INTRODUCTION
Subscapularis of the shoulder is an integral structure that maintains stable anterior posture [1]. If damaged, it is usually accompanied by a tear of the rotator cuff [2-4].
According to literature, subscapularis tear is less common than the supraspinatus/infraspinatus tear that make up around 5% of all rotator cuff tears [5-7], but in fact subscapularis tear has been detected concomitantly in around 19% of arthroscopic repair events of rotator cuff tears [8]. However, no particular indications are found during physical examination that suggests tears in the upper subscapularis, making them difficult to detect and
diagnose [9]. Recently, improved diagnostic tools and arthroscopic techniques have led to increase in reports of subscapularis tears and their successful treatments.
Further, many clinical studies of arthroscopic repairs of subscapularis tears have been published [10,11].
However, conservative management of subscapularis tears if in combination with supraspinatus/infraspinatus tears has not been reported of yet. The authors here report of 12-month follow-up studies on patients who underwent arthroscopic repair of rotator cuff tears whilst the tear in the upper subscapularis (Pfirrmann class I) was conservatively managed.
Background: The aim of this study was to identify the clinical outcomes after conservative management of partial tears of the upper subscapularis tendon (Pfirrmann class I) in patients who underwent arthroscopic repair of rotator cuff tears.
Methods: Of the two hundred and eighty-one patients who underwent arthroscopic rotator cuff repair at our institution between January 2005 and August 2011, fifty-six patients had a subscapularis tendon tear. And among them, twenty- three patients who could be followed up until at least 12 months after operation were evaluated retrospectively. Repair of the subscapularis tendon partial tear was not performed in all patients. We evaluated the range of motion (ROM) of shoulder, muscle power, Korean shoulder scoring system (KSS), American Shoulder and Elbow (ASES) scores, and the visual analog scale (VAS).
Results: At 12-months follow-up, range of forward elevation was improved to 148.5o, range of external rotation to 55.4o, and range of internal rotation to the 11th thoracic level. Further, abduction strength was improved to 13.9 kg, external rotation strength to 16.4 kg, and internal rotation strength to 18.4 kg. KSS was improved from 53.0 to 89.4, ASES from 48.4 to 86.6, and VAS from 8.3 to 1.6. There were significant improvements in terms of ROM of shoulder, muscle power, KSS, ASES scores, and VAS (P < 0.05).
Conclusion: Clinical improvement was achieved in patients with arthroscopic repair of rotator cuff tears at a short- term follow-up of 12 months when the partial tear in the upper subscapularis tendon (Pfirrrmann class I) that came concomitantly was conservatively managed.
Keywords: Rotator cuff tear; Partial tear of upper subscapularis; Arthroscopic rotator cuff repair; Conservative management
Clinical outcome after arthroscopic repair of rotator cuff tears without repair of partial tear of upper subscapularis
Joong-Bae Seo, Jong-Pil Kim, Jee-Won Ryu
Department of Orthopedic Surgery, Dankook University College of Medicine, Cheonan, Korea
Copyright © 2014 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
AOSM
Received August 8, 2013; Revised October 22, 2013; Accepted October 23, 2013
Correspondence to: Joong-Bae Seo, Department of Orthopedic Surgery, Dankook University College of Medicine, 119 Dandae-ro, Dongnam-gu, Cheonan 330-997, Korea. Tel: +82-41-550-3950, Fax: +82-41-556-3238, E-mail: [email protected]
METHODS
Subjects of study
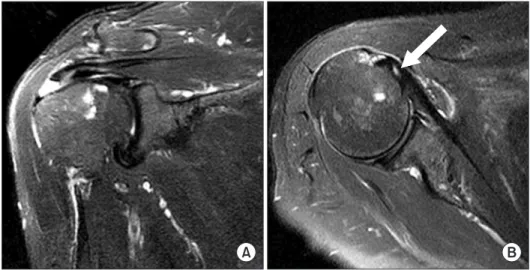
Of the total 281 rotator cuff arthroscopic repairs perfor- med between January 2005 and August 2011, 56 patients had a combined subscapularis tendon tear. Of these, a conservative management approach was taken if the tear resided in the upper subscapularis tendon (Pfirrmann class I), and the patients were willing to take part in a short-term 12-month follow-up study. A total of 23 patients were recruited. Preoperative magnetic resonance imaging (MRI) was performed to detect those with subscapularis tendon tears within the upper third region of the tendon, and only those classified in this Pfirrmann class I-type subscapularis tear were included in the study (Figs. 1, 2) [12]. Others, whose MRI results showed either Pfirrmann class II- or III-type subscapularis tears,
exhibited re-tears of massive rotator cuff tears, or either had underwent a previous open rotator cuff repairs or showed articular defect or nerve injury were excluded in the study. Of the 23 patients who underwent conservative management of the upper subscapularis tendon tear, 15 were men, and 8 were women. The mean age at surgical intervention was 57.0 years (range, 43 to 67 years), and the average follow-up period was 14.2 months (range, 12 to 24 months).
Treatment and rehabilitation
All surgical intervention was performed under general anesthesia and the patient was positioned into a beach- chair pose. The extremities were placed in an abduction and external rotation position, and the articular lesion was confirmed arthroscopically. The rotator cuff tears were repaired arthroscopically as described in our previous
Fig. 1. Magnetic resonance image of a patient who showed combined partial tear of the upper subscapularis. (A) Coronal image shows medium-sized full thickness rotator cuff tear. (B) The arrow indicates upper portion of the partial tear of subscapularis (Pfirrmann class I).
Fig. 2. Arthroscopic findings of patients who exhibited a combined partial tear of the upper subscapularis. (A) After double row rotator cuff repair. (B) Posterior viewing portal shows tear of the upper portion of subscapularis. The subscapularis was not repaired. (C) Another patient’s arthroscopic finding shows longitudinal split tear of the upper portion of subscapularis.
report, but the tear in the upper subscapularis tendon was left untreated (Fig. 2). The patient began pendulum motion exercises 2 days postoperation, and manually operated pulleys and other similar joint rehabilitation equipment from 4-5 days postoperation. Further, an abduction brace at 30o was used for support for 6 weeks after the operation, and thereafter, active joint exercises and muscle-building activities were permitted.
Data analysis and interpretation methods
After arthroscopic repair of the rotator cuff tear, follow- up studies were conducted at 6 weeks, 3 months, and every 3 months subsequently. And at every 3 months postoperation, various muscle strength tests, indicators to measure range of motion (ROM) of shoulder, and questi- onnaires were taken. Muscle strength testing equipment (Myometer, Mecmesin Co., Nottingham, UK) was used to measure the external rotation, internal rotation, and abduction strengths. The external rotation strength was measured by placing the upper arms next to the thoracic, and then measuring the force required to move the upper arms away from the trunk whilst the elbow is bent. The internal rotation strength was measured in a similar manner, but the upper arms pulled towards the trunk. The abduction strength was measurable by determining the force required to raise the upper arm towards the coronal plane (in line with the subscapularis) from when the elbow is extended next to the thoracic.
The ROMs of shoulder assessed were forward flexion and external rotation of the shoulder and internal rotation was indicated by the level of the vertebral body. Clinical outcomes were also analyzed by observing the Korean shoulder scoring system (KSS), American Shoulder and Elbow Surgeons (ASES) scores, and the visual analogue scale (VAS) of pain.
Statistical analysis
To test whether a statistically significant difference exists between the clinical outcomes before and after the surgery, a paired t-test was implemented using the preoperative, 3-month postoperative, and 12-month postoperative values of ROM of shoulder, ASES, KSS, and VAS. A difference was deemed significant if P < 0.05 (SPSS ver. 19.0, SPSS Inc., Chicago, IL, USA).
RESULTS
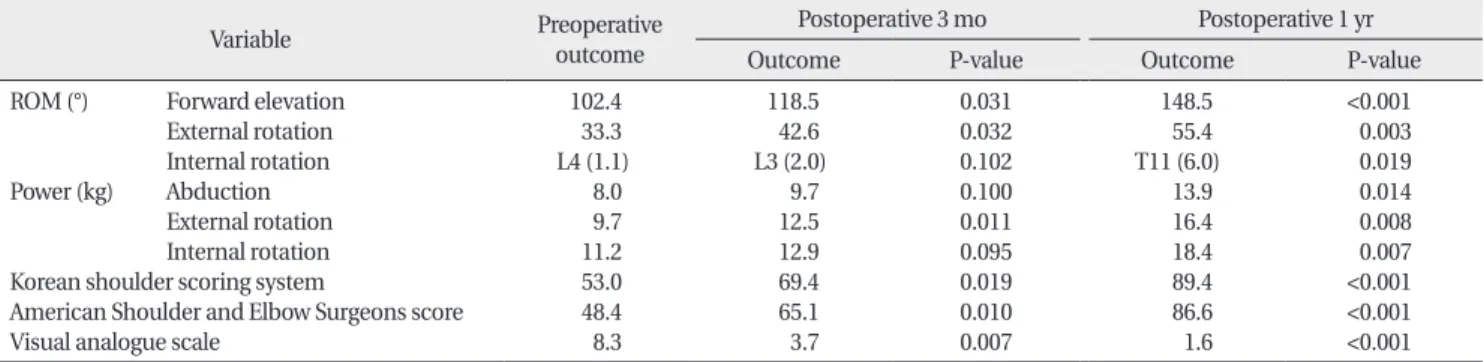
The respective mean values for the ROM of shoulder, for which the indicators assessed were the range of forward elevation, external rotation, and internal rotation, improved over time. At preoperation, these values were 102.4o, 33.3o, and 4th lumbar chord, respectively. At 3-month postoperation, they improved to 118.5o, 42.6o, and 3rd lumbar chord, respectively. At the final follow-up at 12-month postoperation, the values enhanced to 148.5o, 55.4o, and 11th thoracic level. Further, muscle power was also monitored in patients at the same time points.
Preoperative abduction strength was 8.0 kg, external rotation strength was 9.7 kg, and internal rotation strength was 11.2 kg. Three months later, these values improved to 9.7 kg, 12.5 kg, and 12.9 kg, respectively. At 12 months, this was 13.9 kg, 16.4 kg, and 18.4 kg, respectively. Likewise, improvements were seen in other clinical parameters.
KSS improved from 53 to 69.4, and then to 89.4 during the same follow-up periods. ASES improved from 48.4 to 65.1, and then to 86.6, respectively. VAS regarding pain level was 8.3 preoperatively, 3.7 3-month postoperatively, and 1.6 12-month postoperatively. The clinical improvements seen before surgery and at a short-term follow-up at 12 months postoperation for the ROM of shoulder, muscle strength, KSS, ASES scores, and VAS were shown to be statistically significant (P < 0.05) (Table 1).
Table 1. Functional outcomes and P-values of combined partial tear of upper subscapularis
Variable Preoperative
outcome
Postoperative 3 mo Postoperative 1 yr
Outcome P-value Outcome P-value
ROM (°) Forward elevation External rotation Internal rotation Power (kg) Abduction
External rotation Internal rotation Korean shoulder scoring system
American Shoulder and Elbow Surgeons score Visual analogue scale
102.4 33.3 L4 (1.1)
8.0 9.7 11.2 53.0 48.4 8.3
118.5 42.6 L3 (2.0)
9.7 12.5 12.9 69.4 65.1 3.7
0.031 0.032 0.102 0.100 0.011 0.095 0.019 0.010 0.007
148.5 55.4 T11 (6.0)
13.9 16.4 18.4 89.4 86.6 1.6
<0.001 0.003 0.019 0.014 0.008 0.007
<0.001
<0.001
<0.001 ROM, range of motion.
Range of internal rotation, abdominal strength, and internal rotation strength was shown to have a clinically significant improvement from the preoperative stage and at 12-month follow-up. However, when the final follow-up value was compared with the value marked at 3-month follow-up, the difference was no longer statistically significant (P > 0.05). Additionally, the gradation on the probe was used to measure the length of the rotator cuff tear using the length of the damaged tendon after arthroscopic debridement as a standard. The tear was classified according to their length, where below 3 cm was classified as a small, medium tear, and above 3 cm was a large, massive tear. In total, 18 small, medium tears and 5 large, massive tears were assessed (Table 2).
DISCUSSION
Rotator cuff plays an important role in the stability of the shoulder articular joint [1,13]. Equally, subscapularis tendon is involved in maintaining the anterior shoulder stability as well as the stabilizing the humeral head within the glenoid. Thus, in case of subcapularis insufficiency, anterior subluxation of the humeral head may occur [14]. The frequency of subscapularis tendon tear is around 3.5%-27.4%, varying drastically between different literature, and in most cases comes in combination with rotator cuff tears rather than in isolation [5,15,16].
Subscapularis tears associated with supraspinatus/
infraspinatus tears usually occur as a result of the degenerative changes that started initially at the anterior supraspinatus of the rotator cuff tendons. Not only can this spread into the infraspinatus tendon of the rotator cuff, but also the subscapularis tendon and the long head of biceps brachii. Recently, Pfirrmann et al. [12] reported that in 21 cases of subscapularis tears, 76% of these tears elongated to massive rotator cuff tears, demonstrating a strong association.
Preoperative diagnosis of subscapularis tears is unco- mmon. Tung et al. [17] reported that preoperative detection and diagnosis of a subscapularis tear is 31%
by MRI, and that the tear, which tends to reside in the upper region of the subscapularis, may be mistaken for
a continuous tear due to scar tissue. Thus it is important not only to diagnosis after sagittal image analysis but also the axial image [17,18]. Diagnostic approaches to subscapularis tears include, lift-off test, internal rotation lag sign test, Napoleon sign, and abdominal compression tests. Napoleon sign, which is a modified abdominal compression test, has been shown a sensitive diagnostic tool for when there is a defect in or pain due to internal rotation of the shoulder joint [19]. Electromyographic studies on subscapularis tendon by Tokish et al. [20]
showed that upon abdominal compression, the upper subscapularis region becomes stimulated, whereas the lower portion becomes stimulated by the lift-off test.
However, tears localized to the upper portion of the subscapularis is difficult to detect by physical examination alone, and sensitivity of bear-hug and abdominal compression tests to detect the tears have been shown to reach only around 40%-60% [9]. In order to test the patient’s prognosis after conservative management of the upper subscapularis tear, we implemented the abdominal compression test, and positive results came back for 2 cases preoperatively (8.7%), 1 case 3-month postoperation (4.3%), and none at 12-months postoperation. A negative abdominal compression test for all cases at 12-month postoperation, despite the fact that the subscapularis tear was left untreated, may likely be due to false positive results. This may have occurred as a result of limited internal rotation ability of the shoulder, which was not present before surgical intervention.
The fact that the tears are predominantly localized in the upper subscapularis tendon, that they begin and extend from that region, and that preoperative detection of such tears is difficult highlights the importance of increasing the awareness of these tears during an arthroscopic examination. Increase of such efforts, together with availability of improved diagnostic tools and arthroscopic techniques have raised the number of reported subsca- pularis tears in the literature [10,11]. Especially, detection of the subscapularis tears have increased during arthro- scopic repair of rotator cuff tears, which is recently be- coming a standardized procedure and many clinical studies have been conducted to repair subscapularis tears.
Ticker and Burkhard [1] have suggested that in occasions where rotator cuff tears are associated with subscapularis tears, reparation of the subscarpularis tear prior to the repair of rotator cuff tears allows easier reparation due to the lateral movement of supraspinatus/infraspinatus.
On the other hand, if the rotator cuff tears are repaired Table 2. Proportion by cuff tear size of combined partial tear of upper
subscapularis
Tear size (cm) No. of cases (%) Small to medium tear (<3)
Large to massive tear (>3)
18 (78.3) 5 (21.7)
without repairing the subscapularis tears, more tension is placed on the supraspinatus leading to possible re-tear.
However, arthroscopic intervention of the subscapularis is known to be difficult as edema and the resulting effusion may hinder a successful reparation and additionally, establishing enough space for a posterior portal for the arthroscopy guide to pass is difficult [4,11,21,22]. Thus, the authors undertook a conservative management in terms of the subscapularis tear (Pfirrmann class I) whilst repairing the associated rotator cuff tear and report of a significant benefit in terms of clinical outcome when assessed at a short-term 12-month follow-up.
The purpose of our study was to define whether there was a meaningful clinical benefit if tears in the upper subscapularis tendon (Pfirrmannn class I) are con- servatively managed, whilst the associated supraspinatus/
infraspinatus tears are treated arthroscopically. A controlled study comparing the clinical outcomes of the arthroscopic repair of rotator cuff tears of two groups of patients, either treated or not treated of a common upper subscapularis tear would have been ideal. Other limitations include using a few and crude parameters to check clinical outcomes of patients. Further, postoperative
checks were not implemented to observe the status of the upper subscapularis tear either by MRI or ultrasound, but such limitations to this current study may be overcome by addressing these issues in a long-term study. Thus, this short-term 12-month follow-up study should be extended to see the long-term effects of this procedure, and confirm our clinical finding. Despite such limitations to the study, our report describes one of the first observations of conservative management of subscapularis tears with clinically significant improvements.
In conclusion, a clinical improvement of statistical significance was found at a short-term 12-month follow- up after rotator cuff supraspinatus/infraspinatus tears was arthroscopically repaired whilst the concomitant tears in the upper subscapularis tendon (Pfirrmann class I) was conserved. However, a long-term follow-up study is required to gain further clinical outcomes to consolidate our results.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Ticker JB, Burkhart SS. Why repair the subscapularis? A logical rationale. Arthroscopy 2011;27:1123-8.
2. Kreuz PC, Remiger A, Lahm A, Herget G, Gachter A. Comparison of total and partial traumatic tears of the subscapularis tendon. J Bone Joint Surg Br 2005;87:348-51.
3. Bennett WF. Arthroscopic repair of anterosuperior (supra- spinatus/subscapularis) rotator cuff tears: a prospective cohort with 2- to 4-year follow-up. Classification of biceps subluxation/
instability. Arthroscopy 2003;19:21-33.
4. Burkhart SS, Tehrany AM. Arthroscopic subscapularis tendon repair: technique and preliminary results. Arthroscopy 2002;18:
454-63.
5. Flury MP, John M, Goldhahn J, Schwyzer HK, Simmen BR. Rupture of the subscapularis tendon (isolated or in combination with supra spinatus tear): when is a repair indicated? J Shoulder Elbow Surg 2006;15:659-64.
6. Warner JJ, Higgins L, Parsons IM 4th, Dowdy P. Diagnosis and treatment of anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2001;10:37-46.
7. Biondi J, Bear TF. Isolated rupture of the subscapularis tendon in an arm wrestler. Orthopedics 1988;11:647-9.
8. Kim TK, Rauh PB, McFarland EG. Partial tears of the subsca- pularis tendon found during arthroscopic procedures on the shoulder: a statistical analysis of sixty cases. Am J Sports Med
2003;31:744-50.
9. Barth JR, Burkhart SS, De Beer JF. The bear-hug test: a new and sensitive test for diagnosing a subscapularis tear. Arthroscopy 2006;22:1076-84.
10. Foad A, Wijdicks CA. The accuracy of magnetic resonance imaging and magnetic resonance arthrogram versus arthroscopy in the diagnosis of subscapularis tendon injury. Arthroscopy 2012;28:636-41.
11. Choi CH. Subcoracoid lesion. J Korean Arthroscopy Soc 2009;13:
126-31.
12. Pfirrmann CW, Zanetti M, Weishaupt D, Gerber C, Hodler J. Sub- scapularis tendon tears: detection and grading at MR arthro- graphy. Radiology 1999;213:709-14.
13. Inman VT, Saunders JB, Abbott LC. Observations of the function of the shoulder joint: 1944. Clin Orthop Relat Res 1996;330:3- 12.
14. Ticker JB, Warner JJ. Single-tendon tears of the rotator cuff:
evaluation and treatment of subscapularis tears and principles of treatment for supraspinatus tears. Orthop Clin North Am 1997;28:99-116.
15. Arai R, Sugaya H, Mochizuki T, Nimura A, Moriishi J, Akita K. Sub- scapularis tendon tear: an anatomic and clinical investigation.
Arthroscopy 2008;24:997-1004.
16. Bennett WF. Subscapularis, medial, and lateral head coraco-
REFERENCES
humeral ligament insertion anatomy: arthroscopic appearance and incidence of “hidden” rotator interval lesions. Arthroscopy 2001;17:173-80.
17. Tung GA, Yoo DC, Levine SM, Brody JM, Green A. Subscapularis tendon tear: primary and associated signs on MRI. J Comput Assist Tomogr 2001;25:417-24.
18. Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF.
Traumatic tears of the subscapularis tendon: clinical diagnosis, magnetic resonance imaging findings, and operative treatment.
Am J Sports Med 1997;25:13-22.
19. Kim DH, Moon YL, Kim KJ. Partial tear of upper portion of
subscapularis. J Korean Shoulder Elbow Soc 2005;8:9-13.
20. Tokish JM, Decker MJ, Ellis HB, Torry MR, Hawkins RJ. The belly- press test for the physical examination of the subscapularis muscle: electromyographic validation and comparison to the lift- off test. J Shoulder Elbow Surg 2003;12:427-30.
21. Burkhart SS, Brady PC. Arthroscopic subscapularis repair:
surgical tips and pearls A to Z. Arthroscopy 2006;22:1014-27.
22. Choi CH, Kim SK, Chang IW, Kim SS. Subclavian portal approach for isolated subscapularis tendon tear: technical note. J Korean Shoulder Elbow Soc 2009;12:221-5.