- 55 -
KISEP Case Report J Rhinol 12(1), 2005
Foreign Body in the Orbit Associated with Blowout Fracture - A Case Report
Hong-Ryul Jin, M.D.
ABSTRACT
An orbital foreign body combined with blowout fracture after blunt trauma to the orbit may be difficult to diagnose clin- ically and radiologically. The author reports a case of 40-year-old woman who had an unsuspected orbital foreign body after blunt orbital trauma, and initially presumed to have only blowout fracture and conjunctival laceration. Consultation with an ophthalmologist failed to disclose the orbital foreign body and an isolated inferomedial blowout fracture was seen on computed tomography scans with severe diplopia and limitation of eye movement. She was referred to my department for management of the orbital blowout fracture, where a false eyelash was found during the endonasal endoscopic reduction and subsequently successfully removed that resulted in complete resolution of her symptoms. Though it is a rare complication, an orbital foreign body should be suspected considering the mechanism of injury when there are severe and persistent ocular symptoms incon- sistent with the degree of the blowout fracture.
KEY WORDS:Foreign body·Orbit·Blowout fracture.
CASE REPORT
A 40-year-old woman visited emergency room due to the periorbital pain after struck her left orbit by the stair during a slipping down accident. On examination, she had a periorbital swelling, ecchymosis, and lacer- ation of conjunctiva and sclera. Initially, she complained of diplopia with right gaze, but her ocular motility was normal. Computed tomography (CT) revealed mild left inferomedial blowout fracture (BOF)(Fig. 1). The la- ceration was repaired by the ophthalmologist and the BOF was managed conservatively. Ten days after the repair, her diplopia was aggravated with development of severe dizziness and ocular pain. Ocular motility sh- owed restriction with positive forced duction test and the repair site showed slight adhesion. Even after suc- cessful revision of the adhesion site, she continued to
have moderate ophthalmoplegia and severe diplopia.
One month after the injury, she was referred to my department and underwent endonasal endoscopic redu- ction of the inferomedial BOF. After uncinectomy and partial anterior ethmoidectomy, multiple black silk- like threads were found in the ethmoid cavity, which were first thought as a suture material (Fig. 2). After removal of the many fine threads, they could be traced into the herniated orbit that led to the removal of false eyelash (Fig. 3). After removal of the false eyelash, the fractured portion was reduced and supported with Merocel (Xomed, Jacksonville, FL, USA) after silastic sheeting. The Merocel was removed 18 days after the operation. One month after the operation, all symptoms improved. She has been followed up for 6 months and she is free of all preoperative symptoms.
DISCUSSION
Retained orbital foreign bodies are not rare and usu- ally related to the high velocity injuries to the orbit.1-3) Orbital foreign body after blunt trauma often presents challenges to both diagnosis and treatment, especially when it is associated with other orbital injuries like BOF.2)3)
Department of Otolaryngology, College of Medicine, Chungbuk National University, Cheongju, Korea
Address correspondences and reprint requests to Hong-Ryul Jin, M.D., Department of Otolaryngology, Chungbuk National Uni- versity Hospital, 62 San Gaeshin-dong, Heungdok-gu, Cheongju 361-711, Korea
Tel:82-43-269-6352, Fax:82-43-265-6157 E-mail:[email protected]
Accepted for publication on April 25, 2005
56 / J Rhinol 12(1), 2005
For proper and early diagnosis, a detailed history of the injury should be obtained first. Meticulous inspec- tion of the eyelids and globe including the conjunctival fornices should be undertaken if there is any suggestive history of penetrating injury or suspicion of an intraor- bital foreign body.4) Associated injuries to the eyelid, conjunctiva, globe, and periorbital swelling often make complete examination difficult and mask entry wounds.
Often such wounds appear deceptively superficial and insignificant, and their relevance is often dismissed by the patient and even by the examining ophthalmologist.5) In the present case, failure to suspect the possibility of
foreign body at times of conjunctival repair significantly delayed definitive treatment.
Often history and careful examination are not suffi- cient to rule out a retained foreign body and early imag- ing study is necessary to detect and localize the foreign body. These include plain radiographs, ultrasonography, CT, and magnetic resonance imaging (MRI).6) CT scan and ultrasonography are effective for detecting high- density material such as glass or metal.3) MRI may be necessary when an inorganic foreign body is highly suspicious though its usefulness is controversial. Even with the use of CT and MRI, only about 50% of cases are diagnosed preoperatively.5)7) In this case, careful re- view of the facial bone CT scan after the operation did elicit high suspicion of a foreign body consistent with small soft tissue density in the herniated orbital tissue.
The possibility for misinterpretation of the CT scan was high considering the fact that the false eyelash is a very rare foreign body with such kind of injury mechanism.
Metallic objects and glass fragments are the most fre- quently encountered orbital foreign bodies, and usually cause little inflammatory reaction with the exception of copper while organic foreign bodies usually incite an acute inflammation, which will cause serious complic- ation if it becomes chronic without removal.6) Treat- ment consists of adequate antibiotics and removal of the foreign body.6) Delays in diagnosis and management can lead to complications like periorbital abscess, pano- pthalmitis, orbito-cutaneous fistula and central nervous system extension. In this case, mild ophthalmitis might have occurred due to the delay in definitive treatment, which caused severe dizziness with ophthalmoplegia.
Fig. 1. CT scan shows inferomedial blowout fracture of the left orbit and a suspicious foreign body (arrow) within the hernia- ted orbital tissue.
Fig. 2. A false eyelash is being removed from the left orbital tissue herniated into the ethmoid cavity.
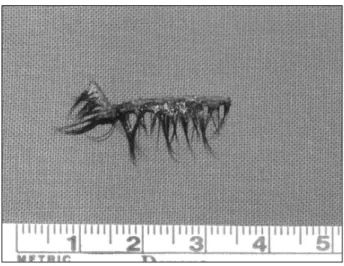
Fig. 3. A false eyelash removed from the left orbit.
Jin:Foreign Body in the Orbit / 57
In case with a suggestive history, even with apparently negative imaging results, exploration seems to be just- ified.3) Surgery to remove an orbital foreign body is not without risks. Though orbital foreign bodies are usually removed via external approach, they can be re- moved safely through endoscopic approach alone or in conjunction with the external approach according to the size and location. Endoscopic approach either thr- ough the nose or antrum provides a safe and effective way for extraction of these foreign bodies located near to the approaching sinuses.
The BOFs of the orbit should be explored and rep- aired when there are definitive indications like severe and persistent diplopia, evidence of muscle entrapment with positive forced duction test, and a CT scan show- ing large orbital wall fracture with displacement of the orbital contents. Waiting 10 to 14 days till the edema or hematoma goes away and the transient nerve palsy subsides is a routine in equivocal cases. When there is severe disabling diplopia or ophthalmoplegia inconsis- tent with the degree and severity of the fracture shown in CT scan, another possible cause should be sought considering the mechanism or characteristic of the in- jury specific to each case.2) In this case, persistence of disabling diplopia and restriction of eyeball movement for a month after trauma led to the exploration of the BOF.
CONCLUSION
Though orbital foreign bodies are not common in patients with BOF after blunt orbital trauma, persistent pain, diplopia, ophthalmoplegia, or proptosis which are not compatible with the severity of the associated BOF are suggestive of a retained orbital foreign body. Early diagnosis with proper imaging study and possible exp- loration can lead to successful management with little complication.
REFERENCES
1) Flynn SB, Cannon TC, Schmucker T, Davis R, Westfall C. Orbital foreign body. Arch Ophthalmol 2004;122:296-7.
2) Chen CS, Davis GJ, Selva D. Orbital foreign body misdiagnosed as superior orbital rim fracture. Clin Experiment Ophthalmol 2002;
30:295-6.
3) Tite DJ, Batstone MD, Lynham AJ, Monsour FN, Chapman PJ. Pen- etrating orbital injury with wooden foreign body initially diagnosed as an orbital floor blowout fracture. ANZ J Surg 2002;72:529-30.
4) Holt GR, Holt JE. Management of orbital trauma and foreign bod- ies. Otolaryngol Clin North Am 1988;21:35-52.
5) Nasr AM, Barrett GH, Fleming JC, Hailah M, Zeynel AK. Penetr- ating orbital injury with organic foreign bodies. Ophthalmology 1999;106:523-32.
6) Fulcher TP, McNab AA, Sullivan TJ. Clinical features and mana- gement of intraorbital foreign bodies. Ophthalmology 2002;109:
494-500.
7) Lustrin ES, Brown JH, Novelline R, Weber AL. Radiologic assess- ment of trauma and foreign bodies of the eye and orbit. Neuroim- aging Clin N Am 1996;6:219-37.