205
Received:June 16, 2014, Revised (1st) August 1, 2014, (2nd) August 21, 2014, Accepted:August 21, 2014
Corresponding to:Sang-Won Lee, Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 120-752, Korea. E-mail : sangwonlee@yuhs.ac
pISSN: 2093-940X, eISSN: 2233-4718
Copyright ⓒ 2015 by The Korean College of Rheumatology. All rights reserved.
This is a Free Access article, which permits unrestricted non-commerical use, distribution, and reproduction in any medium, provided the original work is properly cited.
Case Report
Journal of Rheumatic Diseases Vol. 22, No. 3, June, 2015 http://dx.doi.org/10.4078/jrd.2015.22.3.205
전신홍반루푸스에서 동반된 대동맥염
정수영ㆍ박혜선ㆍ지종현ㆍ이충근ㆍ이지연ㆍ박지은ㆍ한승희ㆍ박용범ㆍ이수곤ㆍ이상원 연세대학교 의과대학 세브란스병원 내과학교실
A Case of Aortitis with Systemic Lupus Erythematosus
Su-Young Jung, Hye-Sun Park, Jong Hyun Jhee, Choong-Kun Lee, Ji-Yeon Lee, Ji-Eun Park, Seung-Hee Han, Yong-Beom Park, Soo-Kon Lee, Sang-Won Lee
Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
A 21-year-old woman with a history of systemic lupus erythematosus (SLE) was admitted with dyspnea on exertion for a year.
A transesophageal echocardiogram showed dilated aortic root with intimal thickening. A positron emission tomog- raphy/computed tomography demonstrated increase in glucose hypermetabolic along the walls of the aortic valve, ascending aorta, aortic arch, and aorta, vasculitis was observed. She underwent the Bentall operation due to inflammation at sinus of right coronary cusp. She started high dose glucocorticoid after the operation. Currently she is able to sustain with low dose steroid after gradually tapered. Her symptoms were disappeared, and inflammatory markers decreased to within the normal range.
Aortitis and aortic aneurysms are an uncommon manifestation of SLE. Furthermore, almost of lupus patients with medium and large vessel vasculitis are not biopsied or studied histologically. We present first case in Korea that was a 21-year-old woman who diagnosed with lupus aortitis by pathology after aortic valve replacement operation. (J Rheum Dis 2015;22:205-208) Key Words. Systemic lupus erythematosus, Aortitis
서 론
전신홍반루푸스는 피부, 관절, 신장, 폐, 심장, 신경계 등 을 침범하여 염증 반응과 조직 손상을 초래하는 자가면역 질환이다[1,2]. 침범하는 장기에 따라서 다양한 증상이 나 타나는데, 심혈관계를 침범하는 경우에는 치명적인 합병 증을 초래할 수 있다. 일반적으로 전신홍반루푸스 관련 혈 관염은 주로 관상동맥이나 중소동맥에 발생하는데 대동맥 을 침범하는 경우는 매우 드문 것으로 보고가 되고 있고, 보고된 사례의 경우 대부분이 대동맥류나 대동맥 박리, 혈 전을 동반하였으며 부검 또는 수술 중 발견이 되었다[3,4].
Silver 등[5]은 2006년 전신홍반루푸스로 진단받은 30세 남자에서 대동맥혈전과 관련한 대동맥염이 진단된 경우를
보고하였으며 이는 대동맥류나 대동맥박리를 동반하지 않 은 첫 번째 사례이다.
또 다른 증례로는 반복적인 폐렴으로 입원한 23세 여자 환자에게서 심장 자기공명영상을 통해 대동맥염이 진단되 어 대동맥 근부 및 상행대동맥부위 치환술 및 관상동맥우 회로 수술을 받은 사례가 있었다[6].
하지만 아직까지 국내에서 타카야수 동맥염에 동반된 루 푸스 신염 1예가 보고된 바를 제외하고는 전신홍반루푸스 환자에서 발생한 대동맥염은 보고된 바가 없다. 이에 저자 들은 전신홍반루푸스 진단 후 대동맥 판막 역류증으로 대 동맥판막 치환술을 받은 후에 루푸스 대동맥염이 진단된 증례를 보고한다.
Su-Young Jung, et al.
206 J Rheum Dis Vol. 22, No. 3, June, 2015
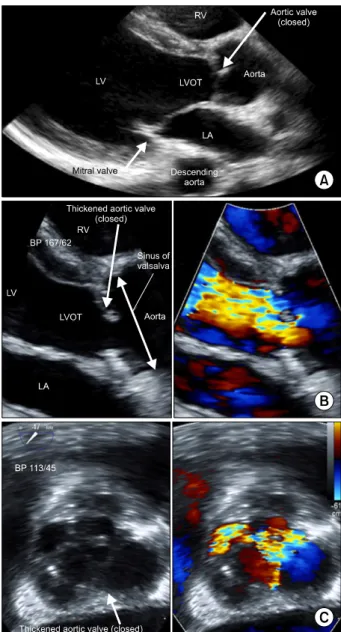
Figure 1. (A) Parasternal long axis view of transthoracic echo- cardiography showed slightly thickened aortic valve and mod- erately thickened aortic root. (B) Parasternal long axis view of transthoracic echocardiography (zoomed view) showed thick- ened aortic valve and aortic root (left). Color Doppler showed jet flow of severe aortic regurgitation in diastole (right). (C) 47o aortic valve short axis view of transesophageal echocardiog- raphy showed focally thickened aortic valve and aortic root (left). Color Doppler showed jet flow of aortic regurgitation in diastole (right). BP: blood pressure, LA: left atrium, LVOT: left ventricular outflow tract, LV: left ventricle, RV: Right ventricle.
증 례
21세 여자가 1년간의 간헐적인 가슴 통증 및 심계항진, 운동시 호흡곤란, 피로감을 주소로 입원하였다. 2년 전 3 개월간의 야간 발열을 주소로 타 병원에 내원하였으며 내 원 당시 말초혈액 검사에서 백혈구 수치는 8,360/mm3, 혈 색소 7.7 g/dL, 혈소판 396,000/mm3, C-reactive protein (CRP) 17 mg/L (0∼0.5 mg/L), erythrocyte sedimentation rate (ESR) 75 mm/h (0∼30 mm/h), C3/C4 53/12 mg/dL (C3 90∼180 mg/dL, C4 17∼45 mg/dL), 직접쿰스검사 양 성, 항핵항체 양성(1:160 이상), 항dsDNA항체 양성 소견 보여 전신홍반루푸스가 진단되었다. 얼굴의 나비모양 발 진, 원형의 반점, 광과민성, 입안 궤양, 장간막염 소견은 없었으며, 소변검사에서 단백뇨는 없었고, 두통, 경련 등 의 신경학적 변화는 보이지 않았다. 이후 전신홍반루푸스 로 추적관찰 중 설사증상으로 입원하였고, 당시 시행한 복 부 전산화단층촬영에서 소장 장간막의 림프절이 관찰되는 것 외에 대동맥염을 의심할 만한 소견은 없었다.
전신홍반루푸스 진단 당시 검사에서 루푸스 항응고인자 양성, 항-카디오리핀 항체 immunoglobulin (Ig) M 약양 성, IgG 음성을 보였고, 항-베타2 당단백 IgM 양성, IgG 음성소견을 보였다. 12주 후에 재시행한 검사에서 항응고 인자 양성, 항-카디오리핀 항체 IgM 양성, 항-베타2 당단 백 IgM 음성, IgG 음성 소견 보였으며 양측 허벅지 부종 및 통증으로 시행한 다리부위 초음파에서 표층정맥 혈전 정맥염이 보여 항인지질항체 증후군에 합당하므로 와파린 투여를 시작하였다. 당시 심전도상 동성 빈맥 및 측부 사 지유도에서 ST 분절 하강소견을 보여 시행한 경흉부 심장 초음파에서 대동맥 판막의 석회화 및 중증도의 대동맥 판 막 역류증을 보였고 정상 좌심실 이완기말 직경을 보였다.
좌심실 구출률은 59%로 확인되었고 호흡곤란, 심계항진 등의 증상이 두드러지지 않아 경과관찰 하였으며 pre- dnisolone 2.5 mg 하루 2회 복용하며 추적관찰 하였다.
이번 입원 시 신체 검진에서 호흡은 정상이었고, 심음은 규칙적이었으나 확장 초기 심잡음이 좌연 상부에서 청진 되었다. 심전도에서는 동성 빈맥 소견 및 좌심실 비대 소 견이 보였고, 호흡곤란에 대한 원인 감별을 위해 시행한 경흉부 심장초음파에서 대동맥판이 두꺼워져 판막엽의 불 완전 접착으로 인하여 중증 대동맥 판막 역류증을 보였으 며, 좌심실 구출률은 58%로 이전과 큰 차이는 없었으나 좌심실 확장소견(좌심실 이완기말 직경 55 mm)을 보였 다. 경식도 심장초음파에서 대동맥근이 부분적으로 두꺼 워져 있고, 부종을 보여 대동맥염이 의심이 되었으며, 대 동맥 판막엽이 전반적으로 두꺼워지고 판막엽 움직임 제 한을 보이며 중증 대동맥 판막 역류증 소견을 보였으며, 그 외 혈전소견은 보이지 않았다(Figure 1). 시행한 검사 에서 백혈구 수치는 6,640/mm3, 혈색소 13.4 g/dL, 혈소 판 348,000/mm3, 총단백질 7.5 g/dL, 알부민 4.1 g/dL였
으며 단순 뇨검사에서 단백뇨 음성이었고, C3/C4 87/20 mg/dL (C3 90∼180 mg/dL, C4 10∼40 mg/dL), CRP 55 mg/L (0∼8 mg/L), ESR 67 mm/h (0∼20 mm/h), 항핵 항체 양성(1:160 이상), 항dsDNA항체 모호한 양성이었으 며, 이전 양성이었던 항응고인자, 항-카디오리핀 항체, 항- 베타2 당단백 모두 음성이었다. 대동맥염을 확인하기 위
A Case of Lupus Aortitis in Korea
www.jrd.or.kr 207
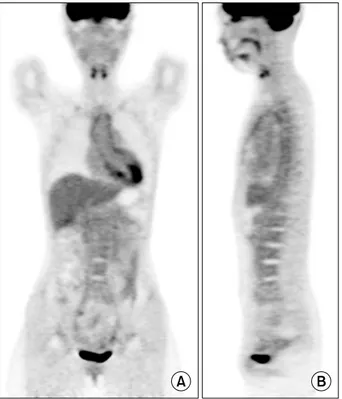
Figure 2. Positron emission tomography/computed tomog- raphy shows significant increased in 18-fluorodeoxyglucose uptakes along the walls of aortic valve, ascending aorta, aortic arch, descending thoracic aorta, and abdominal aorta, that were suggestive of vasculitis. (A) Coronal view, (B) sagittal view.
Figure 3. Aortitis was present in ascending aorta biopsy. It showed necrotizing inflammation of media with neovascularization and lymphoplasmacytic infiltration in media and adventitia associated with small vessel vasculitis, consistent with lupus aortitis. (A) Hematoxylin-eosin, Media (×200), (B) Elastic van Gieson stain (×40).
해 시행한 positron emission tomography/computed to- mography (PET/CT)에서 대동맥 판막벽과 상행 대동맥, 대동맥활, 하행 대동맥, 복부 대동맥에서 혈관염을 시사하 는 fluorodeoxyglucose (FDG) 섭취가 관찰되었다(Figure
2). 대동맥 판막 역류증에 대해 벤탈 수술을 시행받았고, 대동맥 판막 및 상행대동맥에서 시행한 조직검사에서 비 감염성 대동맥염으로서 주로 중간 막의 괴사성 염증소견 및 림프구 형질세포 침윤이 관찰되었으며, 거대세포 반응 은 관찰되지 않았다. 대동맥 혈관벽내의 혈관 및 신생혈관 의 혈관염이 동반되어 있는 점으로 볼 때 전신홍반루프스 에 의한 대동맥염으로 판단되었다(Figure 3). 타카야수 동 맥염의 경우 전층 동맥염의 소견을 보이며 단핵세포 침윤 이 관찰될 수 있고, 육아종성 반응과 층판괴사가 관찰되며 탄력 섬유의 단편화가 두드러지게 나타날 수 있으나 그런 특징이 없는 점으로 타가야수 동맥염을 배제하였다[7]. 루 푸스 대동맥염에 대해 prednisolone 50 mg를 시작하였고 증상 호전을 보이며 CRP 55 mg/L (0∼8 mg/L), ESR 67 mm/h (0∼20 mm/h)에서 치료 6개월째 CRP 1.2 mg/L (0∼8 mg/L), ESR 16 mm/h (0∼20 mm/h)으로 정상화 되었으며, 심장 초음파 추적 검사상 인공판막의 기능은 정 상이었고, 온전한 상행대동맥이 관찰이 되어 predniso- lone 10 mg까지 감량하여 추적 관찰 중이다.
고 찰
대동맥염은 감염성 혹은 비감염성을 모두 포함하며 대동 맥 벽의 이상 염증반응으로 인한 것을 말하고, 루푸스 대 동맥염은 전신홍반루푸스의 전신 침범으로 나타날 수는 있으 나 대동맥 혈관 침범은 드문 것으로 보고가 되고 있다[8].
비감염성 대동맥염의 흔한 원인은 거대세포 동맥염과 타 카야수 동맥염으로 알려져 있으며, 외국에서는 루푸스 대 동맥염에 대한 증례보고가 있으나 우리나라에서 루푸스 관련 대동맥염은 드문 증례이다[9].
타카야수 동맥염일 때는 임상 특징이 파행, 상완동맥 맥
Su-Young Jung, et al.
208 J Rheum Dis Vol. 22, No. 3, June, 2015
박의 감소, 양팔의 혈압차, 빗장 밑 동맥이나 복부 대동맥 에서 잡음이 청진될 수 있는 특징이 있으나 이 환자에서는 그런 소견은 보이지 않아 타카야수 동맥염은 배제하였다.
또한 루푸스 환자에서 판막 이상을 보일 때 감별이 필요한 리브만-삭스 심내막염의 경우 감염과 상관없이 판막의 증 식이 나타나며 주로 왼쪽의 판막, 승모판막의 심실면에서 나타나고, 그 기전으로는 혈소판-피브린 혈전의 형성이 관 련되어 있으며 섬유화를 일으키고 흉터형성 및 판막부전 을 일으키는 것으로 알려져 있다. 혈액검사 결과 항인지질 항체가 증가될 수 있는 것으로 알려져 있는데 이 환자의 경우 판막의 증식 소견은 관찰되지 않아 리브만-삭스 심내 막염 가능성은 없었다[10].
전신홍반루푸스에서 대동맥류의 형성에 관한 메타분석 논문에서 두 가지 가설을 제시하였는데 두 가지 다른 요인 이 대동맥의 다른 부위를 침범하는 것을 가정하였다. 분석 결과 대동맥의 중간막의 파괴는 혈관염과 연관되어 있으 며 주로 흉부 대동맥을 침범하였다. 죽상동맥경화증은 이 기전에서 중요하지 않았으며, 혈관염의 진행이 흉부 대동 맥류를 일으켰다. 반면 전신홍반루푸스의 환자에서 복부 대동맥류는 죽상동맥경화증과 관련이 있었으며 장기간의 스테로이드 사용과 관련성이 있었다[11,12].
이번 증례의 경우 CT나 magnetic resonance imaging의 검사는 시행하지 않았으며, PET/CT상 대동맥 판막벽과 상행 대동맥, 대동맥활, 하행 대동맥, 복부대동맥에서 혈 관염을 시사하는 FDG 섭취가 관찰되었다. 보통 루푸스 환 자에서 중간막의 파괴가 대부분 흉부대동맥을 침범하며 대동맥류나 대동맥 박리를 동반하는 데 비해 이 환자의 경 우 흉부대동맥 및 복부 대동맥까지 모두 침범하였고, 대동 맥류나 대동맥 박리를 동반하지 않았다. 전신홍반루푸스 의 대동맥류 기전과 관련된 죽상동맥경화증에 대한 평가 를 위한 경동맥 초음파는 시행되지 않았고, 경동맥 평가가 추후 진료 시 도움이 될 것으로 생각되며 병리검사에서 림 프구 형질세포 침윤을 보이는 IgG 관련 질환에 대한 감별 진단 또한 필요할 것으로 생각된다.
루푸스 대동맥염의 1차 치료로는 코르티코스테로이드가 이용되고, 루푸스에서 대동맥염이 드물지만 높은 이환율 과 사망률을 보인다. 이 환자의 경우 스테로이드를 사용하 며 증상 조절되어 추적관찰 중이다.
요 약
대동맥염은 전신홍반루푸스의 흔한 합병증이 아니며 대
혈관 혈관염이 조직학적으로 확진된 경우는 드물다. 이번 증례는 우리나라에서 대동맥류 및 대동맥 박리, 대동맥 혈 전을 동반하지 않고 PET/CT 및 조직 검사를 통해서 루푸 스 대동맥염이 확진이 되어 스테로이드 치료 중인 첫 번째 증례이다.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Slobodin G, Naschitz JE, Zuckerman E, Zisman D, Rozenbaum M, Boulman N, et al. Aortic involvement in rheumatic diseases. Clin Exp Rheumatol 2006;24(2 Suppl 41):S41-7.
2. Ramos-Casals M, Nardi N, Lagrutta M, Brito-Zerón P, Bové A, Delgado G, et al. Vasculitis in systemic lupus eryth- ematosus: prevalence and clinical characteristics in 670 patients. Medicine (Baltimore) 2006;85:95-104.
3. Breynaert C, Cornelis T, Stroobants S, Bogaert J, Vanhoof J, Blockmans D. Systemic lupus erythematosus complicated with aortitis. Lupus 2008;17:72-4.
4. Wang J, French SW, Chuang CC, McPhaul L. Pathologic quiz case: an unusual complication of systemic lupus erythematosus. Arch Pathol Lab Med 2000;124:324-6.
5. Silver AS, Shao CY, Ginzler EM. Aortitis and aortic throm- bus in systemic lupus erythematosus. Lupus 2006;15:541-3.
6. Dhaon P, Das SK, Saran RK, Parihar A. Is aorto-arteritis a manifestation of primary antiphospholipid antibody syn- drome? Lupus 2011;20:1554-6.
7. Vaideeswar P, Deshpande JR. Pathology of Takayasu arter- itis: a brief review. Ann Pediatr Cardiol 2013;6:52-8.
8. Drenkard C, Villa AR, Reyes E, Abello M, Alarcón-Segovia D. Vasculitis in systemic lupus erythematosus. Lupus 1997;
6:235-42.
9. Gornik HL, Creager MA. Aortitis. Circulation 2008;117:
3039-51.
10. Ménard GE. Establishing the diagnosis of Libman-Sacks en- docarditis in systemic lupus erythematosus. J Gen Intern Med 2008;23:883-6.
11. Kurata A, Kawakami T, Sato J, Sakamoto A, Muramatsu T, Nakabayashi K. Aortic aneurysms in systemic lupus eryth- ematosus: a meta-analysis of 35 cases in the literature and two different pathogeneses. Cardiovasc Pathol 2011;20:e1-7.
12. Ohara N, Miyata T, Kurata A, Oshiro H, Sato O, Shigematsu H. Ten years’ experience of aortic aneurysm associated with systemic lupus erythematosus. Eur J Vasc Endovasc Surg 2000;19:288-93.