ORIGINAL ARTICLE
41
방광요관역류 환아에서 요관 점막하 Dextranomer/Hyaluronic Acid Copolymer (Deflux
Ⓡ) 주입치료의 경험
Experience of Subureteral Dextranomer/Hyaluronic Acid Copolymer (Deflux
Ⓡ) Injection Treatment in Children with Vesicoureteral Reflux
Jong Jin Oh, Sang Hyun Jee, Young Kwon Hong
From the D epartm ent of U rology, College of M edicine, CH A U niversity, Seongnam , Korea
오종진ㆍ지상현ㆍ홍영권 포천중문의과대학교 비뇨기과학교실
Purpose: We assessed the results of endoscopic subureteral Dextra- nomer/Hyaluronic acid copolymer (DefluxⓇ) injection treatment in chil- dren with vesicoureteral reflux.
Patients and Methods: Between September 2006 and December 2007, a total of 30 (51 renal units) VUR patients underwent subureteral DefluxⓇ injection treatment. All the patients were postoperatively assessed by ul- trasound and voiding cystourethrography (VCUG) to evaluate any compli- cation and the result of treatment.
Results: The mean follow-up period was 5.9 months (range 3-17). Of the 51 refluxing ureters, 14 were cured (27.5%) and 26 were improved (50.9%) after treatment. Cure rates by ascending grade were 100%, 0%, 36%, 18%, 0% after 1st trial with DefluxⓇ. All of two grade I VURs were cured (100%). Of two grade II VURs, one was improved (50.0%) and the other was persistent (50.0%). Of 22 grade III VURs, eight were cured (36.4%), 12 improved (54.5%), and two were persistent (9.1%). Of 22 grade IV VURs, four were cured (18.2%), 11 improved (50.0%), and seven were persistent (31.8%). Of three grade V VURs, none was cured, two improved (66.7%), and one was persistent (33.3%). There was no sig- nificant complication associated with this procedure. All of the cured pa- tients had sterile urine even without prophylactic antibiotics, and none of the patients with bacteriuria after the procedure proved to be cured.
Conclusions: An endoscopic subureteral DefluxⓇ injection can be used as the 1st line of therapy for VUR because it is a safe procedure without causing any significant complication. Downgrading was encountered in more than half of the cases. However, the cure rate was not so high prob- ably due in some part to the fact that this study was our initial experience. Additional injection trial after failed initial injection is wor- thy of consideration. Postoperative bacteriuria is thought to be a sig- nificant factor to predict the result of the operation.
Key Words: Deflux, Injection, Vesico-Ureteral reflux (Received: February 28, 2009, Accepted: March 16, 2009) 교신저자
홍영권
분당차병원 비뇨기과 경기도 성남시 분당구 야탑동 351, 463-712 Tel: 031-780-5353 Fax: 031-780-5323 E-mail: [email protected]
서 론
방광요관역류는 소아에서 1-2%의 유병률을 보이 며, 특히 소아 요로 감염 환자의 30-40%에서 발견된 다.1 국제소아역류연구회 분류법에 따라 I-II 등급의 방광요관역류는 자연적으로 호전이 되는 경우가 많 지만, III-IV 등급의 방관요관역류는 5년 이내에 16%
만이 자연적으로 호전된다고 한다.2,3 치료는 내과적 치료로 예방적 항생제 사용과 외과적 치료로서 개복 항 역류 수술 및 내시경 요법으로 크게 나눌 수 있다.
내시경 요법은 1981년 Matouschek4이 보고하고, 1984년 O’Donell 등5,6이 polytetra-fluoroethylene (PTFE, TeflonⓇ) 를 시도한 이후에 현재 널리 사용되고 있다. 특히, DefluxⓇ는 여러 연구를 통해 효과와 안정성이 입증되 어 최근 역류 교정의 1차 치료로 인정되고 있다.7 이에 저자들은 소아 역류에 대한 내시경적 요관점막하 DefluxⓇ 주입 치료의 효과와 안전성에 대해 알아보고 자 하였다.
대상 및 방법
2006년 9월부터 2008년 12월까지 방광요관역류로 요관점막하 DefluxⓇ 주입치료를 시행한 환자 30명 (51 신 단위)을 대상으로 후향적으로 자료를 분석하였다.
모든 환아에서 술 전 신장초음파, 배뇨중 방광요도조 영술, 신주사 (99mTc-DMSA)를 시행하였으며, 방광요 관역류의 등급은 1985년 국제소아역류연구회에서 소 개한 분류법을 사용하여 I-V단계로 분류하였다.
요관 점막하 DefluxⓇ 주입치료의 적응증은 1) 발열 성 요로감염이 발생한 병력이 있거나 신주사에서 신 반흔이 있는 VUR, 2) III 등급 이상의 VUR로 하였으 며, 1)과 2) 모두 보호자가 예방적 항생제 복용을 원하 지 않는 경우에 시행하였다.
시술 당시 환자의 평균 나이는 5.76±3.1세로, 30명 중 남아가 13명, 여아가 17명이었다. 수술은 한 명의 술자 (operator)에 의해 이루어졌다. 대상 환아를 전신 마취 후 쇄석위 자세에서 소아용 방광내시경 (8/9.5 Fr, Richard Wolf, Germany)을 이용하여 요도 및 방광 내를 관찰한 후, 23 gauge의 주사용 바늘에 생리식염수를 통과한 뒤 Deflux가 들어있는 주사기와 연결하여 시술 하였다. 수술 후 도뇨관은 삽입하지 않았고, 다음날 아침 환아가 소변을 잘 보고 발열이 없으면 1주간의
경구용 항생제를 처방받고 퇴원하였다. 수술 이후 1-2 주 사이에 신장초음파, 요검사, 요배양검사를 시행하 였으며, 이후 1개월 간격으로 요검사와 요배양검사를 시행하여 세균뇨가 있는 경우에만 예방적 항생제를 사용하였다. 수술 후 3개월에는 배뇨중 방광요도조영 술을 시행하여 방광요관역류의 소실 여부를 확인하 였다. 역류가 소실되지 않았을 경우에는 잔존 역류의 등급에 따라 I-II 등급은 추적 관찰을, III-IV 등급은 Deflux 2차 시도를, V 등급은 개복수술을 시행하는 것 을 원칙으로 하였으나 보호자의 선택을 고려하여 결 정하였다. 결과에 대한 판단은 역류가 완전히 소실되 었을 경우를 완치 (cured), 수술 전 등급에 비해 낮아진 경우 호전, 수술 전과 동일한 경우 지속으로 판단하였 다.
결 과 1. 대상 환자 특성
전체 51요관 중, 양측성이 14요관, 단측성이 23요관 이었다. 수술 전 요로감염 횟수는 평균 2.2±1.3회 (1-8) 였으며, DMSA 신주사에서 환측의 상대 신기능은 평 균 36.6±18.2%였다. 수술 전 역류의 등급은 신 단위 기준으로 I 등급이 2례, II 등급이 2례, III 등급이 22례, IV 등급이 22례, V 등급이 3례였다 (Table 1).
2. DefluxⓇ 주입치료의 성적
추적 관찰기간은 3개월에서 17개월 사이로 평균 5.9개월이며, 수술 후 3개월에 시행한 배뇨중 방광요 도조영술 시행 결과 완치는 14례 (27.5%), 호전은 26례 (50.9%)로 총 41 신 단위에서 역류의 완치 및 호전을 보였으며, 11례 (21.6%)에서는 변화가 없었다 (Table 2).
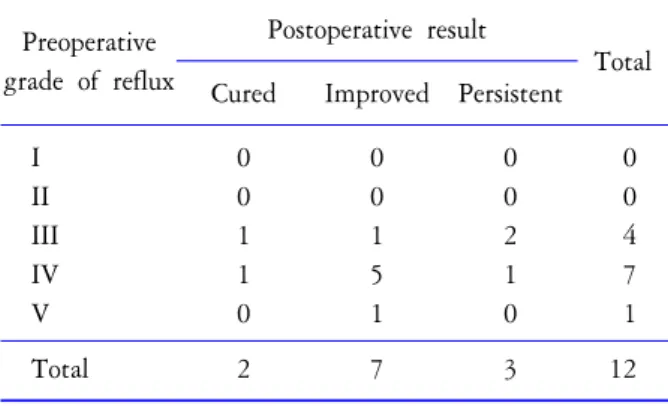
1차 시술 후에도 III 등급 이상의 역류가 있었던 12례 (III 등급이 4례, IV 등급이 7례, V 등급이 1례)의 경우, 2차 시술을 시행한 후 완치가 2례 (16.7%), 호전은 7례 (58.3%), 지속은 3례 (25.0%)로 1차 시술 결과와 비교 하여 완치율은 더 낮았다 (Table 3).
3. 수술 후 경과
수술 후 임상적으로 유의한 요관폐색의 증상은 발 견되지 않았으며, 육안적 혈뇨를 보인 경우라도 2-3일 이내에 호전되었다. 수술 후 1-2주 사이에 시행한 신 장 초음파에서 수술 전에 관찰되지 않았던 수신증의 발생 및 악화는 없었으며, 수술 후 1-2주 사이에 시행
Table 2. Treatment results after initial injection of Deflux Preoperative
grade of reflux
Postoperative result
Total Cured Improved Persistent I
II III IV V
2 0 8 4 0
0 1 12 11 2
0 1 2 7 1
2 2 22 22 3
Total 14 26 11 51
Table 4. Treatment results according to postoperative bacteriuria
Preoperative bacteriuria
Postoperative result
Total Cured*
(%)
Improved (%)
Persistent*
(%) (+)
(−)
0 (0.0) 14 (36.8)
5 (38.5) 21 (55.3)
8 (61.5) 3 (7.9)
13 38
Total 14 26 11 51
*: p<0.05
Table 3. Treatment results of second trial after failed initial injection of Deflux
Preoperative grade of reflux
Postoperative result
Total Cured Improved Persistent I
II III IV V
0 0 1 1 0
0 0 1 5 1
0 0 2 1 0
0 0 4 7 1
Total 2 7 3 12
Table 1. Patients’ characteristics Variables
No. of renal unit Bilateral Unilateral Age (year)
Laterality (right:left) Number of febrile UTI VUR grade
I II III IV V
14 23 5.76±3.1
20:31 2.2±1.3
2 2 22 22 3
UTI: urinary tract infection, VUR: vesicoureteral reflux
한 요배양검사에서 105개 이상의 CFU (colony-forming unit)가 배양되는 유의한 세균뇨가 있었던 환아는 8명 (13 신 단위), 없었던 환아는 22명 (38 신 단위)이었다.
발열성 요로감염으로 입원 치료가 필요했던 환아는 2명으로 한 명은 Deflux 2차 시술로 역류가 소실되었 으며 나머지 한 명은 요관방광재문합술을 시행받았 다. 세균뇨가 없었던 경우에는 완치 14례 (36.8%), 호 전 21례 (55.3%), 지속 3례 (7.9%)로, 세균뇨가 있던 경 우 완치 0례 (0.0%), 호전 5례 (38.5%), 지속 8례 (61.5%)의 결과에 비해 유의하게 높은 성공율을 보였 다 (p<0.05) (Table 4).
고 찰
방광요관역류의 교정 수술은 방광 점막 아래 요관 의 길이를 충분히 확보하고 요관 말단부가 방광 근육
층의 충분한 지지를 받게 하여 배뇨 중 요관구가 폐쇄 상태를 유지하도록 하는 것을 목표로 한다. 같은 원리 로 비교적 시술 방법이 간단한 요관 점막하 이물질 주입치료가 고안되었는데, 관혈적 수술을 피할 수 있 는 장점이 있다. 1984년 O'Donnell과 Puri가 polytetra- fluoroethylene (Teflon)을 이용한 주입 요법을 보고한 이 후 Teflon을 포함하여 collagen, polydimethylsiloxane (Macroplastique), Deflux 등을 이용한 연구들이 보고되 었다. 방광 점막 아래에 주입되는 이물질은 타 장기로 전이가 없어야 하고, 전이가 되더라도 안전해야 하며, 이상 반응을 보이지 않고 장기간 효과를 유지하여야 이상적이지만, 실제로는 이물질 입자의 이동, 염증 및 육아종성 반응 등으로 안전성에 문제가 대두되어 왔 다.8-11 인체에 무해하면서 시술 부위에 염증 또는 면 역 반응, 이동, 전이가 없이 쉽게 주입할 수 있는 물질 로 2001년 미국 식약청 (Food and Drug Administration) 의 승인을 받은 DefluxⓇ는 1995년 Stenberg와 Lackgren12 이 보고한 이후 현재 가장 많이 사용되는 방광요관역 류 치료 물질 중 하나로 인식되고 있다.
지금까지 여러 연구에서 방광요관역류에 대한 DefluxⓇ 주입술의 치료 성공률은 65-90%로 보고되고 있으며, 성공률은 등급이 높을수록 낮아진다고 보고
되었다.13-15 본원에서의 치료 성공률은 완치율이
27.5%, 호전이 50.9%로 이전의 보고들에 비해 낮은 성 공률을 보였다. 이러한 차이의 가장 큰 원인은 Kirsch 등15이 보고한 학습 곡선 효과에서 기인한 것으로 판 단된다. 그들의 결과에 따르면, 20례까지는 성공률이 60%, 100례까지는 70%의 성공률을 보였으며, 100례 이후에 80%까지 성공률의 상승을 보고하여 학습 곡 선과 성공률간의 연관 요소가 크다고 하였다. 또한 환 아의 역류 등급 구성에 있어 IV 등급이 43%를 차지하 고 있는 점도 낮은 성공률을 초래한 원인으로 생각한 다.
Elmore 등16은 1차 DefluxⓇ 주입 시술을 받고 역류가 소실되지 않은 환아를 대상으로 2차 주입술을 시행하 였을 때, 39례의 환아 (53 신 단위)에서 84-92%의 높은 성공률을 보여 1차 DefluxⓇ 주입술 후, 특히 낮은 등급 의 방광요관역류가 남아있을 경우, 2차 주입술로 만 족할만한 결과를 얻을 수 있다고 보고하였다. 소규모 의 연구이긴 하지만 Lee 등17이 7례 (11 신 단위)의 환 아를 대상으로 2차 주입술을 시행한 국내 연구에서는 추적 검사가 가능한 3례 (4 신 단위) 중 1례 (1 신 단위) 에서 2차 주입술로 역류가 소실되었으며, 2례 (3 신 단위)에서는 역류가 잔존하여 요관방광재문합술을 시행하였다고 보고하였다. 본 연구에서 2차 시술한 환아는 12 신 단위 (7명)였으며, 결과는 완치가 2 신 단위 (16.7%), 호전은 7 신 단위 (58.3%), 지속은 3 신 단위 (25.0%)로 1차 시술과 큰 차이는 없었다.
1차 시술 후 잔존하였던 역류 등급이 III 등급이 4 례, IV 등급이 7례, V 등급이 1례로 구성에 있어 높은 등급의 역류가 많아 성공률이 다소 낮게 나온 것으로 판단된다.
방광요관역류에 대한 내시경적 Deflux 주입술 후 요 로감염이 발생하는 경우가 드물지 않은 데, Elder 등18 은 약 6%에서 요로감염이 발생하였다고 하였고, Chi 등19은 12%에서 열성 요로 감염이 발생하였다고 하였 다. Kang 등20의 보고에서는 1차 Deflux 시술 후 역류 가 잔존한 49명 중 16.2% (8/49)는 수술 후 예방적 항 생제를 복용했음에도 불구하고 열성 요로 감염이 발 생하였다고 한다. 본 연구에서 세균뇨는 26.7% (8/30 명)에서 발생하였으나 열성 요로감염으로 발현된 경 우는 6.7% (2/30명)로 기존의 보고와 큰 차이는 없었
다. 다만 본 연구에서는 추적 검사에서 세균뇨가 증명 된 경우에만 예방적 항생제를 사용하였다는 점을 고 려하여 결과를 해석해야 할 것이다.
Deflux 주입술의 성공 여부를 바로 확인하기 의해 Purlmutter 등21은 수술 종료 직전 방광 압박에 의한 VCUG 촬영을 시행하였는데 수술 전에 발견되지 않 았던 대측의 역류를 발견하는 경우는 있었지만 환측 의 Deflux 수술의 성공 여부를 예측할 수 는 없다고 하였다. Deflux 주입술의 성공 여부를 판단하는 인자 로서 ‘수술 후 세균뇨’가 유용한지에 대해서는 잘 알 려져 있지 않지만 본 연구에서는 수술 후 세균뇨가 없는 경우 더 높은 성공률을 보여 향후 이에 대한 추 가 연구가 필요할 것으로 생각한다.
결 론
내시경을 이용한 Deflux 주사는 안전한 방법으로 방 광요관역류의 치료에 일차적으로 사용될 수 있으며, 많은 경우 역류 등급의 하향 변화를 기대할 수 있으나 본 연구에서의 역류의 소실률은 기대에 미치지 못하 였다. 따라서 초기 경험 술자는 학습 곡선을 고려하여 역류에 대한 치료 계획을 세워야 할 것으로 생각한다.
시술 후에도 지속되는 세균뇨는 방광요관역류의 존 속을 의미하는 지표가 될 수 있을 것으로 판단된다.
REFERENCES
1. Perez-Brayfield M, Kirsch AJ, Hensle TW, Koyle MA, Furness P, Scherz HC. Endoscopic treatment with dextra- nomer/hyaluronic acid for complex cases of vesicoureteral reflux. J Urol 2004;172:1614-6
2. Puri P. Endoscopic correction of vesicoureteral reflux. Curr Opin Urol 2000;10:593-7
3. Tamminen-Mobius T, Brunier E, Ebel KD, Lebowitz R, Olbing H, Seppanen U, et al. Cessation of vesicoureteral reflux for 5 years in infants and children allocated to medical treatment. The International Reflux Study in Children. J Urol 1992;148:1662-6
4. Matouschek E. Treatment of vesicorenal reflux by transurethral teflon-injection. Urologe A 1981;20:263-4 5. O'Donnell B, Puri P. Treatment of vesicoureteric reflux by
endoscopic injection of Teflon. Br Med J 1984;289:7-9 6. Puri P, O'Donnell B. Correction of experimentally
produced vesicoureteric reflux in the piglet by intravesical injection of teflon. Br Med J 1984;289:5-7
7. Lackgren G, Wahlin N, Skoldenberg E, Stenberg A.
Long-term followup of children treated with dextrano- mer/hyaluronic acid copolymer for vesicoureteral reflux. J Urol 2001;166:1887-92
8. Joyner BD, Atala A. Endoscopic substances for the treatment of vesicoureteral reflux. Urology 1997;50:489-94 9. Bhatti HA, Khattak H, Boston VE. Efficacy and causes
of failure of endoscopic subureteric injection of Teflon in the treatment of primary vesicoureteric reflux. Br J Urol 1993;71:221-5
10. Smith DP, Kaplan WE, Oyasu R. Evaluation of polydimethylsiloxane as an alternative in the endoscopic treatment of vesicoureteral reflux. J Urol 1994;152:1221-4 11. Cukier J, Beauchamp RA, Spindler JS, Spindler S, Lorenzo
C, Trentham DE. Association between bovine collagen dermal implants and a dermatomyositis or a polymyo- sitis-like syndrome. Ann Intern Med 1993;118:920-8 12. Stenberg A, Lackgren G. A new bioimplant for the
endoscopic treatment of vesicoureteral reflux: experimental and short-term clinical results. J Urol 1995;154:800-3 13. Lorenzo AJ, Pippi Salle JL, Barroso U, Cook A, Grober
E, Wallis MC, et al. What are the most powerful determinants of endoscopic vesicoureteral reflux correction?
Multivariate analysis of a single institution experience during 6 years. J Urol 2006;176:1851-5
14. Méndez R, Somoza I, Tellado MG, Liras J, Sanchez A, Paris E, et al. Predictive value of clinical factors for successful endoscopic correction of primary vesicoureteral reflux grades III-IV. J Pediatr Urol 2006;2:545-50
15. Kirsch AJ, Perez-Brayfield MR, Scherz HC. Minimally invasive treatment of vesicoureteral reflux with endoscopic injection of dextranomer/hyaluronic acid copolymer: the Children's Hospitals of Atlanta experience. J Urol 2003;170:211-5
16. Elmore JM, Scherz HC, Kirsch AJ. Dextranomer/hyalu- ronic acid for vesicoureteral reflux: success rates after initial treatment failure. J Urol 2006;175:712-5
17. Lee DW, Kang KM, Oh WS, Kim JS, Chung SK. Risk factors for treatment failure after endoscopic subureteral injection of dextranomer/hyaluronic acid copolymer (Deflux
Ⓡ) for vesicoureteral reflux. Korean J Urol 2009;50:61-6 18. Elder JS, Diaz M, Caldamone AA, Cendron M, Greenfield
S, Hurwitz R, et al. Endoscopic therapy for vesicoureteral reflux: a meta-analysis. I. Reflux resolution and urinary tract infection. J Urol 2006;175:716-22
19. Chi A, Gupta A, Snodgrass W. Urinary tract infection following successful dextranomer/hyaluronic acid injection for vesicoureteral reflux. J Urol 2008;179:1966-9 20. Kang MY, Park DS, Park YH, Lee JW, Baek MK, Choi
H. Overall outcomes and factors predicting the success of endoscopic dextranomer/hyaluronic acid copolymer injection for vesicoureteral reflux. Korean J Urol 2009;50:51-6 21. Perlmutter AE, Talug C, Darbandi SS, Morabito R, Tarry
WF. Utility of an intra-operative cystogram with a simulated voiding phase after endoscopic treatment of vesicoureteral reflux. W V Med J 2008;104:22-4