143
•교신저자:송기학, 충남대학교 의학전문대학원 비뇨기과학교실 대전 중구 문화로 33 우 301-721
Tel: 042-2280-7777, Fax: 042-257-0966 E-mail: urosong@cnu.ac.kr
Received: September 2, 2010 Accepted: September 28, 2010
급성 신우신염
충남대학교 의학전문대학원 비뇨기과학교실
송기학∙이지용∙김영호[Abstract]
Acute Pyelonephritis
Ki Hak Song, Ji Young Lee, Young Ho Kim
From the Department of Urology, Chungnam University School of Medicine, Daejeon, Korea
Acute pyelonephritis is a very common upper urinary tract infection, and most of them may be uncomplicated and resolve without serious sequelae. Acute pyelonephritis is defined as clinical symptoms and signs such as abrupt onset of chills, fever, and flank or costovertebral angle pain and/or tenderness.
The incidence of acute pyelonephritis is higher in young women than in men and then the incidence is similar to women over 65 years old. In general, acute pyelonephritis is caused by microorganisms ascending from the bladder into the upper urinary tract. E. coli is the most common uropathogen causing pyelonephritis, accounting for 70∼90% of infections. Recently, antibiotic resistance against E. coli and uropathogen is remarkably noted in uncomplicated acute pyelonephritis as well as uncomplicated UTI. The purpose of this study was to determine the recent trends of acute pyelonephritis, to suggest change to current strategies in the management and prevention of acute pyelonephritis, and to review 2010 EAU guideline and recent literatures. (Korean J UTII 2010;5:143-150)
Key Words: Acute pyelonephritis, Management
서 론
급성신우신염은 임상적인 질환으로 대부분 방광 염 증상 없이 38℃ 이상의 고열을 동반한 측복부통 증 및 오심과 구토가 나타나는 신우신배계와 신간
질의 세균성감염으로 치료를 소홀이 하면 사망할
수 있으며 비교적 치료비용이 많이 드는 상부요로
감염질환이다.
1신우신염의 유병률은 대단히 높은
것으로 알려져 있다. 특히 여성은 해부학적인 요인
으로 인해 20∼35%가 일생 동안 한 번 이상 신우
신염을 경험하는 것으로 알려져 있으며 급성신우
신염은 대부분의 경우 요로감염에 의한 상행성 전
파가 주된 경로이다. 1997년 미국의 통계자료에 의
하면 급성신우신염의 유병률은 연간 250,000명이
며, 이 중 입원치료를 받은 환자가 10,000명 당 여
자는 11.7명, 남자는 2.4명으로 보고하였다.
2국내
보고로는 1년에 인구 10,000명 당 35.7명의 높은 발
병률을 보이며 이 중 여자는 9.96명, 남자는 1.18명 이 입원치료를 받는 흔한 질환이다.
3그러나 근래 에는 항생제의 오남용으로 인한 내성균이 증가하 고 있으며 병원감염의 증가로 인해 적극적인 치료 및 예방이 필요한 실정이다. 이에 저자들은 급성신 우신염의 증상, 진단, 치료 및 특수한 상황에서의 치료 등에 관한 내용을 중심으로 2010년 유럽비뇨 기과학회 권고안과 문헌고찰을 통하여 최근 경향 에 대하여 정리하고자 한다.
본 론
환자군은 비교적 젊은 연령의 여성에서 호발하 며 고령이나 남성에서 발병할 경우 입원치료의 가 능성이 높아지고 임상적으로 다른 특성을 나타낼 가능성이 있다. 급성신우신염의 임상진단은 전통적 으로 임상증상, 증후, 발열정도, 백혈구증다증, 소변 검사 및 배양검사를 토대로 진단하게 된다.
1위험 인자로는 하부요로감염, 임신, 하부요로폐색, 방광 요관역류, 유전적 요인 등이 있으며, 이러한 위험인 자가 있을 때 신우신염이 더 빈번하게 발생하게 되 며 임상양상도 더 심한 경우가 많다.
1. 임상증상
임상 양상은 그람 음성 패혈증부터 경도의 측복 부 통증이 있는 방광염까지 다양하게 나타난다. 대 표적 증상으로는 수시간 내지 하루 사이에 급격히 발생하는 39.4℃ 이상의 고열, 오한, 그리고 일측성 또는 양측성 측복부 통증이며 배뇨통, 빈뇨, 급박뇨 등의 하부요로 증상을 동반할 수도 있다. 유아 및 소아에서는 식욕부진과 체중감소와 같은 비특이적 증상을 보이는 경우가 많아 진단이 늦어지는 경우 가 있을 수 있다.
2. 진단
급성신우신염의 진단으로 신체검사, 검사실검사 및 방사선 검사가 있지만 방사선검사는 특별히 달 라진 내용이 없으며 신체검사는 비뇨기과학의 기
본적 내용이므로 여기에서는 신체검사 및 검사실검 사만 논하고자 한다. 신우신염은 의미있는 세균뇨를 동반한 측복부통증 및 발열을 언급하지만 임상증상 이 염증부위와 일치하지 않는다. Busch와 Huland
4는 재발성 요로감염이 있는 201명의 여자와 12명의 남 자를 대상으로 한 연구에서, 발열과 측복부통증으로 신우신염의 진단을 내리지 못한다고 발표하였고 측 복부통증 및 발열이 있는 환자의 50% 이상은 하부 요로 세균뇨를 동반하고 있다. 반대로 방광 증상이 있든 없든 이러한 환자들은 종종 상부요로세균뇨 가 있으며 약 75%의 환자는 하부요로감염의 기왕 력이 있다. 신체검사에서 늑골척추각 압통이 가장 뚜렷한 소견이며 이는 신실질의 부종으로 신피막 이 팽창되어 발생한다. 또한 급성신우신염은 위장 관계를 자극하여 복부통증, 오심, 구토, 설사 등을 유발할 수 있으며 청진시 장음이 감소할 수 있다.
특히 면역력 저하가 있는 환자에서 급성 신우신염 의 만성 신우신염으로의 진행은 확실한 증상 없이 발생할 수 있고 급성 신부전은 드물게 발생할 수 있다. 환자들은 대부분 호중구가 많은 비중을 차지 하는 백혈구 증가증이 있으며, 뇨검사에서는 보통 많은 수의 백혈구, 백혈구 원주 및 그람염색에서 세균이 발견되며, 소변에 많은 양의 granular casts 또는 leukocyte casts가 존재하는 것은 신실질의 감 염이 있다는 것을 의미한다. 세균과 함께 특정 cast 의 존재는 급성신우신염 환자의 소변에서 확인할 수 있으며 혈액검사는 호중구가 많은 비중을 차지 하는 백혈구 증가증, 적혈구 침강속도의 증가, C-reactive protein의 증가와 함께 신부전이 동반된 경우 혈청 creatinine 수치의 증가가 나타날 수 있으 며 creatinine clearance는 감소할 수 있다. 또한 혈액 배양 검사에서 양성을 나타날 수도 있다.
단순 급성신우신염의 주된 원인균은 E. coli이며,
Jung 등
5은 2000년부터 2005년까지 2,901명을 대상
으로 한 국내 다기관연구에서 79%가 E. coli에 의한
신우신염으로 보고하였다. 요배양 검사에서 세균이
검출된 경우는 46.3%에 불과하였으며 1차 의료기관
이나 약국에서항생제를 복용한 결과라고 생각되며
이에 대한 실태조사가 필요할 것이라고 하였다. 또한
E. coli 외에 Klebsiella pneumonia (3.7%), Pseudomonas
Table 1. Antibiotic resistance for Gram negative organisms10
Drug resistance (%)
Organism Year AM CF FOX CTX CAZ CXM GM CIP IPM SXT
E. coli 1996 80.7 42.9 9.4 6.4 - - 42.9 26.2 0.0 64.0
1997 78.0 39.3 7.5 5.9 - - 36.1 23.6 0.7 59.3
1998 80.5 46.6 7.5 3.9 - - 42.7 26.4 0.0 60.9
1999 79.9 46.7 9.0 3.4 - - 34.0 36.3 0.3 88.0
2000 86.4 51.1 12.5 8.2 - - 46.2 48.9 0.5 54.9
2001 75.4 64.1 11.1 4.9 - - 36.7 43.7 0.2 50.8
2002 72.0 48.4 29.2 7.4 - - 29.2 38.3 0.5 41.5
2003 75.8 53.2 11.0 16.0 - - 35.2 40.4 0.2 45.4
2004 75.1 56.1 19.0 21.5 - - 37.8 41.7 0.0 52.4
2005 78.8 59.4 29.4 30.6 - - 30.0 44.1 0.0 44.1
Total 77.4 51.4 14.3 10.2 - - 36.5 37.2 0.2 56.0
Klebsiella 1996 94.3 40.0 2.9 20.0 - - 37.1 5.7 - 34.3
1997 94.4 44.4 2.8 11.1 - - 44.4 2.8 - 52.8
1998 92.7 53.7 9.8 12.2 - - 39.0 4.9 - 48.8
1999 98.8 42.7 6.1 18.3 - - 28.0 9.8 - 42.7
2000 94.4 50.0 16.7 33.3 - - 16.7 11.1 - 33.3
2001 100.0 68.2 25.8 31.8 - - 54.5 25.8 - 36.4
2002 98.9 63.6 19.3 53.4 - - 45.5 30.7 - 37.5
2003 96.1 50.0 14.5 40.8 - - 38.2 13.2 - 39.5
2004 97.2 52.3 45.9 45.9 - - 43.1 39.4 - 43.1
2005 100.0 75.5 67.9 71.7 - - 52.8 52.8 - 54.7
Total 97.1 54.9 23.1 35.5 - - 41.4 22.0 - 42.6
Acinetobacter 1996 90.5 100.0 100.0 61.9 76.2 57.1 4.8 57.1
1997 93.8 93.8 87.5 62.5 50.0 31.3 12.5 56.3
1998 97.1 98.5 98.5 91.0 77.6 83.6 3.0 79.1
1999 85.5 95.2 93.5 69.4 72.6 66.1 3.2 66.1
2000 100.0 96.3 100.0 85.2 85.2 88.9 0.0 77.8
2001 93.5 99.1 99.1 75.9 76.9 71.3 10.2 76.9
2002 97.6 97.6 96.4 88.1 81.0 89.3 86.9 11.9 79.8
2003 93.3 100.0 100.0 71.1 68.9 71.1 71.1 17.8 66.7
2004 94.1 97.1 91.2 64.7 52.9 55.9 50.0 58.8 5.9 58.8
2005 100.0 100.0 96.0 68.0 56.0 48.8 68.0 52.0 16.0 64.0
Total 94.3 98.1 96.9 77.1 69.7 52.5 75.3 72.2 8.6 72.0
Enterobacter 1996 92.6 96.3 92.6 25.9 - - 48.1 7.4 0.0 51.9
1997 95.1 92.7 87.8 46.3 - - 43.9 19.5 2.4 29.3
1998 93.2 95.5 97.7 38.6 - - 56.8 34.1 0.0 70.5
1999 90.9 100.0 90.9 15.2 - - 48.5 12.1 0.0 48.5
2000 96.4 100.0 92.9 35.7 - - 32.1 14.3 0.30 32.1
2001 92.5 98.1 88.7 45.3 - - 34.0 37.7 0.0 37.7
2002 100.0 100.0 96.6 44.8 31.0 - 34.5 27.6 3.4 37.9
2003 95.2 95.2 95.25 50.0 47.6 - 38.1 16.7 2.4 38.1
2004 91.7 100.0 100.0 41.7 37.5 33.3 29.2 37.5 4.2 37.5
2005 94.4 94.4 100.0 33.3 33.3 22.2 22.2 16.7 0.0 22.2
Total 94.1 97.1 93.5 38.9 38.9 28.6 40.1 23.6 1.2 41.9
AM: ampicillin, CF: cephalothin, FOX: cefoxitin, CAZ: ceftazidime, CTX: cefotaxime, CXM: cefuroxime, GM: gentamicin, CIP: ciprofloxacin, TMP/SMX: trimethoprim/sulfamethoxazole, IPM: imipenem
Table 2. Recommended initial empirical antimicrobial therapy in acute uncomplicated pyelonephritis in otherwise healthy premenopausal women (2010 EAU guidelines)
I. Oral therapy in mild and moderate cases
Antibiotic Daily dose Duration of therapy (days) Reference
Ciprofloxacina 500∼750mg bid 7∼10 15
Levofloxacina 250∼500mg qd 7∼10 16
Levofloxacin 750mg qd 5 17,18
Alternatives (clinical but not microbiological equivalent efficacy compared with fluoroquinolones):
Cefpodoxime proxetil 200mg bid 10 14
Ceftibuten 400mg qd 10 13
Only if the pathogen is known to be susceptible (not for initial empirical therapy):
Trimethoprim–sulphamethoxazole 160/800mg bid 14 15
Co-amoxiclavb,c 0.5/0.125g tid 14
a: lower dose studied, but higher dose recommended by experts b: not studied as monotherapy for acute uncomplicated pyelonephritis c: mainly for Gram-positive pathogens
II. Initial parenteral therapy in severe cases.
After improvement, the patient can be switched to an oral regimen using one of the above-mentioned antibacterials (if active against the infecting organism) to complete the 1∼2-week course of therapy. Therefore, only daily dose and no duration of therapy are indicated:
Antibiotics Daily dose Reference
Ciprofloxacin 400mg bid 15
Levofloxacina 250∼500mg qd 16
Levofloxacin 750mg qd 17
Alternatives:
Cefotaximeb 2g tid
Ceftriaxonea,d 1∼2g qd 19
Ceftazidimeb 1∼2g tid 20
Cefepimea,d 1∼2g bid 21
Co-amoxiclavb,c 1.5g tid
Piperacillin/tazobactama,d 2.5∼4.5g tid 22
Gentamicinb 5mg/kg qd
Amikacinb 15mg/kg qd
Ertapenemd 1g qd 19
Imipenem/cilastatind 0.5/0.5g tid 22
Meropenemd 1g tid 20
Doripenemd 0.5g tid
a: lower dose studied, but higher dose recommended by experts b: not studied as monotherapy in acute uncomplicated pyelonephritis c: mainly for Gram-positive pathogens
d: same protocol for acute uncomplicated pyelonephritis and complicated UTI (stratification not always possible)
BLI = β-lactamase inhibitor; TMP = trimethoprim; SMX = sulphamethoxazole
Fig. 1. Clinical management of acute pyelonephritis (2010 EAU guidelines).
aeruginosa (3.3%) 등의 순서로 배양되었고 그람양성 균인 Enterococcus species와 Staphylococcus aureus도 3.9%와 1.5%로 나타났으며, 남자 환자에서는 여자 환 자에 비해 E. coli의 비중이 낮고 P. aeruginosa,
Enterococcus species의 빈도가 높아 성별에 따른 차이
를 보였다. 요로감염의 원인균에 대한 연구는 발생
지역과 시기에 따라 그 결과에 차이가 있다. 국내
에서는 급성신우신염 환자의 요배양균에서 E. coli
의 비율은 1980년대의 자료에서는 69.1∼81.6%로
보고되었고,
6,790년대 후반과 2000년대 초에는 79
∼91%로 다소 증가하는 경향을 보이나
8,9통계적인 검증이 필요할 것으로 생각한다. 또한 Chung 등
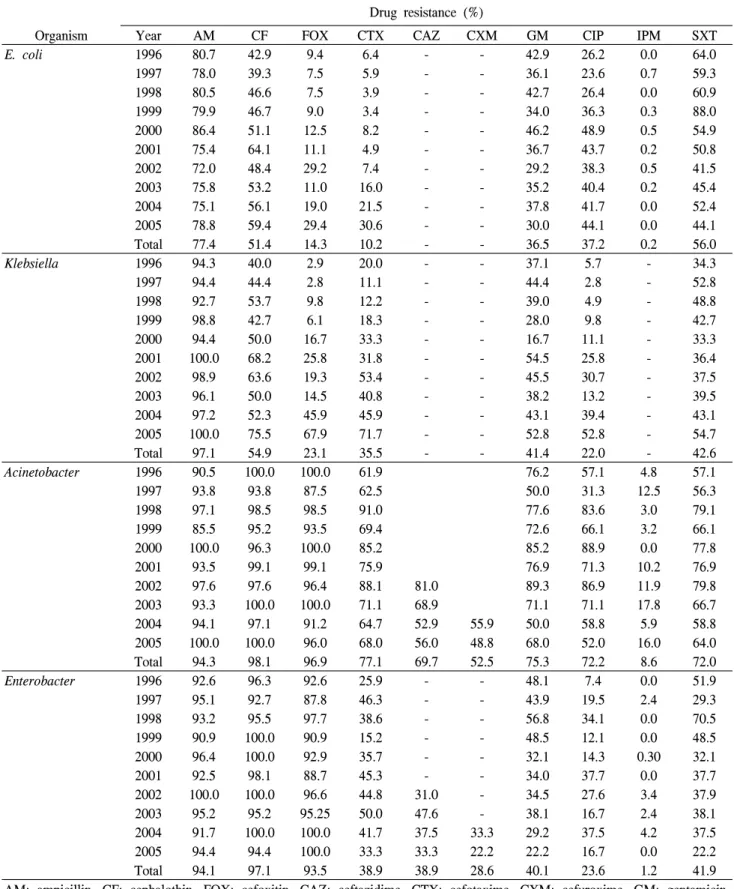
6은 E. coli의 항생제에 대한 감수성에서는 ampicillin 37.7%, cephazolin 66.1%, trimethoprim/sulfamethox- azole (TMP/SMX) 62.8%, gentamicin 73.9%으로 보 고하였다. Kim 등
10은 1996년부터 2005년까지의 요 로감염환자를 대상으로 대장균에 대한 내성률을 연구하여 전, 후기로 나누어 비교하였다. Ampicllin 의 내성률은 평균 77.4%로 높았으며 전기는 80.6%
에서 후기는 75.0%로 소폭 감소하였고 cephalothin, cefoxitin 및 cefotaxim에 대한 내성률은 평균 51.5%, 11.4% 및 10.2%였으며 전후기 비교 시에도 각각 45.0%에서 56.1%로, 8.9%에서 18.2%로, 그리고 5.2%에서 13.9%로 내성률이 증가함을 보였으며, 특 히 ciprofloxacin에 대한 내성률은 26.2%에서 44.1%
로 현저히 증가하였다고 보고하였다 (Table 1). 향 후 유용한 경험적 일차약물로서 사용하기 위해서 는 항생제 사용의 남용을 지양하고 적응증을 제한 하여 사용하여야 하며 적절한 항생제 선택을 위해 항생제 내성 패턴에 대한 주기적인 조사의 필요성 을 주장하였다.
3. 치료
가장 중요한 것은 신속한 진단으로 적절한 항생 제를 투여하여 합병증을 예방하는 것이다. 일반적 으로 치료 전에 소변배양검사나 그람염색을 하게 되며 배양검사가 나오기 전까지는 경험적 항생제 를 투여하고 요로폐색, 신경인성방광 및 결석이 있 을 때는 가능한 한 교정하여 준다. 임상증상이 소 실되었다고 항상 세균학적 완치를 의미하는 것은 아니라는 점을 알아야 한다. 급성 신우신염 환자는 입원을 필요로 하지 않는 합병증이 동반되지 않은 감염과 비경구 치료를 위해 입원이 필요할 정도로 아픈 정상적인요로를 가진 합병증이 동반되지 않 은 감염, 그리고 도뇨관 삽입, 비뇨기과적 수술, 요 로계 비정상과 연관이 있는 합병증을 동반한 감염 으로 입원이 꼭 필요한 경우로 나눌 수 있다.
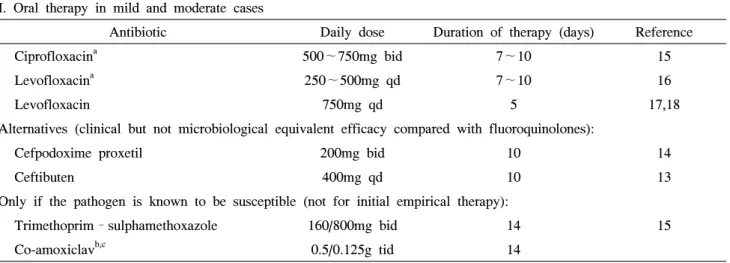
11유럽비뇨기과학회 권고안에 따르면 단순급성신우
신염인 중 경증 혹은 중증인 경우는 10∼14일간의
경구항생제요법을 권장하고 있으며 E. coli의 내성률
이 10% 미만인 경우는 7∼10일간의 fluoroquinolone
을 일차치료로 권장하고 있다.
12Cefpodoxime prox-
etil 혹은 ceftibuten 같은 3세대 경구 cephalosporin이
대체요법으로 사용할 수는 있지만 ciprofloxacin보다
임상적으로는 비슷한 효과를 보이나 효율성이나
미생물학적인 측면에서는 좋다고 할 수는 없다
(Table 2).
13,14그러나 앞에서 언급하였듯이 우리나
라에서는 ciprofloxacin의 E. coli에 대한 내성률이
높기 때문에 경험적 일차치료로 사용할 때는 신중
한 고려가 필요할 것으로 생각된다. Fluoroquinolone
대한 E. coli 내성률이 10% 미만일 때는 비경구 flu-
oroquinolone이나 3세대 cephalosporin을 투여하지만
fluoroquinolone 대한 E. coli 내성률이 10% 이상일
때는 aminoglycoside 혹은 carbapenem의 투여를 고
려한다.
12급성신우신염 환자에서 합병증 동반의 유
무를 판단하는 것이 매우 중요하며 이는 입원치료
를 결정하는 중요한 요인 중의 하나이다. 만일 환
자가 항생제 경구투여에 순응하지 않고 위중한 경
우에는 즉각적인 입원치료 및 비경구 항생제투여
를 하여야 하며 초기에 절대안정, 충분한 비경구적
수분공급, 및 해열제를 투여하는 것이 필요하다. 급
성신우신염 환자는 비록 항생제 치료 후 소변이 무
균상태가 될지라도, 며칠 동안 발열, 오한, 측복부
통증을 지속적으로 호소할 수 있으며 따라서 환자
에 대한 지속적인 관찰이 필요하다는 것을 항상 생
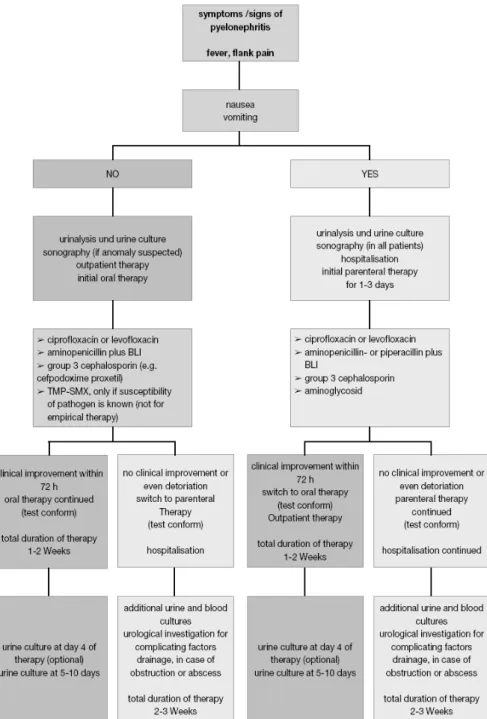
각하여야 한다. 입원 환자는 fluoroquinolone 혹은 3
세대 cephalosporin으로 적어도 1∼3일 동안 치료해
야하며 72시간 내에 임상증상이 호전되면 경구약으
로 바꾸어 통원치료를 시도한다. 그러나 지속적인
증상이 있거나 심해지면 비경구항생제 투여를 지속
하며 추가적인 뇨배양검사, 혈액배양검사 및 초음파
혹은 콤프터단층촬영 등의 비뇨기과적 검사가 필요
하며 항생제의 변경을 고려하게 되며 이 때 항생제
에 대한 환자의 임상적인 반응과 배양검사의 결과
와 감수성 검사를 참고해야 하며 적어도 2∼3주의
치료기간이 필요하게 된다 (Fig. 1). 치료 후 무증상
환자에서는 뇨검사나 뇨배양검사가 필요하지는 않
으며, 3일 이내에 증상의 호전을 보이지 않으나 2주
내에 치료된 후 재발된 여성에게는 뇨검사나 뇨배 양검사 및 항생제 감수성검사가 반복적으로 필요하 고 방사선학적 비뇨기계검사가 필요하다.
결 론
신우신염의 원인균으로서 E. coli에 의한 감염이 가장 많았으며 항생제에 대한 내성도 같이 증가하 고 있고 현재는 ampicillin, TMP/SMX을 신우신염의 일차약제로 사용하는 비뇨기과의사는 없을 것이다.
Ciprofloxacin도 최근 들어 내성률이 현저하게 증가 하여 신우신염의 일차약제로는 부적합한 것으로 나타나고 있다. 따라서 새로 개발된 비싼 약제를 투여하게 되며 진료비의 상승을 유도하는 원인으 로 작용할 수 있을 것이다. 비용적인 측면을 고려 하지 않는다 하더라도 차후에 치료에 불응하는 균 주가 생기지 않게 하기 위해서는 항생제 투여시 감 염의 특성 및 항생제의 작용범위, 부작용 등을 고 려하여 내성균의 발생을 최소화 할 수 있는 항생제 선택을 하는 것이 바람직할 것으로 생각한다.
REFEENCES
1. Hooton TM, Stamm WE. Diagnosis and treatment of uncomplicated urinary tract infection. Infect Dis Clin North Am 1997;11:551-81
2. Foxman B, Klemstine KL, Brown PD: Acute pyelo- nephritis in US hospitals in 1997: hospitalization and in-hospital mortality. Ann Epidemiol 2003;13:144-50 3. Ki M, Park T, Choi B, Foxman B. The epidemiology
of acute pyelonephritis in South Korea, 1997-1999. Am J Epidemiol 2004;160:985-93
4. Busch R, Huland H. Correlation of symptoms and re- sults of direct bacterial localization in patients with uri- nary tract infections. J Urol 1984;132:282-5
5. Jung YH, Cho IR, Lee SE, Lee KC, Kim JG, Jeon JS, et al. Comparative analysis of clinical parameters in acute pyelonephritis. Korean J Urol 2007;48:29-34 6. Chung KS, Ko SS, Yoon YJ, Park YH, Son KS, Lee
KY. A clinical study on acute pyelonephritis. Korean J Med 1984;27:597-606
7. Son HS, Ahn JH, Lee TY, Lim CK, Kim MJ. Clinical
study on 740 cases of acute pyelonephritis (1980-1989).
Korean J Nephrol 1990;9:380-8
8. Min HJ. Acute pyelonephritis; clinical study and con- sideration about inpatient therapy. Korean J Med 1998;
55:232-45
9. Lee JS, Rho SH, Kim SE, Nam TM, Kim JS, Kim SK, et al. A study on the clinical and microbiologic features of community-acquired acute pyelonephritis for the recent 5 years in a university hospital. Korean J Nephrol 2002;21:905-13
10. Kim JM, Lee SD, Jang CH. A single center study of the change of antibiotic resistance to the causative or- ganisms of urinary tract infection for recent 10 years.
Korean J UTII 2008;3:63-74
11. Schaeffer AJ, Schaeffer EM. Kidney infection. In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell-Walsh urology. 9th ed. Philadelphia:
Saunders; 2007;265-71
12. Grabe M, Bjerklund-Johansen TE, Botto H, Çek M, Naber KG, Tenke P, et al. EAU guidelines on uro- logical infections. 2010;11-6
13. Cronberg S, Banke S, Bergman B, Boman H, Eilard T, Elbel E, et al. Fewer bacterial relapses after oral treat- ment with norfloxacin than with ceftibuten in acute pye- lonephritis initially treated with intravenous cefuroxime.
Scand J Infect Dis 2001;33:339-43
14. Naber KG, Schoenwald S, Hauke W. Cefpodoxime prox- etil in patients with acute uncomplicated pyelonephritis.
International, prospective, randomized comparative study versus ciprofloxacin in general practice. Chemother J 2001;10:29-34
15. Talan DA, Stamm WE, Hooton TM, Moran GJ, Burke T, Iravani A, et al. Comparison of ciprofloxacin (7 days) and trimethoprim-sulfamethoxazole (14 days) for acute uncomplicated pyelonephritis pyelonephritis in women: a randomized trial. JAMA 2000;283:1583-90 16. Richard GA, Klimberg IN, Fowler CL, Callery-D’Amico
S, Kim SS. Levofloxacin versus ciprofloxacin versus lo- mefloxacin in acute pyelonephritis. Urology 1998;52:51-5 17. Klausner HA, Brown P, Peterson J, Kaul S, Khashab M, Fisher AC, et al. A trial of levofloxacin 750 mg once daily for 5 days versus ciprofloxacin 400 mg and/or 500 mg twice daily for 10 days in the treatment of acute pyelonephritis. Curr Med Res Opin 2007;23:
2637-45
18. Peterson J, Kaul S, Khashab M, Fisher AC, Kahn JB.
A double-blind, randomized comparison of levofloxacin 750 mg once-daily for five days with ciprofloxacin 400/500 mg twice-daily for 10 days for the treatment of complicated urinary tract infections and acute pyelonephritis. Urology 2008;71:17-22
19. Wells WG, Woods GL, Jiang Q, Gesser RM.
Treatment of complicated urinary tract infection in adults: combined analysis of two randomized, dou- ble-blind, multicentre trials comparing ertapenem and ceftriaxone followed by an appropriate oral therapy. J Antimicrob Chemother 2004;53:ii67-74
20. Mouton YJ, Beuscart C. Empirical monotherapy with meropenem in serious bacterial infections. Meropenem Study Group. J Antimicrob Chemother 1995;36:145-56 21. Giamarellou H. Low-dosage cefepime as treatment for
serious bacterial infections. J Antimicrob Chemother 1993;32:123-32
22. Naber KG, Savov O, Salmen HC. Piperacillin 2 g/tazo- bactam 0.5 g is as effective as imipenem 0.5 g/cil- astatin 0.5 g for the treatment of acute uncomplicated pyelonephritis and complicated urinary tract infections.
Int J Antimicrob Agents 2002;19:95-103