉통과 몇 가지 점에서 차이가 있다. 위식 도역류에 의한 흉통은 협심증에서처럼 쥐어짜는 듯한 또는 흉골 아래의 타는 듯한 통증으로 등이나 팔로 전파되기도 하지만, 식사 후 특히 누운 자세에서 통증이 악화되고 통증 때문에 잠에서 깨기도 하고 스트레스로 인해서 증상이 심해 질 수 있다. 또한 통증의 지속시간은 수 시간 또는 수 일까 지 지속되기도 하고, 음식이나 제산제에 의해서 완화되기도 한다.
하지만 증상만으로 두 질환을 감별하는 것은 다소 어려운 점이 있다. 실제로 관상동맥 질환을 가지고 있는 환자의 약 50%에서 적어도 한 가지 이상의 식도 질환의 증세를 보일 수 있으며,26 운동량이 증가함에 따라 흉통이 심해지면 협심 증의 가능성이 높지만 몸을 앞으로 웅크린 채 격한 운동을 하면 위식도역류가 조장되어 흉통이 발생하기도 하고 이러 한 경우에 설하 nitrates 투여로 흉통이 완화될 수 있어 협심 증과의 감별이 더욱 어려워진다.27 또한 위산의 역류가 미주 신경을 자극하여 관상동맥의 경련을 일으키기도 한다. 누운 자세에서 증세가 발생하면 위식도 역류에 의한 통증일 가능 성이 크지만 드물게는 협심증도 누운 자세에서 유발될 수 있다. 이러한 여러 가지 이유로 두 질환을 감별하는 데 많은 어려움이 따르며, 실제로 흉통이 발생한 환자에서는 우선적 으로 심장에 대한 검사를 시행하는 것이 추천된다.
산 역류에 의한 식도 자극이 흉통을 유발하는 기전에 대 해서는 잘 알려져 있지 않은데, Balaban 등은 산 역류로 인 한 식도 종주근의 수축이 단기간 지속될 경우(sustained esopha- geal contraction) 흉통이 발생될 수 있다고 제시하였다.28
2. 호흡기 증상
호흡기 증상은 주로 야간시간에 잘 발생하는데, 이는 수
면 중 상부 기도가 부분적으로 좁아지거나 폐쇄되면 흉곽 내 압력이 증가하고, 그 결과 위산 역류의 빈도가 증가되어 결국 호흡기 증상이 유발되기 때문이다.20
1) 기관지 천식
기관지 천식을 가진 환자의 80%에서 병적인 위식도역류 가 관찰된다.29 많은 역학 연구에서 위식도역류질환과 기관 지 천식의 연관성이 보고되고 있으며, 일부 연구에서는 두 질환이 동시에 존재하여 서로 인과 관계를 가지므로 성인에 서 기관지 천식의 중요한 원인의 하나로서 위식도역류질환 을 제시하고 있다.30 특히 위식도역류와 호흡기 증상에 대해 서는 위내용물의 식도로의 역류로 인해 천식 증상이 악화되 거나 입원할 위험성이 커지며 고용량의 약물치료가 필요한 경우가 증가할 수 있다.31,32 하지만 위식도역류에 의한 기관 지 천식 환자에서 가슴쓰림이나 산 역류와 같은 전형적인 위식도역류질환의 증상을 가지지 않은 경우가 많고 내시경 검사에서도 하부 식도에 이상 소견이 없는 경우가 대부분이 므로, 실제 임상에서 관련성을 파악하는 데에 어려움이 있 다.
기관지 천식 환자에서 흉곽 내 압력 상승과 반가로막의 교정(hemidiaphragm rectification) 등의 생리적인 변화가 일어 나면, 그 결과 항역류 장벽을 약화시켜 역류가 유발된다.30 이러한 역류는 다음과 같은 두 가지 기전을 통해서 천식을 야기하게 된다. 첫째는 위 내용물의 미세흡인에 인해 호흡 상피가 지속적인 자극을 받고 여러 염증 매개체들이 분비됨 으로써 기관지 수축과 최대호기유량(peak expiratory flow)의 감소가 발생한다는 것이다.33 두 번째 기전으로는 미주미주 신경 반사(vasovagal reflex)에 의한 기전으로, 기관기관지 나 무(tracheobronchial tree)와 식도가 동일하게 미주신경을 통 해 자율신경계 신경분포를 받을 뿐만 아니라, 두 장기 모두 태생학적으로 동일하게 앞창자(foregut)에서 유래한다는 사 실에 근거를 두고 있다.34,35 즉, 하부 식도에 산 노출이 되면 산에 민감한 수용체가 자극되어 반사 작용을 통해 기관지 수축이 발생한다는 것이다.
2) 만성 기침
만성 기침은 보고자에 따라 차이가 있지만 기침이 적어도 8주 이상 지속되는 경우를 말하며,36 위식도역류, 후비루 (postnasal drip), 기침 이형 천식이 만성 기침의 40% 정도에 서 원인이 되고 있다.37 일반적으로 위식도역류는 기침 이형 천식과 후비루에 이어 만성 기침의 세 번째로 가장 흔한 원 인이다.38 이러한 세 질환에 의한 만성 기침에서 증상의 특 징, 증상 발생 시간 및 합병증의 정도에서는 차이가 없다고 알려져 있다.39
위식도역류에 의한 기침은 주로 낮에 서 있는 자세에서
72 The Korean Journal of Gastroenterology: Vol. 52, No. 2, 2008
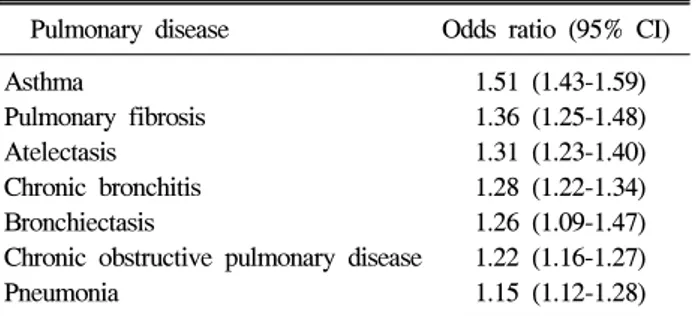
Table 3. Associations of Erosive Esophagitis and Pulmonary Disease (el-Serag HB et al.42)
Pulmonary disease Odds ratio (95% CI) Asthma 1.51 (1.43-1.59) Pulmonary fibrosis 1.36 (1.25-1.48) Atelectasis 1.31 (1.23-1.40) Chronic bronchitis 1.28 (1.22-1.34) Bronchiectasis 1.26 (1.09-1.47) Chronic obstructive pulmonary disease 1.22 (1.16-1.27) Pneumonia 1.15 (1.12-1.28) CI, confidence interval.
발생하는 것으로 알려져 있지만, 일부 환자들은 밤에 증상 이 발생하기도 한다.40 마른 기침 혹은 다량의 점액질 가래 를 동반하기도 하며, 환자의 40-75%는 가슴쓰림이나 산 역 류와 같은 전형적인 증상을 가지지 않는다.30 많은 환자에서 쉰 목소리, 후두통, 발성장애(dysphonia)가 동반될 수 있다.
다른 원인의 만성 기침 자체에 의해서도 위식도역류가 유발 될 수 있으므로(cough-reflux cycle), 다른 진단이 붙은 환자 에서도 위식도역류는 기침을 악화시키는 인자로 작용할 수 있다.
서구의 경우 만성 기침의 원인 중 10-40%에서 위식도역류 가 원인이며,31 ProGERD 연구에 의하면 나이 증가, 역류 식 도염, 과체중이 기침과 유의한 관계가 있다.3
위식도 역류가 기침을 유발하는 기전은 첫째로, 역류물이 후두에 도달하거나 기도로 직접 흡입되어 후두나 기도의 기 침 수용체를 직접 자극하거나 미주신경을 통하여 하부 호흡 기의 점액분비를 촉진시킴으로써 기관이나 기관지의 기침 수용체를 자극할 수 있다.40 두 번째로 역류된 위산에 의하 여 윈위부 식도의 점막하 수용체가 자극되어 기침이 유발된 다는 식도 -기관지 기침 반사(esophago-tracheobronchial cough reflex)가 있으며 이 기전이 가장 중요한 원인으로 생각되고 있다.38
3) 특발 폐섬유증
특발 폐섬유증과 위식도역류질환과의 연관이 일부 연구 에서 제시되고 있다. 원인을 알 수 없는 폐섬유증 환자 48명 을 대상으로 식도, 위, 십이지장의 방사선학 검사를 시행한 연구에서 이들 환자의 많은 수가 틈새탈장(hiatal hernia)이나 병적인 위식도 역류를 보였으며,41 조직검사에서 특발 폐섬 유증으로 확진된 17명의 환자에서 두 채널 pH 검사를 시행 했을 때 94%에서 병적인 위식도역류가 관찰되었고 전형적 인 위식도역류질환의 증상을 보인 환자는 25%에 불과하 다.19 이러한 결과들은 특발 폐섬유증 환자의 일부에서 위식 도역류가 원인으로 작용하며 이에 대한 치료가 폐질환의 자 연 경과를 변화시킬 가능성을 시사하는 것으로 이에 대한 연구가 필요한 실정이다.
4) 기타 호흡기 증상
역류 식도염과 폐렴, 기관지 확장증, 만성폐쇄성폐질환 (chronic obstructive pulmonary disease)과의 연관성이 보고되 고 있지만(Table 3),42 이에 대해서는 좀더 많은 연구가 필요 하리라 생각된다.
3. 이비인후과 증상
일반적으로 위식도역류질환을 가진 환자의 25% 정도가 이비인후과적인 이상 소견이나 증상을 가지는 것으로 알려
져 있으며, 정확한 역류 후두염의 유병률은 알 수 없지만 이 비인후과에 방문하는 환자의 약 4-10% 정도에서 위식도역 류질환과 관련된 증상과 징후를 보인다고 알려져 있다.43 많은 이비인후과 질환들이 위식도역류질환과 관련이 있 지만, 가장 현저한 소견은 후두염이다.44 위식도역류질환과 관련된 후두염은 후부 후두염(posterior laryngitis), 산 후두염 (acid laryngitis), 소화 후두염(peptic laryngitis), 그리고 최근에 는 역류 후두염(reflux laryngitis) 등으로 다양하게 불려지고 있다.
위식도역류질환과 관련된 증상들 중에서 쉰 목소리가 가 장 흔한 증상으로 역류 후두염 환자의 92%이상에서 발생하 고, 다른 증상들로는 인두구, 잦은 목 청소, 삼킴 통증, 목소 리 변화 등이 있다.45
기타 위식도역류에 의한 이비인후과 질환으로는 성대 결 절, 성대 및 피골 내벽 부종, 접촉성 궤양 및 육아종, 후두 연화증 (laryngomalacia), 성대문 연축, 후두 협착, 부비동염 등이 있다.
위식도역류가 이비인후과 증상을 유발하는 기전을 살펴 보면, 해부학적으로 후두와 근위부 식도는 근접해 있으므로 펩신과 담즙산의 후두부로의 역류로 인한 직접적인 자극으 로 후두 조직의 염증반응을 일으켜 증상을 유발한다는 기전 과 하부 식도의 위산역류가 미주신경을 매개로 한 반사작용 을 일으켜 증상을 유발한다는 기전이 있다.8 특히 밤에 간헐 적으로 발생하는 식도-인두 역류(intermittent nocturnal esopha- geal-pharyngeal reflux)가 가장 중요한 인자로 생각된다.11 후 두의 점막은 정상적으로 위산과 접촉되지 않으며 타액에 의 하여 중화될 수 없으므로 역류된 위내용물에 대한 방어 기 전이 매우 약하다. 밤에는 상부식도괄약근의 압력이 낮에 비하여 낮으며 기침과 타액분비와 같은 다른 방어기전도 약 해지므로 위 내용물의 인후로의 역류와 이에 의한 부종이나 염증과 같은 손상이 쉽게 일어날 수 있다.38
Kim GH. Extraesophageal Manifestations of Gastroesophageal Reflux Disease 73
Fig. 2. Dental erosions (arrow) found during the dental examina- tion (A, Gandara BK et al.47) and routine endoscopic examination (B) in the patients with gastro- esophageal reflux disease.
4. 치아 미란
이전부터 치아 미란과 위식도역류질환과의 연관성에 대 해서는 보고가 되어 왔으나, 2006년 위식도역류질환의 Mon- treal 정의와 분류에 ‘치아 미란 증후군(dental erosion synd- rome)'이라는 용어가 사용됨으로써 최근에 관심이 증가되고 있다.
치아 미란은 세균에 의하지 않고 화학적인 반응의 결과로 치아의 구조에 비가역적인 손상이 오는 것으로 정의한
다.46,47 치아 미란의 내재적인 원인으로서는 폭식증(bulimia),
되새김 증후군(rumination syndrome), 알코올 중독으로 인한 무증상 역류, 구강건조증(xerostomia), 위식도역류질환 등이 있다.48 일반인에서 치아 미란의 빈도는 2-18%인데 비해, 위 식도역류질환을 가진 환자에서 치아 미란의 빈도는 17- 68%이며, 치아 미란이 있는 환자에서 위식도역류질환의 빈 도는 25-83%로 보고되고 있다.49 따라서 위식도 역류가 치아 미란의 중요한 원인의 하나로 제시되고 있다. 이러한 치아 미란은 하악 어금니(mandibular molar) 부위에서 가장 흔히 관찰되며, 내시경 검사 중에도 자세히 관찰해보면 발견할 수 있다(Fig. 2).
식도 외 증상 환자에서의 진단적인 접근
1. 비심인 흉통
흉통 환자가 내원 시 가장 먼저 이루어져야 하는 것은 심 인 흉통과 비심인 흉통을 구분하는 것이다. 이를 위해서 임 상에서는 흔히 흉통의 양상에 대한 병력 청취와 ‘nitrogly- cerin test'를 시행하게 된다. 일단 여러 가지 심장에 대한 검 사로 심인 흉통의 가능성이 배제가 되었다면, 통증의 양상 에 대한 병력 청취와 신체검진을 통해서 흉통을 유발할 수 있는 상부 위장관 질환, 담관 질환, 흉벽 질환 및 폐 질환을 배제해야 한다.
내시경 검사는 위식도 역류에 의한 비심인 흉통 환자에서 미란 식도염이나 바렛 식도를 보이는 비율이 10% 미만으로 알려져23 비용-효과적인 측면에서 유용하지 않지만 삼킴 곤 란이나 삼킴 통증과 같은 경고 증상이 있는 경우는 위내시 경 검사가 선행되어야 한다. 24시간 pH 검사는 비심인 흉통 환자에서 증상 지수(symptom index)를 통해 위식도역류와의 연관성을 진단할 수 있을 것으로 생각되었으나, 검사 중에 흉통이 기록되는 경우가 적고 검사에 대한 환자의 인지 부 족 등의 제한점이 있고50 고가이면서 침습적인 검사법으로 널리 사용하는 데에는 한계가 있다. 최근에는 비심인 흉통환 자에서 고용량의 양자펌프 억제제(proton pump inhibitor, PPI) 를 단기간 투여하는 PPI 검사가 69-95%의 민감도와 67-86%
의 특이도를 보이며, 무엇보다도 방법이 간단하고 부작용이 거의 없다는 점에서, 또한 비용-효과적인 면에서 가장 유용 한 방법으로 알려져 있다.51,52
2. 호흡기 증상
위식도 역류와의 연관성을 진단하기 위한 간단한 방법은 없다. 호흡기 증상을 나타내는 환자에서 항생제, 항히스타 민제, 그 외에 약물요법에도 불구하고 증상의 호전이 없을 때 위식도역류와의 연관성을 고려해 보아야 한다.
1) 기관지 천식
임상적으로 위식도역류와 관련된 기관지 천식을 의심할 수 있는 경우는 (1) 성인에서 시작된 천식, (2) 천식의 가족 력이 없는 경우, (3) 천식이 있기 전에 역류 증상이 선행된 경우, (4) 식후에 쌕쌕거림(wheezing)이 심해질 때, (5) 야간 에 기침이나 쌕쌕거림이 있을 때, (6) theophylline이나 beta2- 길항제에 의해 악화되는 천식이 있는 경우이다.
위산 역류로 유발된 천식을 진단하는 첫 번째 단계로는 경험적인 PPI 검사를 시행한다. 이 검사는 간단하며 합병증 이 적고, 침습적이지 않으며 많은 연구에서 높은 민감도와 특이도를 보였다.53-55 O'Connor 등은 천식의 유발이나 악화
74 대한소화기학회지: 제52권 제2호, 2008
Table 4. Reflux Finding Score for Identifying Laryngopharyn- geal Reflux (Belafsky PC et al.62)
Reflux scoring scale Subglottic edema 0 - absent
2 - present Ventricular obliteration 2 - partial
4 - complete Erythema/hyperemia 2 - arythenoids only
4 - diffuse Vocal fold edema 1 - mild
2 - moderate 3 - severe 4 - polypoid Diffuse laryngeal edema 1 - mild
2 - moderate 3 - severe 4 - obstructing Posterior commissure hypertrophy 1 - mild
2 - moderate 3 - severe 4 - obstructing Granuloma/granulation tissue 0 - absent
2 - present Thick endolaryngeal mucus 0 - absent
2 - present
Fig. 3. Findings of reflux lar- yngitis during routine endoscopic examination in the patients with gastroesophageal reflux disease.
의 원인이 위식도역류라고 진단하는데 3개월간 매일 ome- prazole 20 mg을 사용하는 PPI 검사가 가장 비용-효과면에서 우수하다고 보고하였다.56 위산억제 치료에도 불구하고 증 상이 지속될 때에는 다른 질병을 감별하기 위해서 24시간 pH 검사를 시행한다. 내시경 검사에서 하부 식도의 이상 소 견이 없는 경우가 대부분이지만 삼킴 곤란, 빈혈, 체중감소 또는 출혈 등의 경고 증상이 있을 때에는 내시경 검사를 시 행해야 한다.57
진단 시 주의할 점은 위식도역류와 연관된 천식환자에의 쌕쌕거림 증상은 하부 식도로의 위산 역류와는 연관이 없고 상부 식도로의 위산역류와 연관이 있어서,58 반드시 두 개 이상의 pH 전극을 가진 24시간 pH 검사를 하는 것이 바람 직하다.
2) 만성 기침
만성 기침을 보이는 환자는 우선 흉부 X-ray를 검사하고 자세한 병력을 청취하여 안지오텐신전환효소(angiotensin con- verting enzyme) 억제제나 흡연에 의한 원인을 제외하여야 한다. 내시경 검사는 만성 기침 환자에서 대부분 정상 소견 을 보이므로 거의 도움이 되지 않는다. 고용량의 PPI 검사 는 비교적 저렴하고 간단한 진단법으로 가장 우선적으로 시 행한다. 이후 산 억제 치료에 반응이 없는 환자에서는 24시 간 pH 검사가 추천되는 검사법이다. 하지만 정확한 인과 관 계를 밝히기 어렵고 비산성 역류를 감지할 수 없다는 단점 이 있다. 24시간 pH 검사에서 역류와 증상의 시간적인 연관 성이 있고 위식도역류에 대한 치료로 기침이 호전된다면 가 장 정확한 진단이 된다. 상부식도괄약근 상부 2 cm에서 인 두부 pH를 측정하는 방법이 상부 기도에 도달하는 위산 역 류를 진단하는데 높은 정확도를 보이지만,59 이 검사법은 아 직까지 널리 사용되고 있지 않다. 최근에는 식도 내 임피던 스를 측정하는 방법이 시도되고 있는데, 이 방법은 24시간 pH를 동시에 측정할 수 있고, 산 역류와 비산역류를 구별할 수 있다. 또한 역류와 호흡기 증상의 시간적 연관성을 확인
할 수 있어 위산분비 억제제 치료의 효과를 예측하는 데 도 움이 된다.60
3. 이비인후과 증상
이비인후과 증상을 가진 환자에서는 먼저 초기 검사로 후 두경 검사를 시행해야 한다. 이때 후인두역류를 의심할 수 있는 후두경 소견은 발적, 후두부 후벽의 부종, 성대 결절 및 육아종, 성문하 협착 등이 있으며, 상부 내시경 검사 중 에도 비교적 쉽게 관찰할 수 있다(Fig. 3). 하지만 이러한 소 견들의 대부분은 비특이적인 징후로 흡연, 술, 후비루 등의 다른 원인에 의해서도 관찰될 수 있고 관찰자 간의 일치율
김광하. 위식도역류질환의 식도외 증상 75
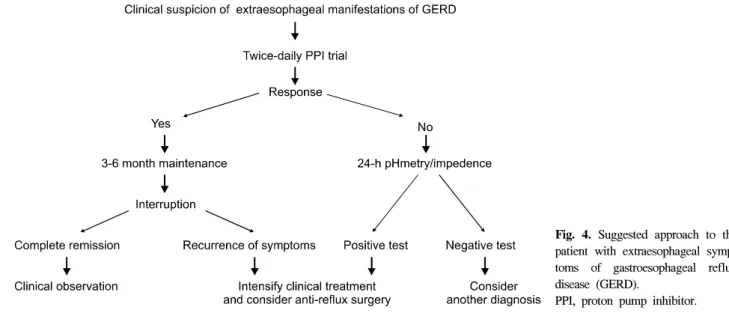
Fig. 4. Suggested approach to the patient with extraesophageal symp- toms of gastroesophageal reflux disease (GERD).
PPI, proton pump inhibitor.
도 낮은 것으로 알려져 있다.61 한 연구에서는 역류점수척도 (reflux scoring scale)를 이용하여 점수가 7 이상인 경우에 후 두의 염증이 후인두역류로 인한 것을 나타낸다고 보고하였 다(Table 4).62 역류 후두염으로 추정되는 환자에서 위식도역 류의 존재를 확인하기 위한 가장 유용한 검사는 24시간 pH 검사이다. 그러나 증상과 후두경 소견과의 일치율이 낮아서 진단적인 유용성은 낮은 것으로 보고되고 있다.61 정상 24시 간 pH 검사 결과를 보인 역류 후두염 환자의 23%에서 후두 부에 전극을 추가하여 검사하였을 때 식도-인두 역류가 관 찰된다는 보고가 있어,44 현재로서는 인두 pH 검사(pharyn- geal pH monitoring)가 후두 질환이 있는 환자에서 위식도역 류와의 인과 관계를 밝히는데 가장 좋은 방법이다.63 고용량 의 PPI 검사의 유용성에 대해서는 아직 이견이 있는 상태 로, 한 전향 연구에서는 PPI 검사 후 63%의 환자에서 후두 증상의 호전을 보였다고 하나 통계적인 유의성은 없었다고 보고하고 있다.64 이는 비특이적인 후두 징후에 대해 과도하 게 역류성 후두염으로 진단내렸을 가능성과 함께, 후두 증 상을 보이는 경우 여러 원인들이 복합되어 있는 경우가 많 아 PPI 검사를 시행 후 반응에 대한 효과적인 예측인자를 찾기 어렵다는 점 등을 고려할 수 있다.
치 료
위식도역류질환의 식도 외 증상을 가진 환자에서 산 억제 제 치료의 반응은 전형적인 식도증상을 가진 환자에 비해서 반응을 예측하기가 어렵다. 이는 여러 원인이 복합되어 식 도 외 증상이 발생하거나 위식도역류질환과 관련성이 있을 것으로 과대 진단되는 경우가 있기 때문이다. 또한 식도 외 증상을 보이는 환자에선 산 억제제 치료에 대한 반응은 서 서히 나타나고 미약하며 장기간 유지되지 못하는 경향이 있
다.38 최근 PPI 치료가 주를 이루고 있으며 증상 조절을 위 한 적절한 용량과 치료 기간을 정하기 위해서 많은 연구가 이루어지고 있다. 여러 연구들을 종합해 볼 때 식도 외 증상 을 가진 위식도역류질환의 치료는 전형적인 식도증상을 가 진 환자보다 고용량의 PPI를 장기간 투여하는 것이 효과적 일 것으로 보인다. 일반적으로 PPI를 고용량으로 하루 2회, 최소한 3개월간 사용하여 반응 여부를 판단할 것을 추천하 고 있다. 위식도역류를 억제하기 위한 수술 치료가 내과 치 료보다 더 우수한지에 대해서는 아직까지 명확하지 않지만, 적절한 내과 치료에 반응이 없는 일부 환자에서는 수술 치 료를 조심스럽게 적용할 필요성도 있다(Fig. 4).65
1. 비심인 흉통
24시간 pH 검사에서 이상 소견이 있는 비심인 흉통 환자 의 초기치료로서 생활습관 교정과 PPI 치료가 우선적으로 시행되고 있다. PPI 용량과 치료기간은 통일되어 있지 않으 나, 하루 1-2회의 용량으로 시작하고 증세의 호전이 없을 때 증량하는 방법을 추천한다.66
비심인 흉통환자에서 시행한 이중맹검실험에서 고용량의 PPI를 2달 이상 투약 후 장기간 유지요법을 시행하는 것이 효과적이며,67 Fang 등은 고용량 PPI의 경험적인 치료는 위산 역류와 연관된 흉통의 초기 진단과 치료에 가장 효과적인 방 법이라 보고하였다.24 실제로 최근에는 24시간 pH 검사를 시 행하기 어렵거나 전형적인 위식도역류질환의 증상을 가지고 있는 환자에서는 우선적으로 고용량의 PPI를 투약하여 진단 및 치료를 동시에 시행하는 방법이 이용되기도 한다.
2. 호흡기 증상
1) 기관지 천식
산 억제제 치료에 대한 효과는 여러 전향적인 연구에 잘
76 The Korean Journal of Gastroenterology: Vol. 52, No. 2, 2008
나타나 있다. Kiljander 등은 역류 식도염을 가진 천식환자에 서 고용량의 esomeprazole 치료로 페기능 검사와 야간의 호 흡기 증상이 유의하게 완화되었으며,68 Tsugeno 등은 rabeprazole 치료로 20% 이상의 환자에서 최고호기속도의 향상이 있었다고 보고하였다.69 또한 Litter 등도 중증 기관 지 천식 환자를 대상으로 한 전향 연구에서 lansoprazole 30 mg 1일 2회씩 24주간 투여한 군에서 증상의 호전뿐 아니라 천식 발작의 빈도가 감소하였다.70 수술 치료는 복강경하 위 저부주름술(laparoscopic fundoplication)이 주로 행해지는데, 적응증은 24시간 pH 검사에서 양성이고 50세 이하, 내과 치 료에 반응이 없거나, PPI 치료 후 4주 내에 재발한 경우, 그 리고 지속적인 PPI 치료가 요구되는 경우이다.30 수술 성적 은 417명의 환자를 대상으로 한 연구에서 역류 증상의 개선 이 90%, 천식 증상 호전이 79%, 기관지 확장제 사용의 감소 가 88%, 마지막으로 27%의 환자에서 폐기능이 호전되었 다.71
2) 만성 기침
24시간 pH 검사에서 비정상 소견이 있는 만성 기침 환자 의 초기치료로서 생활습관의 교정과 PPI 투여가 일반적으 로 이용된다. Ours 등은 omeprazole 40 mg을 1일 2회 투여하 는 고용량 PPI 요법으로 치료 시작 2주 만에 현저한 증상의 호전을 관찰하였다고 보고하였다.72 PPI 투여 후 증상 호전 의 기간은 환자에 따라 차이가 있으므로 반응 여부를 판단 하기까지 최소 3개월 정도는 치료를 지속할 것을 추천한다.
3개월 후에 부분적이라도 증상 호전이 있는 경우에는 추가 적으로 3개월간 투약기간을 연장해 보는 것이 좋다. 또한 약물 중단 후에 빈번한 재발이 일어나므로 PPI를 지속적으 로 사용할 것이 추천된다.
3. 이비인후과 증상
Belafsky 등은 역류 후두염 환자에서 2개월간의 PPI 치료 후에 증상의 호전은 있으나 국소적인 소견의 호전은 증상의 호전보다 느리게 나타나므로 국소적인 소견이 완전히 좋아 질 때까지, 또는 최소 6개월 이상의 PPI 치료가 필요하다고 주장하였다.73 후인두역류의 치료에서 표준화된 PPI 용량과 치료기간은 확립되어 있지 않으며, 많은 환자에서 약물 중 단 시에 빈번히 재발한다. 그러므로 3-6개월간의 지속적인 치료와 정기적인 추적 관찰이 필요하다.74 대개 6개월간의 생활 양식의 변화와 PPI (1일 2회)를 사용하고, 이후 6개월 간 증상이 없으면 약물 용량을 감량하는 것을 제안하고 있 다.75 일부 연구에서는 수술 치료가 역류 후두염을 가진 환 자의 대부분에서 효과적이며,76 복강경하 Nissen 위저부주름 술을 시행 후 70% 이상의 환자에서 이비인후과 증상의 호 전을 보였다.77 수술 성공을 예측할 수 있는 인자로는 PPI에
잘 반응하고 24시간 pH 검사에서 하인두로의 역류가 확인 된 환자, 식도운동능이 보존된 환자 등이다.78,79
결 론
위식도역류질환의 식도 외 증상은 다양하게 나타날 수 있 으며, 가슴쓰림이나 산 역류와 같은 전형적인 증상을 호소 하지 않는 경우가 많아 이에 대한 주의와 관심이 없다면 임 상적으로 진단하기가 쉽지 않다. 비심인 흉통, 만성 기침과 같은 호흡기 증상, 쉰 목소리, 인두구와 같은 이비인후과 증 상 등의 여러 임상 상황에서 다른 원인이 없을 때 위식도역 류질환의 가능성을 고려하여 적극적인 진단과 치료를 할 필 요가 있다. 진단 방법으로는 내시경 검사, 24시간 pH 검사, PPI 검사 등을 주로 이용하는데, 이전에는 24시간 pH 검사 가 우선적으로 추천되지만 최근에는 간단하고 부작용이 적 은 PPI 검사가 많이 이용되고 있다. 치료로 전형적인 위식 도역류질환의 환자에 비해서 고용량과 장기간의 PPI 투여 가 추천되지만, 정확한 용량과 치료 기간이 아직 확립되어 있지 않아 이에 대해서는 좀더 많은 연구가 필요하리라 생 각한다.
참고문헌
1. Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal re- flux disease: a global evidence-based consensus. Am J Gas- troenterol 2006;101:1900-1920.
2. Locke GR 3rd, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ 3rd. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minne- sota. Gastroenterology 1997;112:1448-1456.
3. Jaspersen D, Kulig M, Labenz J, et al. Prevalence of ex- tra-oesophageal manifestations in gastro-oesophageal reflux disease: an analysis based on the ProGERD Study. Aliment Pharmacol Ther 2003;17:1515-1520.
4. Lee SH, Choi MG, Park SH, et al. The clinical spectrum of gastroesophagel reflux disease in Korea. Korean J Gastroint- est Motil 2000;6:1-10.
5. Irwin RS, Curley FJ, French CL. Chronic cough. The spec- trum and frequency of causes, key components of the diag- nostic evaluation, and outcome of specific therapy. Am Rev Respir Dis 1990;141:640-647.
6. McNally PR, Maydonovitch CL, Prosek RA, Collette RP, Wong RK. Evaluation of gastroesophageal reflux as a cause of idiopathic hoarseness. Dig Dis Sci 1989;34:1900-1904.
7. Chevalier JM, Brossard E, Monnier P. Globus sensation and
Kim GH. Extraesophageal Manifestations of Gastroesophageal Reflux Disease 77
gastroesophageal reflux. Eur Arch Otorhinolaryngol 2003;260:
273-276.
8. Tauber S, Gross M, Issing WJ. Association of laryngophar- yngeal symptoms with gastroesophageal reflux disease. Lary- ngoscope 2002;112:879-886.
9. Jacob P, Kahrilas PJ, Herzon G. Proximal esophageal pH-me- try in patients with ‘reflux laryngitis'. Gastroenterology 1991;
100:305-310.
10. Kuhn J, Toohill RJ, Ulualp SO, et al. Pharyngeal acid reflux events in patients with vocal cord nodules. Laryngoscope 1998;108:1146-1149.
11. Koufman JA. The otolaryngologic manifestations of gastro- esophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope 1991;101:
1-78.
12. Ylitalo R, Ramel S. Gastroesophagopharyngeal reflux in pa- tients with contact granuloma: a prospective controlled study.
Ann Otol Rhinol Laryngol 2002;111:178-183.
13. DiBaise JK, Olusola BF, Huerter JV, Quigley EM. Role of GERD in chronic resistant sinusitis: a prospective, open label, pilot trial. Am J Gastroenterol 2002;97:843-850.
14. Schroeder PL, Filler SJ, Ramirez B, Lazarchik DA, Vaezi MF, Richter JE. Dental erosion and acid reflux disease. Ann Intern Med 1995;122:809-815.
15. Ward PH, Hanson DG. Reflux as an etiological factor of car- cinoma of the laryngopharynx. Laryngoscope 1988;98:1195- 1199.
16. Loughlin CJ, Koufman JA. Paroxysmal laryngospasm secon- dary to gastroesophageal reflux. Laryngoscope 1996;106:1502- 1505.
17. Toohill RJ, Ulualp SO, Shaker R. Evaluation of gastro- esophageal reflux in patients with laryngotracheal stenosis.
Ann Otol Rhinol Laryngol 1998;107:1010-1014.
18. Mays EE. Intrinsic asthma in adults. Association with gastro- esophageal reflux. JAMA 1976;236:2626-2628.
19. Tobin RW, Pope CE 2nd, Pellegrini CA, Emond MJ, Sillery J, Raghu G. Increased prevalence of gastroesophageal reflux in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 1998;158:1804-1808.
20. Gislason T, Janson C, Vermeire P, et al. Respiratory symp- toms and nocturnal gastroesophageal reflux: a population- based study of young adults in three European countries.
Chest 2002;121:158-163.
21. Napierkowski J, Wong RK. Extraesophageal manifestations of GERD. Am J Med Sci 2003;326:285-299.
22. Bortolotti M, Pandolfo N, Miglioli M. Abnormal esoph- agocardiac reflex in patients with non-cardiac chest pain. Dis Esophagus 2001;14:57-59.
23. Fass R, Navarro-Rodriguez T. Noncardiac chest pain. J Clin Gastroenterol 2008;42:636-646.
24. Fang J, Bjorkman D. A critical approach to noncardiac chest pain: pathophysiology, diagnosis, and treatment. Am J Gastro- enterol 2001;96:958-968.
25. Hewson EG, Sinclair JW, Dalton CB, Richter JE. Twenty- four-hour esophageal pH monitoring: the most useful test for evaluating noncardiac chest pain. Am J Med 1991;90:576- 583.
26. Singh S, Richter JE, Hewson EG, Sinclair JW, Hackshaw BT.
The contribution of gastroesophageal reflux to chest pain in patients with coronary artery disease. Ann Intern Med 1992;
117:824-830.
27. Schofield PM, Bennett DH, Whorwell PJ, et al. Exertional gastro-oesophageal reflux: a mechanism for symptoms in pa- tients with angina pectoris and normal coronary angiograms.
Br Med J (Clin Res Ed) 1987;294:1459-1461.
28. Balaban DH, Yamamoto Y, Liu J, et al. Sustained esophageal contraction: a marker of esophageal chest pain identified by intraluminal ultrasonography. Gastroenterology 1999;116:29- 37.
29. Sontag SJ, O'Connell S, Khandelwal S, et al. Most asth- matics have gastroesophageal reflux with or without broncho- dilator therapy. Gastroenterology 1990;99:613-620.
30. Gurski RR, da Rosa AR, do Valle E, de Borba MA, Valiati AA. Extraesophageal manifestations of gastroesophageal re- flux disease. J Bras Pneumol 2006;32:150-160.
31. Harding SM, Richter JE. The role of gastroesophageal reflux in chronic cough and asthma. Chest 1997;111:1389-1402.
32. Harding SM, Guzzo MR, Richter JE. 24-h esophageal pH testing in asthmatics: respiratory symptom correlation with esophageal acid events. Chest 1999;115:654-659.
33. Koufman JA, Belafsky PC, Bach KK, Daniel E, Postma GN.
Prevalence of esophagitis in patients with pH-documented lar- yngopharyngeal reflux. Laryngoscope 2002;112:1606-1609.
34. Mansfield LE. Gastroesophageal reflux and asthma. Postgrad Med 1989;86:265-269.
35. Fass R, Achem SR, Harding S, Mittal RK, Quigley EM.
Review article: supra-oesophageal manifestations of gastro- oesophageal reflux disease and the role of night-time gastro- oesophageal reflux. Aliment Pharmacol Ther 2004;20(suppl 9):26-38.
36. Palombini BC, Villanova CA, Araujo E, et al. A pathogenic triad in chronic cough: asthma, postnasal drip syndrome, and
78 대한소화기학회지: 제52권 제2호, 2008
gastroesophageal reflux disease. Chest 1999;116:279-284.
37. Fontana GA, Pistolesi M. Cough. 3: chronic cough and gas- tro-oesophageal reflux. Thorax 2003;58:1092-1095.
38. Fennerty MB. Extraesophageal gastroesophageal reflux disease.
Presentations and approach to treatment. Gastroenterol Clin North Am 1999;28:861-873, vi.
39. Mello CJ, Irwin RS, Curley FJ. Predictive values of the char- acter, timing, and complications of chronic cough in diagnos- ing its cause. Arch Intern Med 1996;156:997-1003.
40. Irwin RS, Richter JE. Gastroesophageal reflux and chronic cough. Am J Gastroenterol 2000;95:S9-14.
41. Mays EE, Dubois JJ, Hamilton GB. Pulmonary fibrosis asso- ciated with tracheobronchial aspiration. A study of the fre- quency of hiatal hernia and gastroesophageal reflux in inter- stitial pulmonary fibrosis of obscure etiology. Chest 1976;69:
512-515.
42. el-Serag HB, Sonnenberg A. Comorbid occurrence of lar- yngeal or pulmonary disease with esophagitis in United States military veterans. Gastroenterology 1997;113:755-760.
43. Tutuian R, Castell DO. Diagnosis of laryngopharyngeal reflux. Curr Opin Otolaryngol Head Neck Surg 2004;12:
174-179.
44. Wong RK, Hanson DG, Waring PJ, Shaw G. ENT manifes- tations of gastroesophageal reflux. Am J Gastroenterol 2000;
95:S15-22.
45. Toohill RJ, Kuhn JC. Role of refluxed acid in pathogenesis of laryngeal disorders. Am J Med 1997;103:100S-106S.
46. Eccles JD, Jenkins WG. Dental erosion and diet. J Dent 1974;2:153-159.
47. Gandara BK, Truelove EL. Diagnosis and management of dental erosion. J Contemp Dent Pract 1999;1:16-23.
48. Barron RP, Carmichael RP, Marcon MA, Sandor GK. Dental erosion in gastroesophageal reflux disease. J Can Dent Assoc 2003;69:84-89.
49. Lazarchik DA, Filler SJ. Dental erosion: predominant oral le- sion in gastroesophageal reflux disease. Am J Gastroenterol 2000;95:S33-38.
50. Dekel R, Martinez-Hawthorne SD, Guillen RJ, Fass R.
Evaluation of symptom index in identifying gastroesophageal reflux disease-related noncardiac chest pain. J Clin Gastroen- terol 2004;38:24-29.
51. Pandak WM, Arezo S, Everett S, et al. Short course of ome- prazole: a better first diagnostic approach to noncardiac chest pain than endoscopy, manometry, or 24-hour esophageal pH monitoring. J Clin Gastroenterol 2002;35:307-314.
52. Bautista J, Fullerton H, Briseno M, Cui H, Fass R. The effect of an empirical trial of high-dose lansoprazole on symptom
response of patients with non-cardiac chest pain--a random- ized, double-blind, placebo-controlled, crossover trial. Aliment Pharmacol Ther 2004;19:1123-1130.
53. Fass R, Ofman JJ, Gralnek IM, et al. Clinical and economic assessment of the omeprazole test in patients with symptoms suggestive of gastroesophageal reflux disease. Arch Intern Med 1999;159:2161-2168.
54. Juul-Hansen P, Rydning A, Jacobsen CD, Hansen T. High- dose proton-pump inhibitors as a diagnostic test of gas- tro-oesophageal reflux disease in endoscopic-negative patients.
Scand J Gastroenterol 2001;36:806-810.
55. Bate CM, Riley SA, Chapman RW, Durnin AT, Taylor MD.
Evaluation of omeprazole as a cost-effective diagnostic test for gastro-oesophageal reflux disease. Aliment Pharmacol Ther 1999;13:59-66.
56. O'Connor JF, Singer ME, Richter JE. The cost-effectiveness of strategies to assess gastroesophageal reflux as an ex- acerbating factor in asthma. Am J Gastroenterol 1999;94:
1472-1480.
57. Moraes-Filho J, Cecconello I, Gama-Rodrigues J, et al.
Brazilian consensus on gastroesophageal reflux disease: pro- posals for assessment, classification, and management. Am J Gastroenterol 2002;97:241-248.
58. Patti MG, Debas HT, Pellegrini CA. Esophageal manometry and 24-hour pH monitoring in the diagnosis of pulmonary as- piration secondary to gastroesophageal reflux. Am J Surg 1992;163:401-406.
59. Eubanks TR, Omelanczuk P, Hillel A, Maronian N, Pope CE, Pellegrini CA. Pharyngeal pH measurements in patients with respiratory symptoms before and during proton pump in- hibitor therapy. Am J Surg 2001;181:466-470.
60. Sifrim D, Dupont L, Blondeau K, Zhang X, Tack J, Janssens J. Weakly acidic reflux in patients with chronic unexplained cough during 24 hour pressure, pH, and impedance moni- toring. Gut 2005;54:449-454.
61. Noordzij JP, Khidr A, Desper E, Meek RB, Reibel JF, Levine PA. Correlation of pH probe-measured laryngophar- yngeal reflux with symptoms and signs of reflux laryngitis.
Laryngoscope 2002;112:2192-2195.
62. Belafsky PC, Postma GN, Koufman JA. The validity and reli- ability of the reflux finding score (RFS). Laryngoscope 2001;111:1313-1317.
63. Koufman JA, Aviv JE, Casiano RR, Shaw GY. Laryngophar- yngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology-Head and Neck Surgery. Otolaryngol Head Neck Surg 2002;127:32-35.
김광하. 위식도역류질환의 식도외 증상 79
64. Williams RB, Szczesniak MM, Maclean JC, Brake HM, Cole IE, Cook IJ. Predictors of outcome in an open label, ther- apeutic trial of high-dose omeprazole in laryngitis. Am J Gastroenterol 2004;99:777-785.
65. DeVault KR. Overview of therapy for the extraesophageal manifestations of gastroesophageal reflux disease. Am J Gastroenterol 2000;95:S39-44.
66. Katz PO. Approach to the patient with unexplained chest pain. Semin Gastrointest Dis 2001;12:38-45.
67. Achem SR, Kolts BE, MacMath T, et al. Effects of omepra- zole versus placebo in treatment of noncardiac chest pain and gastroesophageal reflux. Dig Dis Sci 1997;42:2138-2145.
68. Kiljander TO, Harding SM, Field SK, et al. Effects of esome- prazole 40 mg twice daily on asthma: a randomized place- bo-controlled trial. Am J Respir Crit Care Med 2006;173:
1091-1097.
69. Tsugeno H, Mizuno M, Fujiki S, et al. A proton-pump in- hibitor, rabeprazole, improves ventilatory function in patients with asthma associated with gastroesophageal reflux. Scand J Gastroenterol 2003;38:456-461.
70. Littner MR, Leung FW, Ballard ED 2nd, Huang B, Samra NK. Effects of 24 weeks of lansoprazole therapy on asthma symptoms, exacerbations, quality of life, and pulmonary func- tion in adult asthmatic patients with acid reflux symptoms.
Chest 2005;128:1128-1135.
71. Field SK, Gelfand GA, McFadden SD. The effects of antire- flux surgery on asthmatics with gastroesophageal reflux.
Chest 1999;116:766-774.
72. Ours TM, Kavuru MS, Schilz RJ, Richter JE. A prospective evaluation of esophageal testing and a double-blind, random- ized study of omeprazole in a diagnostic and therapeutic al- gorithm for chronic cough. Am J Gastroenterol 1999;94:3131- 3138.
73. Belafsky PC, Postma GN, Koufman JA. Laryngopharyngeal reflux symptoms improve before changes in physical findings.
Laryngoscope 2001;111:979-981.
74. Issing WJ, Karkos PD. Atypical manifestations of gas- tro-oesophageal reflux. J R Soc Med 2003;96:477-480.
75. Halstead LA. Extraesophageal manifestations of GERD: diag- nosis and therapy. Drugs Today (Barc) 2005;41(suppl B):19- 26.
76. Waring JP, Lacayo L, Hunter J, Katz E, Suwak B. Chronic cough and hoarseness in patients with severe gastroesophageal reflux disease. Diagnosis and response to therapy. Dig Dis Sci 1995;40:1093-1097.
77. Westcott CJ, Hopkins MB, Bach K, Postma GN, Belafsky PC, Koufman JA. Fundoplication for laryngopharyngeal reflux disease. J Am Coll Surg 2004;199:23-30.
78. Allen CJ, Anvari M. Preoperative symptom evaluation and esophageal acid infusion predict response to laparoscopic Nissen fundoplication in gastroesophageal reflux patients who present with cough. Surg Endosc 2002;16:1037-1041.
79. So JB, Zeitels SM, Rattner DW. Outcomes of atypical symp- toms attributed to gastroesophageal reflux treated by laparo- scopic fundoplication. Surgery 1998;124:28-32.