인공 슬관절 전치환술을 받은 한국인에서 대퇴골 원위부 및 경골 근위부의 해부학적 특징
Anatomic Characteristics of the Distal Femur and the Proximal Tibia in Koreans Undergoing Total Knee Arthroplasty
이건우* • 송은규 • 선종근 • 이동현* • 이태민*
화순전남대학교병원 관절센터, *전남대학교병원 정형외과
목적: 저자는 한국인의 대퇴골 원위부 및 경골 근위부의 해부학적 특징들을 분석하고, 남녀 간의 차이에 대하여 비교 분석하고자 하였다.
대상 및 방법: 슬관절 골관절염으로 ROBODOC®을 이용한 슬관절 전치환술을 시행받은 76명의 환자(여자: 50명, 남자: 26명)를 대상으로 하였으며, 대퇴골 원위부 및 경골 근위부의 해부학적 지표의 전후 길이 및 좌우 길이를 ORTHDOC program을 이용하여 측정하였다.
결과: 대퇴골 원위부 및 경골 근위부의 경우 한국 여성은 모든 해부학적 지표에서 남성에 비하여 작게 측정되었으며, 통계학적으로 유의한 차이를 보였다(모두 p<0.05). 하지만 전후 길이에 대한 좌우 길이의 비(Aspect ratio,%)의 경우 남녀 두 군 간에 대퇴골과 경골 모두에서 유 의한 차이를 보이지는 않았다(모두>0.05).
결론: 한국인 여성에서 대퇴골 원위부 및 경골 근위부의 좌우 길이에 대한 전후 길이의 비율이 남성과 다르지 않고 대칭적으로 작은 형태를 가진다고 할 수 있겠다.
색인단어: 대퇴골 원위부, 경골 근위부, 해부학적 특징, 한국 여성
접수일 2010년 12월 22일 게재확정일 2011년 5월 23일 교신저자 송은규
전남 화순군 화순읍 일심리 160, 화순전남대학교병원 관절센터 TEL 061-379-7676, FAX 061-379-7681
E-mail [email protected]
Copyright © 2011 by The Korean Orthopaedic Association
“This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.”
대한정형외과학회지:제 46권 제 6호 2011
서 론
현대 사회가 고령화되면서 전 세계적으로 슬관절 골관절염의 발 생 빈도가 증가하고 있다.1) 매년 골관절염으로 인하여 슬관절 전 치환술을 시행받는 인구가 늘어나고 있으며, 더욱이 여성의 경우 남성에 비해 빠른 속도로 증가하고 있다. 슬관절 전치환술의 경 우 술 전 관절 운동범위, 수술 방법, 치환물의 디자인 및 재활 방 법 등 다양한 요인들이 결과에 영향을 미치고 있다. 무엇보다도 적절한 크기의 치환물을 사용함으로써 연부 조직의 균형과 골 절 제면의 완전한 차폐(coverage)를 이루는 것이 중요하다.2) 정확한 연부 조직의 균형을 통해서 굴곡-신전 간격을 균일하게 하여야 관절 운동 시 안정성을 얻을 수 있으며 장기적으로 좋은 결과를
얻을 수 있기 때문에, 성공적인 슬관절 전치환술을 얻기 위해서 는 정확한 크기의 인공 치환물의 사용이 무엇보다도 중요하다.3,4) 인공 치환물의 크기를 결정함에 있어서 적절한 치환물의 전후 및 좌우 간격은 절제된 골 표면의 적절한 차폐를 통해서 슬관절 부하의 균등한 분배, 긴장이 적은 상처 봉합, 부드러운 슬개골 주 행에 있어서 중요하며, 특히 전후 간격은 굴곡 신전 간격과 대퇴 사두근의 적절한 긴장에 중요하다.5,6)
일반적으로 슬관절 전치환술은 여성에서 더 많이 시행되고 있 으며, 남성에서 여성보다 좀 더 좋은 결과를 보인다고 알려져 있 다.7,8) 이러한 결과를 바탕으로 다양한 원인에 대한 평가가 이루어 지고 있으며, 이 중 남성과는 다른 여성의 해부학적 구조에 대해 서도 최근 연구되고 있다. 즉, 여성의 경우 남성과는 다른 대퇴골 원위부 및 경골 근위부의 해부학적 특징을 가지고 있으며, 따라 서 남녀 공용 치환물을 사용할 경우 남성에 비하여 여성의 경우 적합하지 않은 경우가 많다는 보고도 있다.9) 현재까지는 주로 서 양인에서 대퇴골 원위부의 해부학적 차이에 대한 연구가 이루어 져 왔으며, 이를 바탕으로 서양 여성에서는 여성형 슬관절 치환
물이 더 적합하다고 보고되고 있다.10-17) 그러나 현재까지 한국인 의 대퇴골 원위부 및 경골 근위부 구조의 특징에 대해서는 알려 진 점이 거의 없다.
최근 한국 여성에서 대퇴골 원위부에 여성형 치환물을 사용할 경우, 기존의 남녀 공용 치환물을 사용하였을 때보다 부적절한 차폐(under-coverage)의 비율이 높다는 보고도 있다.18)
따라서 저자들은 본 연구를 통해 한국 여성에서 대퇴골 원위부 및 경골 근위부의 해부학적 특징에 대해서 분석하여, 남녀 간의 차이를 비교하고자 하였다.
대상 및 방법
1. 대상
2006년 10월부터 2007년 12월까지 슬관절 골관절염으로 RO- BODOC® (Integrated Surgical System, Sacramento, CA, USA)을 이 용하여 슬관절 전치환술을 시행받은 76명의 환자(여자: 50명, 남 자: 26명)를 대상으로 하였다. 평균 나이는 여성은 70.6세(범위, 51-80), 남성은 70.0세(범위, 58-84)였다.
2. 방법
모든 환자들은 슬관절 골관절염에 대해서 슬관절 전치환술을 시 행받았으며, ROBODOC을 이용한 슬관절 전치환술을 시행받 기 전 술 전 계획을 하기 위해서 컴퓨터 단층 촬영을 시행하였으 며, 이를 통해 0.625 mm의 간격으로 촬영된 축성 단면 영상들은 ORTHODOC® (Integrated Surgical System, Sacramento, CA, USA) 을 이용하여 3차원으로 재구성하였다.
재구성된 CT 영상에서 대퇴골과 경골의 역학적 축(mechani- cal axis)을 확인하고 회전축(rotational axis)은 대퇴골의 과상간 축 (transepicondylar axis)을 기준으로 하였고, 경골의 전후 축은 경골 결절의 내측 3분의 1과 후방십자인대의 기시부의 중심을 지나는 선을 기준으로 하였다.19) 모든 환자에서 슬관절 전치환술의 기본 술식에 따라 슬관절면 상방 9 mm에서 대퇴골 원위부를 역학적 축에 수직으로 절단하였으며, 경골 근위부는 대퇴골 원위부 절단 면과 평행하게 골 절제를 시행한 후, 절단면의 관상면, 시상면, 횡 단면에서 해부학적 지표의 길이를 ORTHODOC 프로그램을 이 용하여 측정하였다.
대퇴골 원위부의 해부학적 지표로서 대퇴골 외과 전후 길이 (anteroposterior length of lateral femoral condyle, LAP), Box의 좌 우 길이(mediolateral length of Box, Box ML), Flange의 좌우 길이
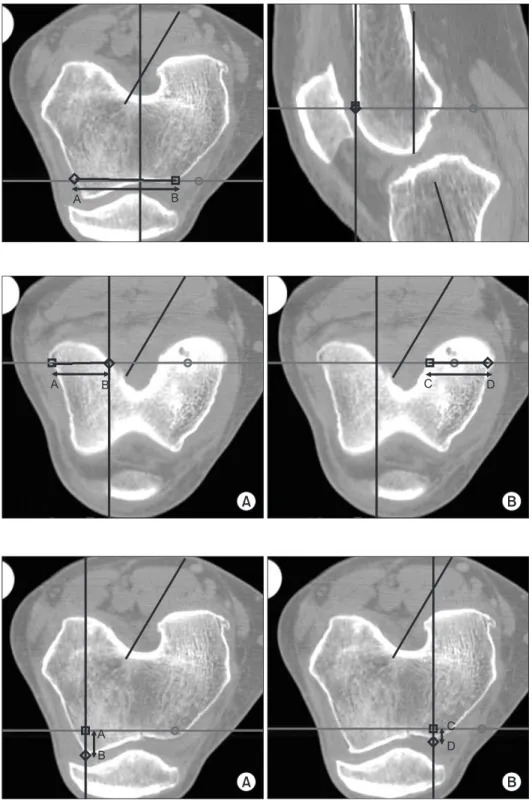
Figure 1. Measurement of the antero- posterior length of lateral femoral condyle, length of line AB and anteroposterior distance from anterior diaphyseal cortex to most posterior point of lateral femoral condyle.
Figure 2. Measurement of the mediolateral length of Box, length of line AB and mediolateral distance between most prominent points mediolaterally at the level of distal femoral cutting.
(mediolateral length of anterior flange, Flange ML), 대퇴골 외과 후 방 절단면 좌우 길이(mediolateral length of lateral femoral condyle, LCML), 대퇴골 내과 후방 절단면 좌우 길이(mediolateral length of medial femoral condyle, MCML), 대퇴골 외과 전방 절단면 전 후 길이(anterior height of lateral femoral condyle, LAH) 및 대퇴 골 내과 전방 절단면 전후 길이(anterior height of medial femoral condyle, MAH)를 ORTHODOC을 이용하여 측정하였으며, 각각 의 수치에 대한 비도 측정하였다. LAP (대퇴골 외과 전후 길이)는
과상간 축이 가장 긴 횡단면에서 대퇴골 외과의 최후방에서 대퇴 골 전방 절단면에 이르는 최단거리로 측정하였다(Fig. 1). Box ML (Box의 좌우 길이)은 ORTHODOC 프로그램을 통해서 planning 을 시행한 대퇴골 원위부의 절단면(level)에서 과상간축에 평행한 최장 거리를 측정하였다(Fig. 2). Flange ML (Flange의 좌우 길이) 은 planning 상 anterior flange와 anterior chamber가 만나는 곳의 내외측 간의 거리를 측정하였다(Fig. 3). LCML (대퇴골 외과 후방 절단면 좌우 길이)은 ORTHODOC 프로그램을 통하여 planning
Figure 3. Measurement of the mediolateral length of anterior flange, length of line AB and mediolateral distance at the junction of planned anterior femoral and chamber cut.
Figure 4. Measurement of the mediolateral length of lateral femoral condyle and mediolateral length of medial femoral condyle. (A) Length of line AB and mediolateral distance of lateral femoral condyle at the planned posterior femoral cut. (B) Length of line CD and mediolateral distance of medial femoral condyle at the planned posterior femoral cut.
Figure 5. Measurement of the anterior height of lateral femoral condyle and anterior height of medial femoral condyle.
(A) Length of line AB and anterior height of lateral femoral condyle at the planned anterior femoral cut. (B) Length of line CD and anterior height of medial femoral condyle at the planned anterior femoral cut.
을 시행한 대퇴골 원위부 외과 후방 절단면의 내외측간 거리를 posterior chamfer의 2분의 1 지점에서 측정하였다. MCML (대퇴 골 내과 후방 절단면 좌우 길이)은 LCML과 같은 방식으로 대퇴 골 원위부 내과 후방 절단면에서 측정하였다(Fig. 4). LAH (대퇴 골 외과 전방 절단면 전후 길이)는 planning을 시행한 대퇴골 원위 부 외과 전방 절단면(level)에서 대퇴골 외과 최전방까지의 수직 거리로 측정하였으며 MAH (대퇴골 내과 전방 절단면 전후 길이) 는 대퇴골 원위부 내과 전방 절단면에서 최전방까지의 수직거리
를 측정하였다(Fig. 5). 남성과 여성에서 해부학적 차이를 비교하 기 위해서는 앞에서 측정된 값만을 비교해서는 남성과 여성의 신 체적 차이를 정확히 비교하기 쉽지 않기 때문에 LAP에 대한 Box ML, MCML, LCML 및 Flange ML의 비를 계산하였다.
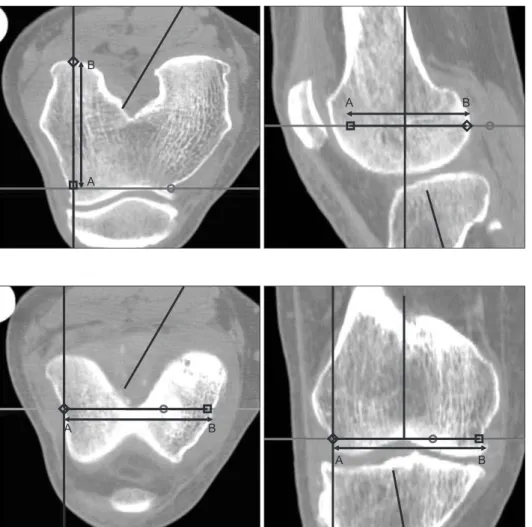
근위 경골의 해부학적 지표로서 경골 절단면에서 대퇴골의 과 상간 축과 평행한 최장 길이(mediolateral length of proximal tibia, ML), 좌우 길이의 중점에서 수직인 선의 전후 길이(middle an- teroposterior length of proximal tibia, AP)로 측정하였다(Fig. 6). 경 Figure 6. Measurement of the anterior height of middle of proximal tibia and mediolateral length of proximal tibia. (A) Length of line AB and anterior height of proximal tibia at the middle of longest mediolateral length. (B) Length of line CD and longest mediolateral length of proximal tibia parallel to the transepicondylar axis of distal femur at the planned anterior femoral cut.
Figure 7. Measurement of the anterior height of lateral and medial condyle of proximal tibia. (A) Length of line AB and anterior height of lateral tibial condyle at the planned tibial cut. (B) Length of line CD and anterior height of medial tibial condyle at the planned tibial cut.
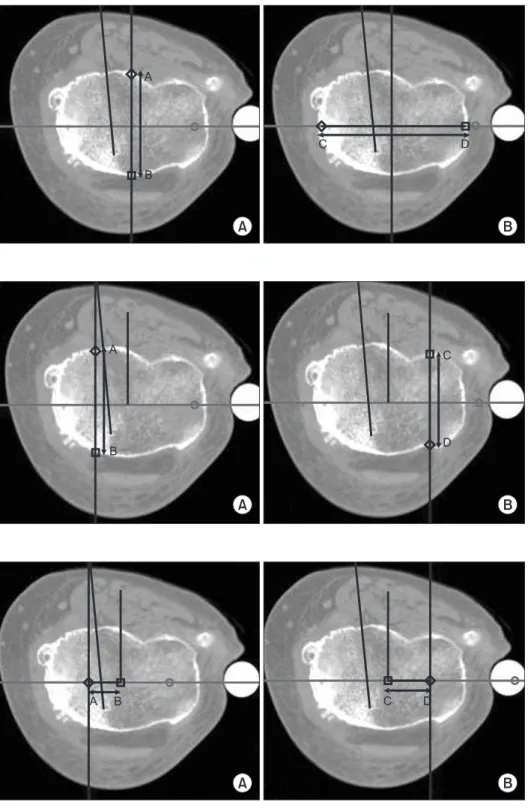
Figure 8. Measurement of the distance from the anterior height of lateral and medial condyle to the anterior height of middle of proximal tibia. (A) Length of line AB and distance from the line of CL to the line of AP at the planned tibial cut. (B) Length of line CD and distance from the line of CM to the line of AP at the planned tibial cut. CL, lateral to center distance;
AP, anteroposterior; CM, medial to center distance.
골 절단면에서 경골 외과의 전후 길이(anteroposterior length of lateral tibial condyle, LAP), 경골 절단면에서 경골 내과의 전후 길 이(anteroposterior length of medial tibial condyle, MAP)를 측정하 였다(Fig. 7). AP선으로부터 각각 LAP선까지 거리(lateral distance to center, CL), AP선으로부터 각각 MAP선까지 거리(medial dis- tance to center, CM)로 하였으며(Fig. 8), 추가적으로 전후 길이에 대한 좌우 길이의 비(Aspect ratio, %)를 계산하였다.2)
3. 통계학적 분석
SPSS 12.0 통계 프로그램(SPSS for Windows Release 11.0, Chicago, IL, USA)을 사용하여 통계학적 유의성을 검증하였는데, 남녀 두 군간의 비교는 독립표본 T 검정을 적용하였으며, 신뢰도는 95%
로 하였다.
결 과
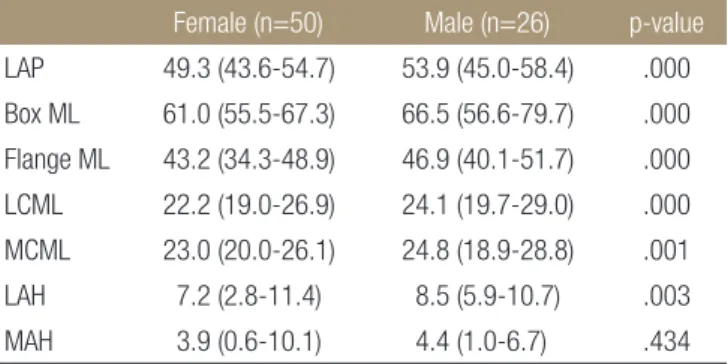
한국 여성에서 평균 대퇴골 외과 전후 길이(LAP)는 49.3 mm (범 위, 43.6-54.7)로 측정되었다. Box의 좌우 길이(Box ML), Flange의 좌우 길이(Flange ML)도 각각 61.0 mm (범위, 55.5-67.3), 43.2 mm (범위, 34.3-48.9)로 측정되었다. 이에 반해 남성의 경우 대퇴골 외 과 전후 길이(LAP), Box의 좌우 길이(Box ML), Flange의 좌우 길 이(Flange ML)는 53.9 mm (범위, 45.0-58.4), 66.5 mm (범위, 56.6- 79.7), 46.9 mm (범위, 40.1-51.7)로 여성의 경우보다 큰 지표를 나 타내었다(모두 p<0.001). 여성에서 대퇴골 외과 후방 절단면 좌우 길이(LCML), 대퇴골 내과 후방 절단면 좌우 길이(MCML)는 22.2 mm (범위, 19.0-26.9), 23.0 mm (20.0-26.1)로 측정되었으며, 남성 에서는 24.1 mm (범위, 19.7-29.0)와 24.8 mm (범위, 18.9-28.8)를 보였다(모두 p<0.001). 대퇴골 외과 전방 절단면 전후 길이(LAH) 는 여성과 남성에서 각각 7.2 mm (범위, 2.8-11.4)와 8.5 mm (범위,
5.9-10.7)로 여성에서 남성보다 작게 측정되었다(p=0.003). 반면 대퇴골 내과 전방 절단면 전후 길이(MAH)는 여성과 남성에서 3.9 mm (범위, 0.6-10.1), 4.4 mm (범위, 1.0-6.7)로 여성에서 작게 측정 되었으나 유의한 차이는 보이지 않았다(p=0.434) (Table 1).
또한, 대퇴골 외과 전후 길이(LAP)에 대한 Box의 좌우 길이 (Box ML), Flange의 좌우 길이(Flange ML), 대퇴골 외과 후방 절 단면 좌우 길이(LCML) 및 대퇴골 내과 후방 절단면 좌우 길이 (MCML) 지표 간의 비율에서는 두 군 간의 유의한 차이를 보이지 는 않았다(p=0.893, p=0.804, p=0.781, p=0.268) (Table 2).
근위 경골의 해부학적 지표에서도 전체적으로 여성의 경우 남 성보다 작게 측정되었다. 평균 ML은 여성과 남성에 있어 65.7 mm (범위, 57.9-71.8)과 70.7 mm (범위, 64.1-79.3)이었으며, AP 도 39.5 mm (범위, 33.4-49.2)와 41.9 mm (범위, 32.8-49.5)로 측정 되었다. 경골 근위부의 외측 및 내측 부분의 전후 길이를 측정하 는 LAP와 MAP도 여성에서는 40.8 mm (범위, 34.0-48.6), 43.1 mm (범위, 35.4-52.4)로, 남성의 경우 44.5 mm (범위, 40.4-50.3)와 49.8 mm (범위, 42.0-57.3)보다 작은 값을 보였다(모두 p<0.05). 하지만 경골 근위부에서 전후 길이(AP)에 대한 좌우 최대 길이(ML)의 비 율을 나타내는 Aspect ratio (%)는 여성과 남성에서 각각 166.8 (범 위, 122.8-192.8)과 169.6 (범위, 149.8-204.2)로 서로 간의 유의한 차이를 보이지는 않았다(p=0.33) (Table 3).
Table 1. Anatomic Characteristics of Distal Femur
Female (n=50) Male (n=26) p-value
LAP 49.3 (43.6-54.7) 53.9 (45.0-58.4) .000 Box ML 61.0 (55.5-67.3) 66.5 (56.6-79.7) .000 Flange ML 43.2 (34.3-48.9) 46.9 (40.1-51.7) .000 LCML 22.2 (19.0-26.9) 24.1 (19.7-29.0) .000 MCML 23.0 (20.0-26.1) 24.8 (18.9-28.8) .001 LAH 7.2 (2.8-11.4) 8.5 (5.9-10.7) .003 MAH 3.9 (0.6-10.1) 4.4 (1.0-6.7) .434 Average values are expressed in millimeters. LAP, anteroposterior of lateral femoral condyle; Box ML, mediolateral of Box; Flange ML, mediolateral of anterior flange; LCML, mediolateral of lateral femoral condyle; MCML, mediolateral of medial femoral condyle; LAH, anterior height of lateral femoral condyle; MAH, anterior height of medial femoral condyle.Table 2. Various Aspect Ratio in Male and Female Patients
Female (n=50) Male (n=26) p-value
Box ML/LAP 1.24 (1.11-1.31) 1.24 (1.11-1.47) .893 Flange ML/LAP 0.88 (0.66-1.03) 0.87 (0.71-1.02) .804 LCML/LAP 0.45 (0.38-0.51) 0.45 (0.39-0.50) .781 MCML/LAP 0.47 (0.43-0.53) 0.46 (0.39-0.53) .268 LAP, anteroposterior of lateral femoral condyle; Box ML, mediolateral of Box; Flange ML, mediolateral of anterior flange; LCML, mediolateral of lateral femoral condyle; MCML, mediolateral of medial femoral condyle.Table 3. Anatomic Characteristics of Proximal Tibia
Female (n=50) Male (n=26) p-value
ML 65.7 (57.9-71.8) 70.7 (64.1-79.3) .000 AP 39.5 (33.4-49.2) 41.9 (32.8-49.5) .004 LAP 40.8 (34.0-48.6) 44.5 (40.4-50.3) .000 MAP 43.1 (35.4-52.4) 49.8 (42.0-57.3) .000 CL 12.5 (6.8-20.3) 14.9 (9.5-22.2) .002 CM 10.5 (6.4-14.3) 11.9 (6.7-57.3) .001 Aspect ratio(=ML/AP) (%)
166.8 (122.8-192.8) 169.6 (149.8-204.2) .330
Average values are expressed in millimeters. ML, mediolateral; AP, anteroposterior; LAP, lateral anteroposterior; MAP, medial anteroposterior;
CL, lateral to center distance; CM, medial to center distance.
고 찰
한국 여성들의 경우 슬관절 골관절염의 높은 유병률을 보이고 있 으며,1) 현재 슬관절 전치환술을 시행받은 환자의 대부분도 여성 들이다. 일반적으로 인공 슬관절 치환물의 경우, 해부학적 형태 에 가장 적합하게 제작되어야 치환물과 골 절단면과의 적절한 차 폐를 이룰 수 있다. 부적절한 차폐나 치환물의 돌출로 인한 연부 조직의 불균형은 장기 추시상 좋지 않은 결과를 야기하는 것으로 보고되고 있다.9)
Hitt 등11)은 슬관절 전치환술을 시행받은 295명(여성: 188명, 남 성: 107명)의 환자를 대상으로 대퇴골 원위부의 해부학적 특징에 대하여 조사하였다. 그 결과 절제된 대퇴골 원위부 전후 길이를 기준으로 대퇴 치환물을 결정하면, 여성의 경우 대퇴골 원위부 좌우 길이가 남성의 경우보다 좁기 때문에 크기가 클 경우 좌우 로 치환물의 돌출이 발생하며, 대퇴골 원위부 크기가 작은 여성 에서는 치환물이 절단면을 다 차폐하지 못하는 것으로 보고하였 다.
최근 이러한 연구들을 바탕으로 여성형 슬관절이라는 치환물 이 출시되었으며, 이는 남녀 공용 대퇴골 치환물에 비하여 같은 전후 길이에 비해 좌우 길이가 좀 더 작게 제작되었다.2)
Lonner 등19)은 대퇴골 외과 전후 길이에 대한 과상간 길이 비교 에서 남녀 각각 1.23과 1.19로 두 군 간의 유의한 차이를 보고하였 으며, Poilvache 등20)도 대퇴골 원위부 외과와 내과의 전방 절단면 전후 길이 합(LAH+MAH)에 대한 과상간 길이(transepicondylar width, TEW)에 대한 비교에서 남녀 각각 1.34와 1.30으로 두 군 간 의 유의한 차이가 있다고 보고하였다. 이는 여성에 있어서 슬관 절 전치환술을 시행할 경우, 좌우 길이가 좀 더 작은 크기의 치환 물을 사용해야 치환물의 돌출을 막을 수 있다고 하였다. Chin 등21) 도 위와 비슷하게 남녀에 있어 대퇴골 원위부 전후 길이에 대한 좌우 길이는 각각 0.82와 0.79로 유의한 차이를 보인다고 보고하 였다. 그러므로 여성에 있어서 기존의 대퇴 치환물을 사용할 경 우, 전후 및 좌우 길이 간의 불균형을 초래할 수 있으며 따라서 치 환물의 돌출 및 이에 따른 불균등한 체중 부하 등으로 인해 조기 실패의 가능성이 높다고 하였다. 본 연구에서도 대퇴골 외과 전 방 절단면 전후 길이(LAH)는 여성에서 남성에 비하여 유의하게 작게 측정되었다(p=0.003). 이를 바탕으로 할 때 여성형 치환물의 anterior flange가 얇게 제작되었다는 점에서 장점이 있을 수 있겠 으나, 약 1.5 mm 이내의 차이를 보인다는 점에서 이에 대한 임상 적 의의에 대해서는 좀 더 많은 대상군을 바탕으로 한 연구가 필 요할 것으로 본다.
반면, Fehring 등10)은 212명(여성: 100명, 남성: 112명)의 환자 들의 슬관절 자기공명 영상을 바탕으로 대퇴골 외과 전방 절단 면 전후 길이(LAH), 내과 전방 절단면 전후 길이(MAH) 및 과상 간 길이(TEW)를 관절면의 10 mm 상방에서 측정하였다. 그 결과
외과 전방 절단면 전후 길이(LAH), 과상간 길이(TEW)의 경우 여 성에서 남성보다 통계학적으로 의미있게 작게 측정되었으나, 좌 우 길이에 대한 전후 길이의 비율인 Aspect ratio (=MAH or LAH/
TEW)의 경우 내측 또는 외측 모두에서 남녀 간의 유의한 차이를 보이지 않았다. 하지만 이러한 해부학적 보고는 대부분 서양인을 대상으로 한 것이며, 즉 한국인의 대퇴골 원위부의 해부학적 특 징에 대한 보고는 거의 없는 실정이다.
최근 Kim 등18)은 양측 슬관절 전치환술을 시행 받은 138명의 한국인 여성 환자를 대상으로 기존의 대퇴 치환물과 여성형 슬 관절 치환물에 따른 수술 중 대퇴골 원위부의 해부학적 구조와 의 적합성에 대하여 조사하였다. 기존의 대퇴 치환물의 경우 80 예(58%)에서 전후 및 좌우 길이가 절제된 대퇴골 원위부와 잘 맞 는 것으로 조사되었으나, 여성형 슬관절 치환물의 경우 단지 15예 (10.9%)만 적절한 차폐를 이루었다. 반면, 여성형 슬관절의 경우 123예(89%)에서 대퇴골 원위부에 비하여 부적절한 차폐(under- coverage)를 보였다.
따라서 본 연구를 통하여 대퇴골 원위부 및 경골 근위부의 다 양한 해부학적 지표를 측정하려고 하였으며, 서로 간의 상관관계 를 밝히는 데 주안점을 두었다.
슬관절 전치환술에 필요한 해부학적 지표들의 측정에 대해서 는 다양한 방법들이 알려져 있으며, 가장 흔히 사용되는 방법 중 하나는 수술 중 측정하는 것이다.11) 본 연구에서는 컴퓨터 단층 촬영을 통해 얻은 술 전 3차원 영상을 바탕으로 각각의 지표들에 대하여 ORTHODOC 프로그램을 이용하여 측정하였다. 컴퓨터 단층 촬영을 통하여 측정함으로써 수술 중 측정하는 것보다 오 차를 줄일 수 있었으며, 대퇴골 원위부와 경골 근위부의 회전축 을 정확히 맞춘 후 원하는 차원의 영상에 대하여 다양한 값을 측 정할 수 있었다. 또한, 치환물의 적절한 크기 및 돌출 예방에 중요 한 지표인 대퇴골 외과 전후 길이(LAP)를 측정 가능케 하였으며, Box의 좌우 길이(Box ML)를 측정함으로써 골 절단면과 치환물 사이의 접촉면적에 대해서도 분석 가능케 하였다.
일반적으로 대퇴골 원위부의 경우, 여성이 남성보다 전후 길 이 및 좌우 길이 모두 작은 것으로 조사되었다. 이는 기존의 서양 인 여성을 대상으로 한 것과 비슷한 결과를 보이고 있으나, 전후 및 좌우 길이의 비율을 측정한 지표에서는 남녀 간 유의한 차이 를 보이지 않았으며, 즉, 한국인 여성의 경우 남성에 비하여 대칭 적으로 작은 해부학적 구조를 가지고 있다고 해석할 수 있다. 이 는 서양 여성의 경우, 전후 및 좌우 길이의 비대칭적인 비율로 인 하여 여성형 슬관절 치환물을 사용해야 하는 것과는 다르며, 기 존의 남녀 공용 치환물 중 작은 크기를 사용함으로써 충분히 적 절한 차폐 및 돌출을 방지할 수 있다는 것을 의미한다.
대부분의 해부학적 지표는 술 전 ORTHODOC 프로그램을 이 용하여 계획된 절단면을 바탕으로 측정되었기에 치환물에 영향 을 받지 않고 측정될 수 있었다. 다만, MCML과 LCML의 경우에
는 술 전 계획과 다른 크기의 치환물이 삽입될 경우 술 후 다르게 측정될 수 있다는 점은 본 연구의 제한점 중 하나이다. 그 외 술 전 영상을 통해 측정함으로써 퇴행성 변화에 따른 골극 형성 등 으로 정확한 수치의 측정이 어려웠을 수 있다는 점과, 여성군에 비하여 남성군의 대상 수가 부족했다는 점을 들 수 있다.
하지만 이전 연구에서는 대퇴골 원위부 및 경골 근위부의 해부 학적 특징을 분석하기 위해 일반인 또는 사체를 대상으로 하였으 나, 본 연구에서는 슬관절 골관절염으로 인해 슬관절 전치환술을 받은 환자군을 대상으로 하였기에 임상적으로 더 큰 의의가 있으 며, 일반적으로 여성에서 관절염으로 인해 슬관절 전치환술을 많 이 받기 때문에 본 연구에서도 일정 기간 동안에 남성 환자의 수 가 부족할 수밖에 없었다. 더욱이 본 연구에서는 컴퓨터 단층 촬 영을 통해 얻어진 자료를 바탕으로 측정하였기에, 과거 단순 방 사선 촬영, 자기 공명 영상(MRI) 및 수술 중 측정한 방법에 비하 여 정확도가 높다는 장점이 있다.
결 론
본 연구를 통하여 한국 여성의 경우 대퇴골 원위부의 해부학적 크기가 남성보다 작은 것을 확인할 수 있었으나, 측정된 수치들 간의 비율에 있어서는 남녀 간에 큰 차이를 보이지는 않았다. 마 찬가지로 근위 경골의 해부학적 지표에 있어서도 남녀 간의 차이 는 존재하였으나, 전후 및 좌우 비율에 있어서는 대칭적인 양상 을 보임을 알 수 있었다. 최근 사용하고 있는 여성형 슬관절 치환 물의 경우 전후 길이에 대하여 좌우 길이가 남녀 공용 치환물에 비하여 작게 제작되었다는 점을 고려할 때, 한국 여성에서는 서 양인과 달리 여성형 슬관절 치환물의 사용이 필요치 않다는 것을 알 수 있다.
참고문헌
1. Hootman JM, Sniezek JE, Helmick CG. Women and arthritis:
burden, impact and prevention programs. J Womens Health Gend Based Med. 2002;11:407-16.
2. Kwak DS, Surendran S, Pengatteeri YH, et al. Morphometry of the proximal tibia to design the tibial component of total knee arthroplasty for the Korean population. Knee. 2007;14:295- 300.
3. Kane RL, Saleh KJ, Wilt TJ, Bershadsky B. The functional outcomes of total knee arthroplasty. J Bone Joint Surg Am.
2005;87:1719-24.
4. Roberts VI, Esler CN, Harper WM. A 15-year follow-up study of 4606 primary total knee replacements. J Bone Joint Surg Br.
2007;89:1452-6.
5. Vaidya SV, Ranawat CS, Aroojis A, Laud NS. Anthropometric measurements to design total knee prostheses for the Indian population. J Arthroplasty. 2000;15:79-85.
6. Bengs BC, Scott RD. The effect of patellar thickness on in- traoperative knee flexion and patellar tracking in total knee arthroplasty. J Arthroplasty. 2006;21:650-5.
7. Parsley BS, Bertolusso R, Harrington M, Brekke A, Noble PC.
Infl uence of gender on age of treatment with TKA and func- tional outcome. Clin Orthop Relat Res. 2010;468:1759-64.
8. Vincent KR, Vincent HK, Lee LW, Alfano AP. Outcomes in total knee arthroplasty patients after inpatient rehabilita- tion: influence of age and gender. Am J Phys Med Rehabil.
2006;85:482-9.
9. Conley S, Rosenberg A, Crowninshield R. The female knee:
anatomic variations. J Am Acad Orthop Surg. 2007;15 Suppl 1:31-6.
10. Fehring TK, Odum SM, Hughes J, Springer BD, Beaver WB Jr.
Diff erences between the sexes in the anatomy of the anterior condyle of the knee. J Bone Joint Surg Am. 2009;91:2335-41.
11. Hitt K, Shurman JR 2nd, Greene K, et al. Anthropometric measurements of the human knee: correlation to the sizing of current knee arthroplasty systems. J Bone Joint Surg Am.
2003;85-A Suppl 4:115-22.
12. Dalury DF, Mason JB, Murphy JA, Adams MJ. Analysis of the outcome in male and female patients using a unisex total knee replacement system. J Bone Joint Surg Br. 2009;91:357-60.
13. MacDonald SJ, Charron KD, Bourne RB, Naudie DD, Mc- Calden RW, Rorabeck CH. The John Insall Award: gender- specifi c total knee replacement: prospectively collected clini- cal outcomes. Clin Orthop Relat Res. 2008;466:2612-6.
14. Merchant AC, Arendt EA, Dye SF, et al. The female knee:
anatomic variations and the female-specifi c total knee design.
Clin Orthop Relat Res. 2008;466:3059-65.
15. Greene KA. Gender-specifi c design in total knee arthroplasty.
J Arthroplasty. 2007;22(7 Suppl 3):27-31.
16. Clarke HD, Hentz JG. Restoration of femoral anatomy in TKA with unisex and gender-specific components. Clin Orthop Relat Res. 2008;466:2711-6.
17. Emerson RH Jr, Martinez J. Men versus women: does size matter in total knee arthroplasty? Clin Orthop Relat Res.
2008;466:2706-10.
18. Kim YH, Choi Y, Kim JS. Comparison of standard and gender-specifi c posterior-cruciate-retaining high-fl exion total knee replacements: a prospective, randomised study. J Bone
Joint Surg Br. 2010;92:639-45.
19. Lonner JH, Jasko JG, Thomas BS. Anthropomorphic differ- ences between the distal femora of men and women. Clin Orthop Relat Res. 2008;466:2724-9.
20. Poilvache PL, Insall JN, Scuderi GR, Font-Rodriguez DE. Ro-
tational landmarks and sizing of the distal femur in total knee arthroplasty. Clin Orthop Relat Res. 1996;(331):35-46.
21. Chin KR, Dalury DF, Zurakowski D, Scott RD. Intraoperative measurements of male and female distal femurs during pri- mary total knee arthroplasty. J Knee Surg. 2002;15:213-7.
Anatomic Characteristics of the Distal Femur and the Proximal Tibia in Koreans Undergoing Total Knee Arthroplasty
Geon Woo Lee, M.D.*, Eun-Kyoo Song, M.D., Ph.D., Jong-Keun Seon, M.D., Dong Hyun Lee, M.D.*, and Tae Min Lee, M.D.*
Center for Joint Disease, Chonnam National University Hwasun Hospital, Hwasun,
*Department of Orthopaedic Surgery, Chonnam National University Hospital, Gwangju, Korea
Purpose: In this study, we examined the anatomic characteristics of the distal femur and the proximal tibia to determine if there
were signifi cant differences between male and female patients.Materials and Methods: Seventy six patients (50 of female, 26 of male) who were treated by total knee arthroplasty using
ROBODOC®, were included. The anteroposterior and mediolateral length of the distal femur and proximal tibia were checked using the ORTHODOC program.Results: The mean sizes of the distal femur and proximal tibia of female knees were slightly smaller than those of male knees.
Statistically signifi cant differences were observed between the two groups (p<0.05 for all). On the other hand, the anteroposterior and mediolateral ratios of distal femur and proximal tibia revealed no differences between female and male knees (p>0.05 for all).
Conclusion: The anteroposterior to mediolateral ratio was similar in the distal femur and proximal tibia of Korean females.
Key words: knee, femur, tibia, anatomy, Korea, female
Received December 22, 2010 Accepted May 23, 2011 Correspondence to: Eun-Kyoo Song, M.D., Ph.D.
Department of Orthopedic Surgery, Center for Joint Disease, Chonnam National University Hwasun Hospital, 160, Ilsim-ri, Hwasun 519-809, Korea