Congenital cervicothoracic kyphoscoliosis is usually progressive and the disorder is not affected by conserva- tive treatment. Progression of this deformity may lead to paraplegia and cardiopulmonary dysfunction (1). A combined anterior-posterior approach is required to cor- rect severe kyphoscoliosis (2). However, surgery is tech- nically challenging as congenital kyphoscoliotic defor- mities are mostly accompanied by vascular abnormali- ties. Intraoperative complications of the anterior cervi-
cal decompression mainly include neurovascular in- juries involving the nerve root, the spinal cord, and the vertebral artery (3, 4). Especially in pediatric patients, the safety of cervical pedicle screw fixation has not yet been established.
Computed tomography angiography (CTA) has been frequently used to evaluate the vascular anatomy (5).
One major advantage of the use of CTA in comparison to conventional angiography is the ability to obtain mul- tiplanar reconstructed images (6). Multidetector CTA (MDCTA) provides higher resolution, three-dimensional vascular imaging as well as excellent bone and soft tis- sue spatial relationships with short breath-hold duration (7, 8). We present the role of MDCTA in surgical plan- ning for congenital cervicothoracic kyphoscoliosis.
The Role of Multi-detector CT Angiography in Surgical Planning for Congenital Cervicothoracic
Kyphoscoliosis: A Case Report1
Hyun Lee, M.D., Won Gyu Choi, M.D.2, Ho-Dong Shin, M.D.2, Byeong Wook Hwang, M.D.2, Sang Jin Lee, M.D.2, Sang-Ho Lee, M.D.2
1Department of Diagnostic Radiology, Busan Wooridul Spine Hospital
2Department of Neurosurgery, Busan Wooridul Spine Hospital
This study was supported by a grant from the Wooridul Spine Foundation Received August 17, 2007 ; Accepted November 9, 2007
Address reprint requests to : Sang-Ho Lee, M.D., Ph.D., Department of Neurosurgery, Busan Wooridul Spine Hospital, Hubsky WIAA Bldg. 13F.
153-8 Oncheon-1-dong, Dongrae-gu, Busan 607-831 Korea
Tel. 82-51-559-2260 Fax. 82-51-559-2295 E-mil: [email protected]
Surgical correction of a cervicothoracic deformity is difficult with a potential risk of vascular injury. Comprehensive preoperative vascular evaluation is important for safe and successful surgery. The use of multi-detector computed tomography angiography (MDCTA) allows a combined display of vascular and osseous structures of the muscu- loskeletal system. However, no clinical reports have described the use of MDCTA for surgical planning of anterior cervicothoracic surgery in patients with vascular malfor- mation. The case of a 7-year-old girl with congenital cervicothoracic kyphoscoliosis who underwent preoperative MDCTA evaluation and successful correction is present- ed in this report.
Index words :Spine Kyphosis
Computed tomography (CT) X-Ray
Angiography Spinal Fusion Child
Musculoskeletal
Case Report
A 7-year-old Turkish girl with congenital cervicotho- racic kyphoscoliosis was admitted to our hospital for surgical treatment. The patient complained of neck pain and frequent respiratory difficulty and could not lie on her back during sleep because of a posterior neck
‘hump’. A plain radiograph showed severe kyphoscolio- sis at the cervicothoracic junction (Fig. 1). T2WI MR and an MR myleogram showed a focal myelopathy with spinal cord compression at the gibbus deformity level (Fig. 2). A CT examination was performed using a 16-de- tector-row CT scanner (Brilliance Philips Medical Systems, Cleveland, OH USA). To evaluate the variabili- ty of the vertebral artery, CTA was performed from the aortic arch to the vertex with 0.5 s gantry rotation speed, 0.75 mm collimator width, 22.5 mm/s table feed/rota-
tion, pitch 0.938, and a reconstruction increment of 0.5 mm. An 18-gauge IV cannula was inserted in the right femoral vein. A high iodine concentration contrast agent, Ultravist (70 mg of iodine/mL; Schering AG, Berlin, Germany) (30 mL) was injected at the rate of 4mL/s. To optimize the enhancement of the arterial ves- sel and to avoid venous superimpositions, we used a test-bolus approach. The standard scan start delay (10 seconds) was calculated from the peak maximum en- hancement at the level of the aortic arch. Arterial-phase images were obtained with caudocranial data acquisi- tion. Following the application of the volume-rendering (VR) algorithm, the staff physicians performed image analysis in real-time.
An abnormal course of the vertebral artery was con- firmed by MDCTA. The left vertebral artery ascended towards the C4 defective transverse foramen, while the right vertebral artery ascended towards the C6 defective
A B
Fig. 1. Preoperative plain anteroposte- rior (A) and lateral radiographs (B) demonstrate left-side scoliosis and se- vere kyphosis at the cervicothoracic junction.
A B C
Fig. 2. A. Sagittal T2WI MR shows that the spinal cord is markedly stretched and angled at the apex of the deformity.
B. An axial T2WI MR shows spinal cord compression and a suspicious myelopathy at the gibbus deformity level.
C. An MR myelogram shows nearly complete block of thecal sac at the level of dysgenesis.
transverse foramen (Fig. 3). The reformatted 3D VR im- ages showed the detail of the malformed cervicothoracic junction with spina bifida of C5 (Fig. 4A). A large inter- vening misshapen C6-T3 body mass was confirmed on the sagittal multiplanar reformation CT images (Fig. 4B).
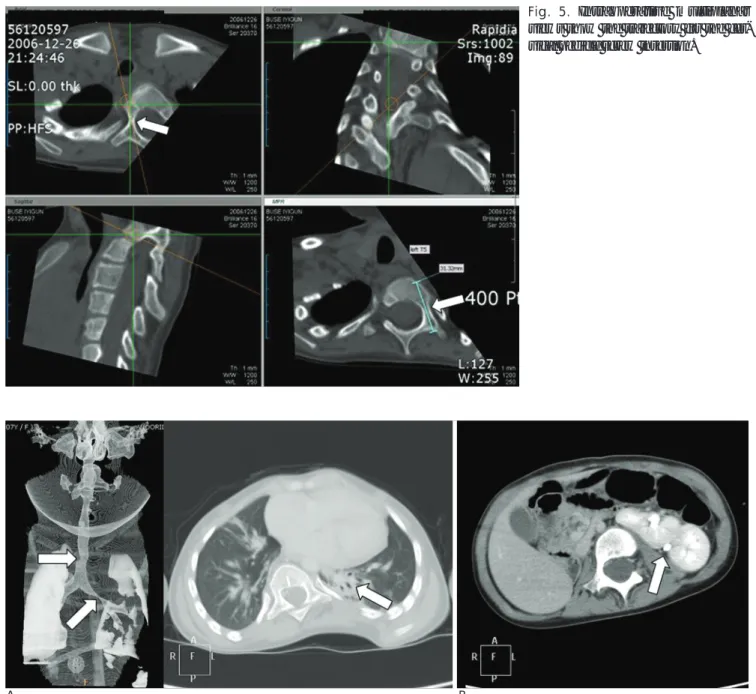
Preoperative multiplanar CT reconstruction of the pedi- cle anatomy was performed for cervicothoracic pedicle screw fixation (Fig. 5). A chest CT revealed congenital stenotic areas in the trachea and left main stem bronchus with parenchymal consolidations in the left
lobe (Fig. 6A). The patient also had kidneys with double ureters (Fig. 6B).
We performed combined anterior-posterior-anterior surgery. The spinal cord was decompressed by perform- ing an anterior release with a resection of the dysgenesis segment. Then, pedicle screws were successfully insert- ed into the pedicles in the cervicothoracic level. Finally, anterior reconstruction using an allograft with anterior plating from C3 to T5 was performed (Fig. 7). There were no iatrogenic neurologic or vascular injuries.
A
B
C
Fig. 3. Volume rendered 3D images of CTA. A. The anteroposterior view shows the course of the vertebral arteries.
B. Left lateral oblique images show the left vertebral artery running towards the C4 defective transverse foramen.
C. Right lateral oblique images show that the right vertebral artery running towards the C6 defective transverse foramen.
A B
Fig. 4. A. The reformatted 3D volume rendering images demonstrate that the C5 spinous process is split, the left lamina of C6 ver- tebra is dysplastic, its right lamina is fused to C7 vertebra, and the vertebral body from T1 to T3 was fused.
B. The sagittal multiplanar reformation CT images demonstrate a large intervening misshapen C6-T3 body mass (arrow).
Discussion
Vertebral artery laceration is a rare, but serious com- plication of anterior cervical decompression (9). Once laceration occurs during surgery, hemorrhage is difficult to control. Therefore, comprehensive preoperative eval- uation of the vascular anatomy is essential to conduct safe and successful surgery.
Although CTA provides high-resolution images, a large number of images for the diagnosing physician to
review are generated. It also is difficult to use for the identification of veins versus arteries. With recent ad- vances in CT technology, MDCTA has been becoming increasingly popular to use for preoperative vascular evaluation (7, 8). The VR technique is a useful tool to vi- sualize 3D clinical images. Using the VR technique, a true 3D display accurate to each pixel in the data-set can be generated. Depending on the clinical question, a vol- umetric 3D image can be generated in real time, focus- ing on the soft tissue, bone, or vascular structures.
Postoperative reviews of patients with orthopedic hard-
A B
Fig. 6. Combined anomalies.
A. A congenital focal tracheal stenosis and left mainstem bronchus stenosis with parenchymal consolidations in the left lobe, which might be the cause of the asthma.
B. Left-sided kidneys with double ureters.
Fig. 5. Intraoperative multiplanar views show the trajectory for the cer- vical pedicle screw insertion.
ware can also be more effective as the use of 3D VR eliminates the vast majority of streak artifacts and clear- ly delineates the relationship between hardware and bone (10).
In our case, the VR algorithm gave a comprehensive overview of the course and caliber of the vertebral arter- ies (Fig. 3). A reformatted 3D VR image demonstrated that the C6 vertebra had a dysplastic left lamina and a right lamina fused to the adjacent C7, spina bifida of C5 and multiple level posterior fusion of T1, T2, and T3 (Fig. 4A). After the surgeons had the detailed spatial re- lationships between the malformed vertebral arteries and the misshapen vertebral bodies, they could safely perform anterior cervical decompression and posterior stabilization.
In conclusion, volume rendered MDCTA is a valuable noninvasive technique for surgical planning of congeni- tal cervicothoracic kyphoscoliosis to prevent vertebral artery injury.
Acknowledgements
The authors warmly thank Song-Woo Shin, In-Kyeong Ha, and Eun-Hee Park for their help in preparing the manuscript and figures.
References
1. Winter RB, Moe JH, Wang JF. Congenital kyphosis: its natural his- tory and treatment as observed in a study of one hundred and thir-
ty patients. J Bone J Surg Am 1973;55:223-256
2. Smith JT, Gollogly S, Dunn HK. Simultaneous anterior-posterior approach through a costotransversectomy for the treatment of congenital kyphosis and acquired kyphoscoliotic deformities. J Bone Joint Surg Am 2005;87:2281-2289
3. Schwartz DM, Sestokas AK, Hilibrand AS, Vaccaro AR, Bose B, Li M, et al. Neurophysiological identification of position-induced neurologic injury during anterior cervical spine surgery. J Clin Monit Comput 2006;20:437-444
4. Burke JP, Gerszten PC, Welch WC. Iatrogenic vertebral artery in- jury during anterior cervical spine surgery. Spine J 2005;5:508-514 5. Datta JC, Janssen ME, Beckham R, Ponce C. The use of computed
tomography angiography to define the prevertebral vascular anatomy prior to anterior lumbar procedures. Spine 2007;32:113- 119
6. Lell M, Wildberger JE, Heuschmid M, Flohr T, Stierstorfer K, Fellner FA, et al. CT-angiography of the carotid artery: first results with a novel. 16-slice-spiral-CT scanner. Rofo 2002;174:1165-1169 7. Schertler T, Wildermuth S, Teodorovic N, Mayer D, Marincek B,
Boehm T. Visualization of congenital thoracic vascular anomalies using multi-detector row computed tomography and two- and three-dimensional post-processing. Eur J Radiol 2007;61:97-119 8. Chan FP, Rubin GD. MDCT angiography of pediatric vascular dis-
eases of the abdomen, pelvis, and extremities. Pediatr Radiol 2005;35:40-53
9. Smith MD, Emery SE, Dudley A, Murray KJ, Leventhal M.
Vertebral artery injury during anterior decompression of the cervi- cal spine. A retrospective review of ten patients. J Bone Joint Surg Br 1993;75:410-415
10. Calhoun PS, Kuszyk BS, Heath DG, Carley JC, Fishman EK.
Three-dimensional volume rendering of spiral CT data: theory and method. Radiographics 1999;19:745-764
A B
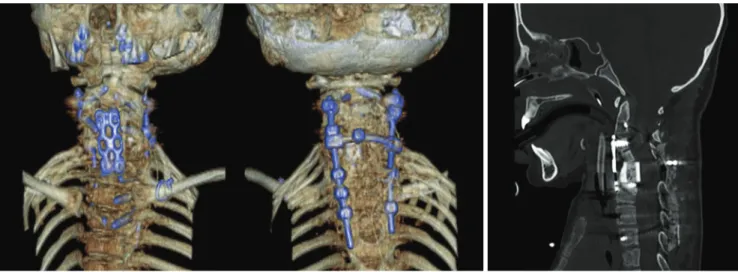
Fig. 7. A. Reformatted 3D volume-rendered images after surgery show the elimination of the vast majority of streak artifacts and clearly delineate the relationship between hardware, bone, and bone fragments.
B. A sagittal multiplanar reformation CT image shows the reconstructed and stabilized cervicothoracic junction after surgery.
대한영상의학회지 2008;58:91-96
선천성 경흉추 후측만증 교정술에서의 MDCT 혈관 조영술의 역할: 증례 보고1
1부산우리들병원 영상의학과
2부산우리들병원 신경외과
이 현・최원규2・신호동2・황병욱2・이상진2・이상호2
경흉추 후측만증 교정술은 혈관 손상의 위험을 내포한다. 안전하고 성공적인 수술을 시행하려면 종합적인 술전 혈관 평가가 중요하다. 다검출기 CT(MDCT) 혈관 조영술은 근골격계의 혈관과 골구조를 복합적으로 보여주나, 혈 관기형을 동반한 환자에서 전방경유 경흉추부 수술시 수술 계획 수립을 위한 MDCT 혈관 조영술의 활용에 관한 보고는 없었다. 본 논문은 선천성 경흉추 후측만증의 7세 여아에서 MDCT 혈관 조영술로 술전 평가를 시행하여 추 골동맥 기형을 파악하고 성공적인 교정술을 시행할 수 있었던 증례를 보고하고자 한다.