VOLUME 12, NUMBER 2, June 2007
Clinical Results of Two Operative Treat- ments in Mallet Fracture
Seung-Yong Lee, M.D., Yoon-Suk Hyun, M.D.
Department of Orthopedic Surgery, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
Purpose: To investigate clinical results of Open reduction and internal fixation with K-wire and modified extension-block K-wire fixation in treatment of Mallet fracture.
Materials and Methods: From March 2000 to December 2006, thiry-one patients(group A) treated by ORIF with K-wire fixation and twenty-four patients (group B) treated by modified extension-block K-wire fixation were included. Using Wehbe and Schneider’s classification 7 type I B, 24 type II B fractures were in group A and 4 type I B, 20 type II B were in group B.
Between two groups postoperative range of motion of distal interphalangeal joint, bony union time, operative time were compared by Chi-square test and functional results were graded by Crawford’s criteria.
Results: There were no statistical difference in postop- erative clinical data and results according to Crawford’s criteria except operative time. In group A, 2 temporary skin problems and 5 tenderness on skin incision were noticed and more operative time was taken.
Conclusion: According to clinical results except pos- sibilities of complications and differences in operation
time, two operative techniques are considered as good treatments in Mallet fracture.
Key Words: Distal interphalangeal joint, Mallet fracture, ORIF with K-wire fixation, Modified extension-block K-wire fixation
서 론
추지 골절은 수지의 원위지골의 기저부 중 수지 신 전근의 부착 부위에서 생긴 견열 골절이다1. 골절편의 크기가 작은 경우 부목 고정 등에 의한 비수술적 방법 만으로도 만족할 만한 결과를 얻을 수 있으나2-5, 골절 편이 관절면의 1/3 이상을 차지하거나 원위지골의 아 탈구가 있는 경우에는 수술적 치료를 해야 한다3,6-9. 보 존적 치료와 수술적 치료와의 비교는 보고된 바 있으 나 수술 방법을 서로 비교한 보고는 많지 않다3,12,13. 따라서 저자는 수술법 중 비교적 널리 이용되는 두 가 지 방법의 임상적 결과를 비교하여 추후 수술적 방법 을 선택함에 있어 도움이 되고자 하였다.
연구 대상 및 방법
1. 대상
2000년 3월부터 2006년 12월까지 본원에서 추지 골절(골성 추지 변형)로 수술적 치료를 받은 환자 121 명의 환자 중 관혈적 정복 및 K-강선 고정술로 치료 받은 31명(A군)과 변형된 신전 차단 K-강선 고정술 로 치료받은 24명(B군)을 대상으로 하였다. 추시 기 간은 6개월 이상인 환자만 대상으로 하였으며 A군에 서는 평균 33.74주(표준 편차±6.56)였고 환자군 B에 서는 평균 33.66주(표준 편차±7.60)였다. A군에서 남자가 24명, 여자가 7명, 평균 연령은 31.4세(표준 편차±9.5세)이고 B군에서는 남자가 19명, 여자가 5
추
추지 지 골 골절 절에 에서 서 두 두 가 가지 지 수 수술 술적 적 치 치료 료의 의 임 임상 상 결 결과 과
한림대학교 의과대학 강동성심병원 정형외과학교실 이승용∙현윤석
통신저자: 현현 윤윤 석석
서울특별시 강동구 길동 445
한림대학교 의과대학 강동성심병원 정형외과학교실 TEL: 02-2224-2850, FAX: 02-489-4391 E-mail: ys7933@naver.com
명, 평균 연령이 33.3세(표준 편차±10.6세)였다.
2. 수술까지의 시간 및 골절의 분류
수술까지의 시간은 A군에서 평균 11일 B군에서 평 균 10.9일이었고 골절의 분류는 Wehbe and Schneider5 분류법(Table 1)을 사용하였다.
3. 수술 적응증 및 수술 방법
수술의 적응증으로는 골절편이 관절면의 30% 이상 을 차지하거나 원위지골의 전방 아탈구가 동반된 경우 로 하였다. A군의 경우 앙와위에서 상완총 신경 마취 를 시행한 후 원위지간 관절의 배측에 T 또는 S자 절 개를 한 후 신전건의 종지부에 손상이 가지 않도록 조 심하면서 골절부를 노출시켰다. 골절부의 혈종을 제거 한 뒤 골편과 원위지골의 배측 피질을 기준으로 해부 학적 정복을 한 다음 0.9 mm 또는 1 mm의 K-강선 으로 골편과 원위지골을 고정한다. 그리고 이동 투시 영상 장치로 보면서 원위 지관절이 중립위 상태에서 1.2 mm나 1.6 mm의 K-강선으로 원위지간 관절을
관통하여 고정하였다(Fig. 1). 수술 후 약 6주간 부목 으로 원위지간 관절을 중립위로 고정한 후 6주째 K- 강선을 제거한 뒤 2주간은 수동적 신전 운동만 시행하 였고 그 후 서서히 수동적 및 능동적 굴곡 운동을 시 행하였다. B군의 경우에는 마취를 시행한 뒤 이동 영 상 투시 장치 하에서 원위지간 관절을 최대한 굴곡한 다음 골절편의 크기에 따라 1 mm나 1.2 mm의 K- 강선을 피부와 신전건을 관통시켜 중위지골 관절면에 삽입하였다. K-강선의 삽입 각도는 측면 방사선 사진 상 중위지와 약 40~45도 정도의 각을 이루게 하였다.
그 후 원위지골을 잡고 최대한 수지의 장축으로 견인 및 신전하면서 골편을 정복시켰다. 이동 영상 투시 장 치로 확인하여 도수 정복으로 정복이 만족스러운 경우 에는 원위지간 관절을 중립위나 약간 신전위로 유지한 채 1.2 mm나 1.6 mm K-강선으로 원위지간 관절을 고정하였다(Fig. 2).
4. 결과의 판정
결과의 판정은 Crawford2 판정법을 사용하였다 (Table 2). 결과를 분석함에 있어 원위지간 관절 정
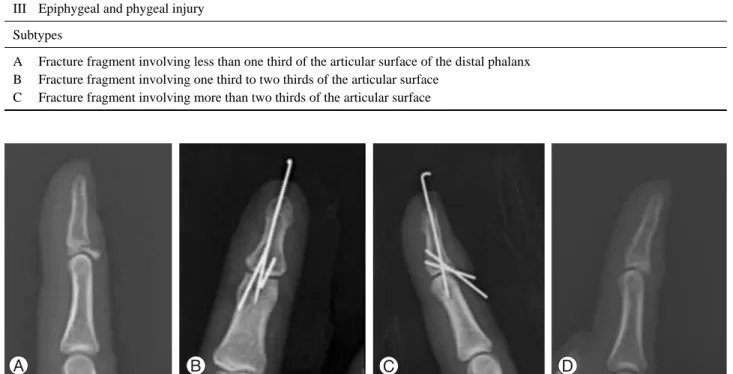
Fig. 1. A 18 year old female patient had bony mallet finger injury. (A) The initial lateral X-ray showed a displaced dorsal fragment and articular involvement more than 30% without subluxation. (B, C) Open reduction and K-wire fixation was performed. (D) Postoperative 6 months, the fractured bone was united and the patient had a range of motion from 0 to 65 degrees.
Table 1. Wehbe and schneider’s classification
Type
I Fracture include bone injuries of varying extent without suluxation of the distal interphalangeal joint II Fracture are associated with subluxation of the distal interphalangeal joint
III Epiphygeal and phygeal injury Subtypes
A Fracture fragment involving less than one third of the articular surface of the distal phalanx B Fracture fragment involving one third to two thirds of the articular surface
C Fracture fragment involving more than two thirds of the articular surface
상 굴곡 범위에 대한 의문이 들었지만 원위지간 관절 의 정상 운동 범위에 관한 보고서가 많지 않았다.
Moiemen과 Elliot14은 40명의 지원자에서 8개 수지 의 원위 지관절의 정상 운동 범위를 분석한 결과 남자 는 69�, 여자는 79�였고 성별에 차이없이 평균 74�였 다. 그러나 저자는 사람마다 최대 능동 굴곡 범위는 다를 것이라고 생각하여 건측 수지에서 근위지간 관절 을 완전 신전위로 한 상태에서 원위지간 관절의 최대 능동 굴곡을 기준으로 하였다. 그리고 두 환자군간의 성별, 연령, 골절 양상, 수상 후 수술까지의 시간, 골 유합에 소요된 시간, 추시 기간, 수술 시간을 조사하 여(Table 3, 4) Chi-square 검정을 이용하여 비교하 였고 SPSS version 12.0을 이용하였으며 유의성의 판정은 p-value가 0.05 미만으로 하였다(Table 5).
그 외 추시 기간 동안 발생한 합병증이나 후유증도 조 사하였다.
결 과
A군에서는 Wehbe and Schneider 분류법상 ⅠB 가 7예, ⅡB가 24예였고, B군에서는ⅠB가 4예, ⅡB 가 20예였고 두 환자군 간에 골절 양상, 성별 및 연령 분포, 수술까지의 소요 시간, 추시 기간 등에 통계학 적으로 유의한 차이는 없었다(p>0.05). 신전 소실과
후속 굴곡 정도, 골유합 기간, 골절 양상, Crawford 판정법 등에서도 두 환자군 간에 통계학적으로 유의한 차이는 없었다(Table 5). Crawford 판정법 결과를 통계 처리함에 있어 Chi-square 검정과 T-test 모두 시행하였다. 결과가 exellent와 good 밖에 없어서 Chi-square 검정은 두 그룹으로 나누어 시행하였고 T-test는 exellent는 4점 good은 3점으로 변환하여 처리하였으나 두 검정법 모두에서 통계학적으로 유의 한 차이를 보이지 않았다(p>0.05). 합병증으로는 A군 에서 피부 절개선 주변에서 한시적인 피부의 허혈성 변화 2예가 발생하였으나 별 후유증을 남기지 않고 해 결이 되었고 5예에서는 수술 절개선 부위에 경미한 압 통이 발견되었으나 환자가 불편해 하지 않았고 기능상 문제를 유발시키지 않아 통계 처리를 이용한 비교 대 상에 포함시키지 않았다. 수술 시간의 비교에서는 A 군에서 더 많은 시간이 소요되는 것을 알 수 있었다 (p=0.00)(Table 5).
고 찰
추지 골절은 신전건이 원위지절 부위에서 그 연속성 이 끊어지면서 발생하는데 주로 신전건이 원위지골에 부착하는 부위에서 견열 골절의 형태로 나타나며 결과 적으로 원위지절의 신전 지연을 초래한다15. 추지는 신
Table 2. Crawford classification
Classification Extension Loss Flexion Pain
Exellent None Full None
Good 0�to 10� Full None
Fair 10�to 25� Any loss of flexion None
Poor > 25� Any loss of flexion Persistent pain
Fig. 2. A 17 year old male patient had bony mallet finger injury. (A) The initial lateral X-ray showed a displaced dorsal fragment and articular involvement more than 30% without subluxation. (B, C) Modified extension- block K-wire fixation was performed.
(D) Postoperative 6 months, the fractured bone was united and the patient had a range of motion from 0 to 65 degrees.
전건이 긴장된 상태에서 원위지 관절의 갑작스런 굴곡 으로 발생할 수 있으며 이때는 신전건 자체에 파열이 발생하던지 혹은 작은 골편을 가지며, 외관상 추지 변 형이 심하게 나타난다. 과신전력에 의한 추지에서는 일 반적으로 중위지 골두에 의한 압박력과 전단력으로 골 절이 생기며, 골편의 크기가 크고 굴곡건과 후방 지지 의 소실로 인해 원위지골의 전방 아탈구를 동반하게 된 다. 후방 골막에 의한 연결이 남아있기 때문에 추지 변 형이 심하지 않고 어느 정도의 신전이 가능하다16. 골 성 추지의 치료방법으로 크게 보존적 치료와 수술적 치 료로 나눌 수 있으나 각각의 적응증과 결과 및 합병증 에 대해 아직도 논란이 많다. Wehbe와 Schneider5 는 골절편의 크기가 큰 경우에도 보존적 치료로 좋은
결과를 얻을 수 있고 수술적 치료가 보존적 치료에 대 해 특별한 장점이 없다고 하였으며 추시상 관찰 가능 한 원위지절 배측의 돌출은 치료 방법에 상관없이 관 찰 가능하며 재형성에 의해 교정이 가능하다고 하였고 단순 방사선 검사 추시에서 발견되는 윈위지절의 퇴행 성 변화는 수지의 기능 및 통증과 관련이 없다고 하였 다. Kalainov 등17에 의하면 골절편이 관절면의 30%
이상 차지하거나 원위지골의 수장부 아탈구가 있는 환 자에서도 보존적 치료로 만족할 만한 결과를 얻을 수 있었고 수상 후 4주 이상이 지난 경우에도 좋은 결과 를 얻었다고 하였다. 그러나 일반적으로 골절편이 작 거나(관절면의 30% 이하) 원위지절의 수장부 아탈구 가 없으면 보존적 치료만으로 만족할 만한 결과를 얻
Table 3. Summary of Group A cases
Age Sex Finger E*(�) F�(�) Class� Crawford� TO‖ F/U¶ U** OT��
(day) (week) (week) (minute)
36 M 5 0 65 2b Exellent 05 32 08 40
29 F 5 0 60 2b Exellent 07 28 10 30
50 M 5 5 65 2b Good 14 24 12 30
45 F 2 0 60 1b Exellent 05 32 08 50
36 M 2 100 65 2b Good 03 28 10 20
20 M 5 0 65 2b Exellent 14 40 14 30
30 M 2 0 65 2b Exellent 08 24 10 40
45 M 5 5 60 1b Good 21 36 10 50
22 F 4 0 65 2b Exellent 10 28 08 30
18 F 4 0 65 1b Exellent 03 24 08 25
29 M 3 0 65 2b Exellent 07 46 12 45
24 M 5 0 65 2b Exellent 13 32 10 30
25 M 5 0 60 2b Exellent 12 40 08 50
27 M 5 0 65 1b Exellent 14 32 10 40
39 M 5 0 60 2b Exellent 21 24 08 20
26 M 3 0 65 1b Exellent 17 48 10 25
48 M 5 5 60 2b Good 28 32 12 35
38 M 5 0 65 2b Exellent 05 28 08 40
19 M 4 0 70 1b Exellent 07 28 10 45
47 F 4 5 65 2b Good 25 36 08 50
18 M 4 0 65 2b Exellent 06 36 06 40
39 M 5 0 60 2b Exellent 43 48 10 30
32 M 4 0 60 2b Exellent 07 32 10 50
19 F 5 0 65 1b Exellent 03 36 08 40
39 M 5 5 65 2b Good 013 40 10 35
30 M 4 0 70 2b Exellent 04 40 08 40
27 M 2 0 65 2b Exellent 05 36 08 40
24 M 5 0 65 2b Exellent 07 24 10 30
33 M 5 0 65 2b Exellent 06 40 08 25
35 M 4 0 60 2b Exellent 05 24 10 20
23 F 2 0 65 2b Exellent 04 48 10 25
Average 11.03 19.61 9.41 35.48
*E, extension lag; �F, further flexion; �Class, Wehbe and Schneider’s classification; �Crawford, results according to Crawford’s cri- teria; ‖TO, Duration Between trauma day and operation day; ¶F/U, follow-up duration; **U, bony union time; ��OT, Operation time
을 수 있다고 여겨지고 있으며 반면에 골절편이 관절 면의 30% 이상을 차지하거나 원위지절의 수장부 아탈 구가 동반된 경우에는 아직 논란의 여지는 있으나 수 술적 치료가 필요하다는 주장이 더 많다3-6,10,18-21
. Lubahn13은 수술적 치료와 비수술적 치료를 비교한 결과 수술적 방법이 미용적으로나 기능적으로 비수술 적 방법보다 더 좋은 결과를 얻었다고 하였다. 그 외 에도 골절편이 관절면의 30% 이상을 차지하거나 원위 지절의 수장부 아탈구가 동반된 경우 보존적 방법으로 치료할 경우 골절편의 해부학적 정복이 이루어지지 않 아 원위 지관절의 신전 소실이나 배측의 돌출, 그리고
퇴행성 관절염을 유발하여 통증과 운동 범위 제한을 유발할 수 있고 그 외에 오랜 고정에 따른 일상 생활 의 불편이나 피부 합병증 등도 일으킬 수 있다는 보고 들도 있다4,6,10,22,23
. 골성 추지의 해부학적 정복을 가능 케 하는 수술적 방법으로는 관혈적 방법으로 관혈적 정복 후 골절편의 K-강선 고정술4,7,21,24, 압박나사 고 정술, 골수강내 강선 고정술, 견인 철사 요법을 이용 한 고정술15,27, 8자형 긴장 강선을 이용한 고정술10,28, Pull-out 봉합술6 그리고 Pull-in 봉합술29, Hook 금 속판을 이용한 고정술30 등이 있고, 비관혈적 방법으로 변형된 신전 차단 K-강선 고정술1,20,32과 원위지간 관절
Table 4. Summary of Group B cases
Age Sex Finger E*(�) F�(�) Class� Crawford� TO‖ F/U¶ U** OT��
(day) (week) (week) (minute)
19 F 3 0 70 2b Exellent 6 36 08 15
42 M 5 5 60 2b Good 7 40 08 20
25 M 5 0 65 2b Exellent 120 40 10 20
36 M 5 0 70 1b Exellent 140 36 12 10
16 F 4 0 70 2b Exellent 6 36 10 05
34 M 3 5 65 2b Good 5 32 12 10
37 F 3 0 65 2b Exellent 3 40 08 15
43 M 5 0 60 2b Exellent 7 36 10 10
32 F 4 0 70 2b Exellent 120 24 08 10
17 M 4 0 65 2b Exellent 100 36 08 05
46 M 3 5 60 2b Good 5 24 12 10
27 M 5 0 65 1b Exellent 120 36 10 15
50 M 4 5 60 2b Good 210 24 10 20
22 F 2 0 70 2b Exellent 5 36 08 10
33 M 5 0 65 2b Exellent 6 36 10 10
39 M 4 0 60 2b Exellent 7 32 10 05
53 M 4 5 65 2b Good 5 40 10 15
22 M 4 0 65 1b Exellent 3 24 08 15
45 M 5 5 65 2b Good 7 24 12 10
34 M 4 0 65 2b Exellent 5 32 10 05
23 M 5 0 70 1b Exellent 6 44 12 10
27 M 4 0 65 2b Exellent 5 44 10 15
44 M 4 5 60 2b Good 600 32 12 30
34 M 5 0 65 2b Exellent 320 24 08 20
Average 10.8 20.75 9.83 13.33
*E, extension lag; �F, further flexion; �Class, Wehbe and Schneider’s classification; �Crawford, results according to Crawford’s cri- teria; ‖TO, Duration Between trauma day and operation day; ¶F/U, follow-up duration; **U, bony union time; ��OT, Operation time
Table 5. Summary of statistical data
Ext lag (�) Further Flex (�) Union time (week) Op. time (minutes)
Group A 1.12 63.8 9.09 35.4
Group B 1.45 65.0 9.83 13.3
p-value 0.618 0.197 0.191 0.00
Ext: Extension, Flex: Flexion, Op.: Operation
에 손상을 주지 않은 Umbrella Handle tech- nique31 등이 있다. 많은 수술 방법들 중 저자가 비교 한 2가지 방법에 대해서만 언급하기로 하겠다. 비교 대상이었던 관혈적 정복 후 골절편의 K-강선 고정술 과 변형된 신전 차단 K-강선 고정술은 이미 여러 연 구를 통해 좋은 결과들을 보고하고 있는 방법들이다
1,4,7,11,20,24,32,33
. 수술 명칭에서도 알 수 있듯이 변형된 신전 차단 K-강선 고정술은 초기 Ishiguro 등11이 제 안한 방법대로 원위지간 관절을 약간 굴곡된 상태로 고정하였더니 신전근의 끝 부분이 다소 당겨진 채로 고정되므로 약간의 신전 소실이 보고되어 후에 여러 연구자들에 의해 원위지간 관절을 중립 상태로 고정하 는 변형된 방법을 사용한다1,20,32. 아쉬운 점은 본 연구 에 사용된 두 가지 수술법에 대한 비교 연구가 없었던 관계로 과거 연구 결과들과의 비교가 어렵다는 것이었 다. 본 연구에서 사용된 관혈적 수술 방법에 관한 보 고를 살펴보면 수술 후 신전 소실이 2�에서 5�로 비교 적 양호한 결과를 보여주고 있다4,7,24. 본 연구의 경우 에서도 신전 소실이 평균 1.12�였다. 관혈적 치료의 합병증으로는 절개 부위 주변 피부 괴사, 굴곡 변형 재발, 강선 주위 감염, 조갑 변형 등이 보고되고 있으 며 발생률은 3%에서 53%까지 다양하게 보고되고 있 다3,18,27,34,35,37
. 본 연구에서는 관혈적 정복 및 K-강선 고정술을 시행한 환자 중에서 강선 주변 감염이 3예, 일시적인 절개 부위 피부의 허혈성 변화가 2예 있었으 나 별 후유증 없이 호전되었다. 변형된 신전 차단 K- 강선 고정술의 경우 만족할 만한 결과를 보고하면서도 한 편에선 신전 소실이 최대 20�까지 그리고 합병증 발생률은 5%에서 최대 60%까지 보고하고 있다
1,20,32,33
. 관혈적 방법이나 비관혈적 방법이나 신전 소실 의 정도에는 차이가 없다고 보고하고 있다1,11,20. 본 연 구에서도 신전 소실은 두 가지 방법에서 별 차이가 없 었으며 변형된 신전 차단 K-강선 고정술의 경우 합병 증이 발생하지 않았다. 수술 시간을 비교한 문헌 보고 는 이제까지 없었느나 저자가 비교해 본 바로는 환자 군 A에서 평균 35.4분(표준 편차±9.6), 환자군 B에 서는 13.3분(표준 편차±5.83)으로 변형된 신전 차단 K-강선 고정술의 경우에서 짧은 것으로 나타났다.
Ishiguro 등36은 변형된 신전 차단 K-강선 고정술의 경우 수상 8주 이상이 지나면 결과가 안 좋다고 하였 고, Khanna 등37은 수술이 지연된 경우 비관혈적 방 법은 해부학적 정복이 쉽지 않아서 여러 번 K-강선을 삽입하게 되므로 골과 연골의 열 손상 및 관절면의 불 일치가 생길 수 있고 그에 따른 이차적인 외상 후 관 절염이 생길 수 있다고 하였다. 본 연구에서는 비록 1 예 이지만 8주가 지난 경우에서도 만족할 만한 해부학 적 정복 및 골 유합을 얻을 수 있었다. 그러나 장기간
의 추시 관찰을 하지 않아서 관절염 발생 여부는 관찰 할 수 없었다.
결 론
골성 추지에서 골절편이 관절면의 30% 이상을 차지 하거나 원위지골의 수장부 아탈구가 있는 경우에서 시 행되는 두 가지 수술적 치료법의 결과를 비교해 본 결 과 원위지간 관절의 운동 범위 회복 정도와 Crawford 식 기능 평가 결과에서는 통계학적으로 유의한 차이가 없었으나 변형된 신전 차단 K-강선 고정술의 경우 수 술 시간의 경우 더 적은 시간이 소요되었다. 피부 괴사 나 감염 등의 합병증의 가능성 및 수술 수기의 상대적 용이성 그리고 수술 시간 등을 고려해 볼 필요는 있으 나 임상 결과만을 놓고 판단해 볼 때 수술적 치료가 필 요한 추지 골절에서 두 가지 수술 방법 모두가 좋은 결 과를 가져올 수 있는 치료법으로 생각된다.
참고문헌
01) Darder-prats A, Fernandez-garcia E, Fernandez-gabada R, Darder-garcia A. Treatment of mallet finger fractures by the extension-block K-wire technique. J Hang Surg Br.
1998;23:802-5.
02) Crawford GP. The molded polyethylene splint for mallet finger deformities. J Hand Surg Am. 1984;9:231-7.
03) Niechajev IA. Conservative and Operative treatment of mallet finger. Plast Reconstr Surg. 1973;16:366-75.
04) Stark HH, Gainor BJ, Ashworth CR, Zemel NP, Rickard TA. Operative treatment of intra-articular fractures of the dorsal aspect of the distal phalanx of digits. J Bone Joint Surg Am. 1987;69:892-6.
05) Wehbe MA, Schneider LH. Mallet fractures. J Bone Joint Surg Am. 1984;66:658-69.
06) Damron TA, Engber WD. Surgical treatment of mallet fin- ger fractures by tension band technique. Clin Orthop.
1944;300:133-40.
07) Hamas RS, Horrell ED, Pierret GP. Treatment of mallet finger due to intra-articular fracture of the distal phalanx. J Hand Surg Am. 1978;3:361-3.
08) Inoue G. Closed reduction of mallet fractures using exten- sion-block Kirschner wire. J Orthop Trauma. 1992;6:413-5.
09) Doyle JR. Extensor tendons-acute injuries. In: Green DP, editor. Operative hand surgery. 4th ed. New York:
Churchill Livingstone; 1999. p1950-1987.
10) Jupiter JB, Sheppard JE. Tension wire fixation of avulsion fractures in the hand. Clin Orthop. 1987;214:113-20.
11) Ishiguro T, Inoue K, matsubayashi N, Itoh Y, Hashizume N. A new method of closed reduction for mallet fractures.
Cent Jpn J Orthop Trauma Surg. 1988;31:2049-51.
12) Clement R, Wray RC Jr. Operative and nonoperative treat- ment of mallet finger. Ann Plast Surg. 1986;16:136-41.
13) Lubahn JD. Mallet finger fractures: a comparison of open and closed technique. J hand Surg Am. 1989;14:394-6.
14) Moiemen NS, Elliot D. Early active mobilization of pri- mary flexor tendon repairs in zone 1. J Hand Surg Br.
2000;25:78-84.
15) Kang HJ, Shim DJ, Choi JC, Yoon HK, Lee SY, Hahn SB.
Pulp traction technique for the operative treatment of bony mallet finger. The Journal of the Korean Society for Surgery of the Hand. 2005;10:162-8.
16) Hahn SB, Kim HS, Park HS, Kang HJ. Treatment of bony mallet finger with extension block technique. The Journal of the Korean Society for Surgery of the Hand. 2005;10:227- 33.
17) Kalainov DM, Hoepfner PE, Hartigan BJ, Caroll C IV, Genuario J. Nonsurgical treatment of closed mallet finger fractures. J Hand Surg Am. 2005;30:580-5.
18) Auchincloss JM. Mallet finger injuries. The Hand.
1982;14:168-73.
19) Kim YH, Kim KW, Min HJ, Yoon US, Baek JH. Outcome study on operative treatment of mallet finger. The Journal of the Korean Society for Surgery of the Hand. 2002;7:34- 41.
20) Tetik C, Gudemez E. Modification of the extension block kirschner wire technique for mallet finger. Clin Orthop.
2002;404:284-90.
21) Badia A, Riano F. A simple fixation method for unstable bony mallet finger. J Hand Surg Am. 2004;29:1051-5.
22) Jones NF, Peterson J. Epidemiologic study of the mallet finger deformity. J Hand Surg Am. 1988;13:334-8.
23) Okafor B, Mbubaegbu C, Munshi I, Williams DJ. Mallet deformity of the finger: Five-year follw-up of conservative treatment. J Bone Joint Surg Br. 1997;79:544-7.
24) Takami H, Takahashi S, Ando M. Operative treatment of mallet finger due to intra-articular fracture of the distal phalanx. Arch Orthop Trauma Surg. 2000;120:9-13.
25) Yamanaka K, Sasaki T. Treatment of mallet fractures using compression fixation pins. J Hand Surg Br.
1999;24:358-60.
26) Pennig D, Gausepohl T, Lukosch R. Use of a fixation pin for fragment stabilization in hand surgery. Handchirurgie Mikrochirurgie Plastische Chirurgie. 1994;26:270-4.
27) Stern PJ, Kastrup JJ. Complications and prognosis of treat- ment of mallet finger. J Hand Surg Am. 1988:13:341-6.
28) Bischoff R, Buechler U, Roche R, Jupiter J. Clinical results of tension band fixation of avulsion fractures of the hand. J Hand Surg Am. 1994;19:1019-26.
29) Ulusoy MG, Karalezli N, Kocer U, Uysal A, Karaaslan O, Kankaya Y, et al. Pull-in suture technique for treatment of mallet finger. Plast Reconstr Surg. 2006;118:696-702.
30) Teoh LC, Lee JYL. Mallet Fractures: A novel approach to internal fixation using a hook plate. J Hand Surg Br.
2007;32:24-30.
31) Rocchi L, Genitiempo M, Fanfani F. Percutaneous fixation of mallet fractures by the “Umbrella handle” technique. J Hand Surg Br. 2006;31:407-12.
32) Hofmeister EP, Mazurek MT, Shin AY, Bishop AT.
Extension block pinning for large mallet fractures. J Hand Surg Am. 2003;28:453-9.
33) Pegoli L, Toh S, Arai K, Fukuda A, Nishikawa S, Vallejo IG. The Ishiguro extension block technique for the treat- ment of mallet finger fracture: indication and clinical results. J Hand Surg Br. 2003;28:15-17.
34) Kang HJ, Shin SJ, Kang ES. Complications operative treatment for mallet fractures of the distal phalanx. J Hand Surg Am. 2001;26:28-31.
35) Nakamura K, Nanjyo B. Reassesment of surgery for mal- let finger. Plast Reconstr Surg. 1994;93:141-9.
36) Ishguro T, Itoh Y, Yabe Y, Hashizume N. Extension block with kirschner wire for fracture dislocation of the distal interphalangeal joint. Tech Hand Up Extrem Surg.
1997;1:95-102.
37) Khanna A, Plessas SJ, Barrett P, Bainbridge LC. The ter- minal effects of Kirschner wire fixation on small bones. J Hand Surg Br. 1999;24:355-7.