Fluorine-18 2-fluoro-2-deoxy-d-glucose (18F-FDG) positron emission tomography (PET) has been used ex- tensively for the diagnosis of various malignancies with high rates of sensitivity and specificity (1). This imaging technique is based on the identification of the increased glycolysis that occurs in malignant cells. FDG is prefer- entially concentrated in the malignant cells due to an in- crease in the number of membrane glucose transporter proteins known as the GLUT transporters in the tumor cells.
In a mechanism similar to glucose, FDG is subse- quently phospholylated by hexokinase to FDG 6- phos- phate. FDG 6-phosphate is not efficiently metabolized, and therefore is trapped within the cell (2). Because of increased metabolic activity, most lung malignancies have a threshold standardized uptake value of 2.5, rep- resenting a much greater FDG uptake than found in
normal tissues (2). According to a recent meta-analysis, the estimated sensitivity of PET for identifying a malig- nant pulmonary lesion is 96.8% and its specificity is 77.8% (3).
However, increased FDG uptake is not always limited to malignant tissues, and it is well recognized that in- flammation may lead to FDG accumulation of macrophages and other activated inflammatory cells.
Moreover, the development of the PET/CT scanner al- lows for the simultaneous acquisition of both anatomic and functional data and reassessment of biological distri- bution patterns of physiological tracers. Thus, PET/CT can improve image interpretation and can have an im- pact on the diagnostic and therapeutic aspects of patient management (4).
In this report, we demonstrate the physiological FDG uptake of normal structures, and describe normal vari- ant and iatrogenic FDG activity using PET/CT imaging and review various benign pathological conditions with standardized uptake values (SUV) greater than 2.5 in the thorax.
Non-Malignant 18F-FDG Uptake in the Thorax by Positron Emission Tomography Computed
Tomography Fusion Imaging
1Hyun Jin Park, M.D., Ie Ryung Yoo, M.D., Ho Jong Chun, M.D., Sun Wha Song, M.D., Soo Ah Im, M.D., Seog Hee Park, Sung Hoon Kim, M.D., Kyo-young Lee, M.D.2
1Department of Radiology, 2Department of Pathology, Kangnam St. Mary’s Hospital
Received March 12, 2007 ; Accepted May 30, 2007
Address reprint requests to : Sung Hoon Kim, M.D., Department of Radiology, Kangnam St. Mary’s Hospital, 505, Banpo-dong, Seocho-gu, Seoul 137-704, Korea
Tel. 82-2-590-2467 Fax. 82-2-599-6771 E-mail: [email protected]
Fluorine-18 2-fluoro-2-deoxy-D-glucose (18F-FDG) positron emission tomography (PET) has been used exclusively to diagnose malignancies. However, increased FDG uptake is not always limited to malignant tissue. Many false positive findings for PET have been reported. Moreover, the use of PET/CT may allow the reassessment of pre- viously recognized patterns of physiological bio-distribution of a tracer. In this report we demonstrate the physiological FDG uptake of normal structures in the thorax using PET/CT imaging and illustrate many benign pathological conditions with standardized uptake values greater than 2.5.
Index words :Positron emission tomography (PET) Thorax
Normal whole body FDG distribution
For whole body PET examinations, performed be- tween 1 and 2 hours after IV administration of FDG, the brain, heart and urinary tract are the most prominent sites of tracer accumulation. The brain, an obligate user of glucose, typically shows high uptake of FDG in the cortices, thalami and basal ganglia. Cortical activity may be reduced in patients under sedation or general anes- thetic. The myocardium has similar FDG avidity in the fed state as the brain. FDG follows the urinary excretory route and it will be present in the bladder and to varying degrees in the upper urinary tract (5).
Elsewhere, tracer activity is distributed at low levels in recognizable anatomic structures on attenuation-cor-
A B
Fig. 2. Uptake in the supraclavicular area fat (“USA-fat”). A 35-year old woman with breast cancer was evaluated after a mastecto- my and chemotherapy.
(A and B) PET/CT (A) and non-contrast CT (B) clearly reveal the location of the bilateral FDG uptake to be the fatty tissue of the supraclavicular regions, and not the lymph nodes (peak-SUV 3.7, arrows).
Fig. 1. Normal whole body FDG distribution.
The brain, heart and urinary tract are the most prominent sites of tracer accumulation, one hour after IV administration of FDG.
A B
Fig. 3. FDG uptake in brown adipose tissue in a 42-year-old woman with breast cancer after breast conserving surgery.
(A and B) Axial images of PET/CT (A), and non-contrast CT (B) obtained at the level of the aortic arch show increased FDG uptake in the right prevascular space of the mediastinum (peak-SUV 4.5, arrow), localized to the adipose tissue.
rected images. In the neck, it is common to see moder- ate symmetrical activity in the tonsillar tissues. The ade- noidal tissue is not usually perceptible in adults but may show noticeable uptake in children. FDG activity associ- ated with the laryngeal musculature or thyroid tissue is frequently seen. In the chest, there is variation in the lung regions, being greater in the inferior and posterior segments. In the abdomen, homogeneous, low-grade ac-
cumulations are seen in the liver and spleen. Small and large bowel activities are quiet variable. The bone mar- row is normally associated with FDG accumulation at levels higher than blood pool activity, and vertebral bod- ies are therefore consistently identified, as well as other major marrow containing skeletal structures such as the pelvis, hips and sternum (6).
The normal distribution of FDG is shown in Figure 1.
A
B
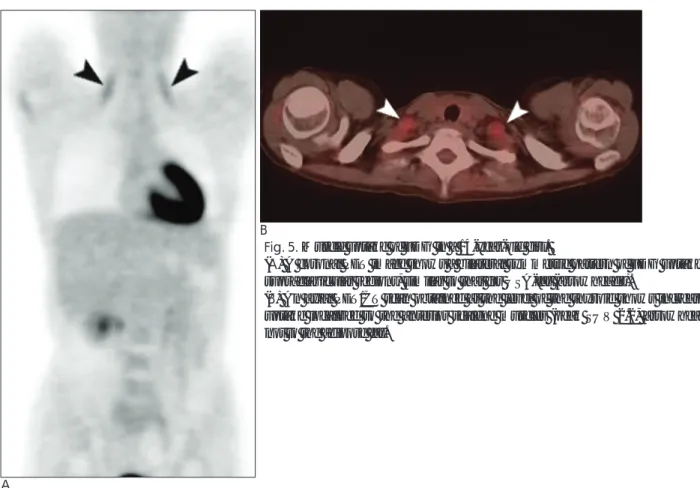
Fig. 5. Muscle uptake of FDG in a 14-year-old girl.
(A) A coronal PET image shows a bilateral symmetric pattern of FDG uptake in both supraclavicular regions, similar to that for USA-fat (arrowheads).
(B) An axial PET/CT scan obtained at the level of the thyroid shows increased FDG uptake localized to the anterior scalene muscles (peak SUV 2.2, arrowheads), and not to the adipose fat.
A B
Fig. 4. Normal FDG uptake in the thymus of a 16-year-old boy.
(A and B) Axial images of PET/CT (A) and non-contrast CT (B) show an inverted V-shaped area of anterior mediastinal uptake (peak SUV 2.7, arrows), corresponding to the thymus. In young patients, the thymus is normally associated with moderate FDG uptake. Given the morphological features, this finding is typical of normal thymic uptake.
Normal Variant FDG Distribution in the Thorax
FDG uptake depicts tissue glucose metabolism.
Hence, in addition to the abnormal glucose metabolism associated with a malignant neoplasm, FDG PET/CT re- veals normal variations in glucose metabolism. Some of the normal variations may mimic pathological processes (5, 6).
Brown Adipose Tissue
Increased FDG uptake in the supraclavicular regions is well known, and is called “USA-fat”. It was thought to be attributed to muscular uptake. However, PET/CT im- ages subsequently proved that these foci of FDG uptake were localized to adipose tissues rather than to muscles (Fig. 2). Increased FDG uptake by fat is visible in the paraspinal area, mediastinum, and upper abdomen as well as the neck (Fig. 3). This FDG uptake can be ex- plained by non-shivering thermoregulation that involves a direct increase in glucose uptake by brown adipose tis- sue caused by increased sympathetic nervous system activity and the need for glucose continuing the process
of lipolysis (7).
Thymus
An increase in FDG uptake can be seen in normal thymic tissue in pediatric and adult patients, and the de- gree of FDG uptake by the thymus overlaps the values of thymic hyperplasia and neoplasia (8). The characteris- tic shape (an inverted V or Y), facilitates the differentia- tion from other anterior mediastinal tumors (Fig. 4) (6).
Skeletal Muscle
At rest, skeletal muscles rely on fatty acid oxidative metabolism for energy. However, with increased ener- gy demand, glycolysis becomes the major source of en- ergy for the skeletal muscles. Skeletal muscles in active contraction and tension demonstrate elevated FDG ac- cumulation (Fig. 5). Additionally, insulin increases mus- cle uptake of glucose (Fig. 6) (5).
Non-malignant Pathological Uptake in the Thorax
Inflammatory cells such as lymphocytes, neutrophils, and macrophages have increased glucose utilization, and increased FDG uptake has been reported in various inflammatory and infectious lesions (9).
Although FDG uptake in infectious and inflammatory lesions can increase the number of false-positive results and reduce the specificity of PET that is performed for oncology examinations, conversely FDG PET can be ex- ploited for detection and assessment of infectious and
Fig. 6. Diffuse muscular FDG uptake in a 70-year-old man with diabetes mellitus. Insulin increases muscle uptake of glu- cose.
Fig. 7. Tuberculosis in a 71-year-old woman, proven by a per- cutaneous needle biopsy of the consolidation.
An axial PET/CT scan at the level of the subcarina shows dif- fuse FDG uptake in the triangular consolidation of the right upper lobe (peak SUV 3.6, thin arrows) and the peribronchial regions (peak SUV 4.0, arrow).
inflammatory lesion activities, especially in the manage- ment of the patients with fever of unknown origin (9).
Granulomatous Disorder
Active granulomatous processes such as tuberculosis, fungal infections and sarcoidosis have been reported to accumulate FDG and cause false-positive results for a malignancy on PET scans. Moreover, Goo et al. (10) re- ported that 90% of tuberculomas were falsely thought to be positive as malignant nodules when using 2.5 as the threshold SUV.
Granulomatous lesions are characterized by cellular infiltrates, granuloma formation and macrophage prolif-
eration. Activated inflammatory cells have markedly in- creased glycolysis. Uptake of FDG is more rapid in the inflammatory cells and as a rule, inflammatory tissues demonstrate avid FDG uptake, in which the uptake is predominantly in the cellular component. In tuberculo- sis, the cellular infiltrate is composed of lymphocytes and macrophages (Fig. 7) (10). FDG uptake by sarcoid granulomas is also common, which appears typically as active lymph nodes in the mediastinum and hilar re- gions (Fig. 8) (9).
Non-tuberculous Infection
FDG rapidly accumulates at sites of bacterial infection and in the reactive lymph nodes, resulting in a high con- trast between the affected and non-involved tissues. In addition to the increased glycolytic activity, the FDG ac- cumulation in activated inflammatory cells is attributed to the increased expression of the glucose. Moreover, it is possible that glucose metabolism and FDG uptake in inflammatory cells is more complicated than in malig- nant cells. For example, there is evidence that numerous cytokines and growth factors, levels of which are often increased during infection, may dramatically affect glu- cose uptake by the inflammatory cells (9).
Pyogenic infections such as abscess and pneumonia typically cause diffuse relatively uniform FDG activity.
However, with cavitation or necrosis the appearance can be indistinguishable from certain neoplasms with cavities and necrotic centers (9).
Fig. 8. Sarcoidosis in a 55-year-old woman with a history of breast cancer after surgery.
An axial PET/CT image at the level of the subcarina shows in- creased FGD uptake by multiple enlarged nodes in both hilar regions and the mediastinum (peak SUV 3.7, arrows).
Fig. 9. A bronchial stump in a 74-year-old man who under- went a left lower lobectomy due to lung cancer.
An axial PET/CT image at the carina level shows increased FDG uptake around the bronchial stump (peak SUP 5.2, ar- row). A bronchoscopic biopsy revealed only an inflammatory change.
Fig. 10. FDG uptake at the median sternotomy site in a 70- year-old man. The patient underwent bypass graft surgery for a thoracic aortic aneurysm five years ago. An axial PET/CT im- age demonstrates a localized nodular FDG uptake at the ster- notomy site (peak SUV 2.7, arrow).
Non-infectious Non-granulomatous Benign Conditions Normal wound healing is associated with an inflam- matory response and thus with modest FDG uptake (Fig. 9). Similarly, a resolving hematoma or thrombus results in modest FDG uptake since leukocytic infiltra- tion is present in the granulation tissue. Recent surgery can result in spuriously increased FDG uptake in areas of resolving inflammation. Sternotomy sites will show modest FDG uptake as well (Fig. 10) (9).
Focal FDG uptake is also seen at the insertion sites of uncomplicated indwelling percutaneous tubes or lines and permanent venous ports (Fig. 11) (5, 6).
Major arteries complicated by advanced atheromatous
disease will often be unexpectedly conspicuous due to FDG uptake by the arterial walls (Fig. 12). Atherosclerosis is an inflammatory disease, characterized by suben- dothelial lipid accumulation, monocyte/macrophage ac- crual, and vascular calcification. Macrophage aggrega- tion results in FDG uptake. As aortic aneurysm is charac- terized by transmural inflammation with lymphocyte and macrophage aggregation, FDG PET can image the aneurysmal wall (5).
Degenerative or inflammatory joint disease can give rise to elevated FDG uptake. Elevated tracer uptake in sternoclavicular joints, and to a lesser extent in the acromioclavicular joints that are frequently demonstrat- ed on bone scans, are seen far less frequently on a FDG PET scan (Fig. 13) (5).
The FDG uptake associated with radiation therapy can be seen even months after the therapy and the up-
Fig. 11. FDG uptake at the insertion site of the percutaneous tube. A 59-year-old man underwent an open lung biopsy for a mass in the right upper lobe. The mass was proven as an ade- nocarcinoma. An axial image of PET/CT demonstrates the mild FDG uptake at the entry site of the tube in the right chest wall (peak SUV 2.5, arrowhead).
Fig. 12. FDG accumulation by atherosclerosis of the aorta.
A coronal image of PET/CT shows a reversed-C-shape FDG uptake along the vascular wall of the aortic arch (peak SUV 3.2, arrow).
Fig. 13. An sternoclavicular joint in a 64-year-old man. An axi- al image of PET/CT shows mild FDG activity in the right stern- oclavicular joint (peak SUV 2.5, arrow).
Fig. 14. Radiation pneumonitis. A 30-year-old female with breast cancer, managed by radiation therapy one month ago.
An axial PET/CT scan reveals the modest band-like FDG up- take in the anterior aspect of the left upper lobe (peak SUV 6.2, arrow), corresponding to the radiation field.
take is usually slightly greater than blood pool activity.
Radiation pneumonitis, however, can be intense and difficult to differentiate from an active infection or neo- plasm (Fig. 14) (7).
Certain benign tumors and non-infectious inflamma- tory conditions have increased FDG uptake, and they can have an intensity that is entirely within the range of a malignant neoplasm (Fig. 15) (7). Yet, benign tumors of the lung with FDG uptake have rarely been reported.
Summary
FDG PET plays an important role in the evaluation of cancer. Although highly sensitive for the detection of a malignancy, FDG uptake in physiological and benign processes is also well documented. Recognition of the unusual patterns of FDG bio-distribution is important in order to avoid misinterpretation of the PET images.
PET/CT provides accurate information regarding both the morphological and metabolic aspects, enabling pre- cise localization of FDG uptake within distinct struc- tures and improving the diagnostic interpretation.
Moreover, the utility of PET/CT in the detection and characterization of infectious diseases is promising.
References
1. Wahl RL, Hawkins RA, Larson SM, Hendee WR, Coleman RE, Holden RW, et al. Proceedings of a national cancer institute work-
shop: PET in oncology?A clinical research agenda. Radiology 1994;193:604-606
2. Kostakoglu L, Agress H Jr, Goldsmith SJ. Clinical role of FDG PET in evaluation of cancer patients. Radiographics 2003;23:315-340 3. Gould MK, Maclean CC, Kuschner WG, Rydzak CE, Owens DK.
Accuracy of positron emission tomography for diagnosis of pul- monary nodules and mass lesions; a meta-analysis. JAMA 2001;285:914-924
4. Israel O, Keidar Z, Iosilevsky G, Bettman L, Sachs J, Frenkel A.
The fusion of anatomic and physiologic imaging in the manage- ment of patients with cancer. Semin Nucl Med 2001;31:191-205 5. Paul DS, Chuong DHB. Normal variants in FDG PET imaging. In
Richard LW, Julia WB. Principles and practice of positron emission tomography. Philadelphia: Lippincott Williams & Wilkins, 2002:111-136
6. Gary Jr C. Artifacts and normal variants in PET imaging. In Peter EV, Dale LB, David WT, Michael NM. Positron emission tomogra- phy, basic science and clinical practice. London: Springer, 2003:495- 505
7. Yeung HW, Grewal RK, Gonen M, Schoder H, Larson SM.
Patterns of 18F-FDG uptake in adipose tissue and muscle: a poten- tial source of false-positives for PET. J Nucl Med 2003;44:1789- 1796
8. Wittram C, Fischman AJ, Mark E, Ko J, Shepard JA. Thymic en- largement and FDG uptake in three patients: CT and FDG positron emission tomography correlated with pathology. AJR Am J Roentgenol 2003;180:519-522
9. Yoshifumi S. Infection and inflammation. In Richard LW, Julia WB.
Principles and practice of positron emission tomography. Philadelphia:
Lippincott Williams & Wilkins, 2002:381-394
10. Goo JM, Im JG, Do KH, Yeo JS, Seo JB, Kim HY, et al. Pulmonary tuberculoma evaluated by means of FDG PET: findings in 10 cas- es. Radiology 2000;216:117-121
A B
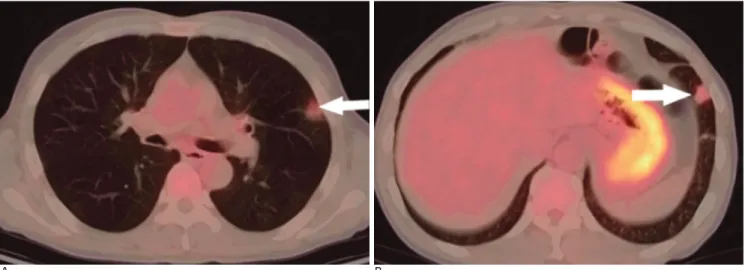
Fig. 15. Eosinophilic pneumonia in an asymptomatic 55-year-old man with peripheral eosinophilia.
(A and B) Axial PET/CT scans with a lung window setting shows two small nodular consolidations with FDG activity at the periph- ery of the left lung (peak SUV 2.5, arrows). Bronchoscopic alveolar larvage reveals many eosinophils.
대한영상의학회지 2007;57:43-50
양전자 방출 단층촬영 검사에서의 흉곽내 비악성 FDG 집적1
1강남성모병원 영상의학과
2강남성모병원 병리과
박현진・유이령・천호종・송선화・임수아・박석희・김성훈・이교영2
지금까지 악성 질환의 진단에 18FDG-양전자 방출 단층촬영 검사(PET)가 널리 쓰이고 있다. 그러나 PET에서 FDG 집적이 반드시 악성 조직에서만 이루어지는 것이 아니며 이는 지금까지의 여러 연구결과를 통해 알려졌다. 이 후 PET/CT의 개발 덕분에 FDG의 생체 내 생리학적 분포에 대해서 알려지게 되었고, 따라서 이전에 PET만으로 설명할 수 없었던 FDG 집적에 관한 재분석이 이루어졌다. 이에 저자들은 PET/CT를 통하여 흉곽 내에의 정상구 조물에 의한 정상적인 FDG 집적과 정상구조물의 생리학적 변화로 인한 FDG 집적 그리고 마지막으로 양성질환에 의한 FDG 집적의 예들을 열거하고자 한다.