접수일 : 2016 년 6 월 14 일 , 게재승인일 : 2016 년 6 월 21 일 책임저자 : 이은영 , 서울시 종로구 대학로 101
03080, 서울대학교 의과대학 내과학교실 류마티스내과
Tel: 02-2072-0852, Fax: 02-762-9662 E-mail: [email protected]
척추관절염의 진단과 치료
서울대학교 의과대학 내과학교실 류마티스내과
박은혜ㆍ이은영
Diagnosis and Management of Spondy- loarthritis
Eun Hye Park, M.D. and Eun Young Lee, M.D., Ph.D.
Division of Rheumatology, Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea Spondyloarthritis (SpA) is a group of chronic inflammatory disorders that share common clinical features, such as in- flammation of the sacroiliac joints and spinal structures, pe- ripheral arthritis, enthesitis, and extraarticular manifestations such as uveitis. They share a common genetic predis- position, the HLA-B27 gene. Radiographic sacroiliitis has been considered a hallmark of ankylosing spondylitis (AS).
However definite evidence of sacroiliitis on plain radio- graphs is not observed during the early stages of disease.
The Assessment in SpondyloArthritis international Society (ASAS) international working group has proposed a new set of diagnostic criteria that could identify SpA before the structural changes. The optimal management of patients with AS requires a combination of non-pharmacological and pharmacological treatment modalities. The first line of phar- macologic treatment is a nonsteroidal antiinflammatory drug (NSAID), and anti-TNF (tumor necrosis factor) therapy should be started to patients with high disease activity de- spite conventional treatments. TNF inhibitors have markedly improved the therapeutic options for patients with active AS.
(Clinical Pain 2016;15:1-8)
Key Words: Spondyloarthritis, Sacroiliitis, ASAS (Assessment of SpondyloArthritis international Society), NSAID, TNF inhibitors
서 론
척추관절병증은 특정 임상 증상과 유전적 관련성을 공유 하는 일련의 질환군을 의미하는 것으로, 강직척추염(anky-
losing spondylitis), 반응관절염(reactive arthritis), 건선관절 염과 척추염(psoriatic arthritis and spondylitis), 염증장질환 (inflammatory bowel disease; IBD) 관련 관절염(IBDA) 등 의 질환을 포함한다. 각각의 질병 카테고리에 정확히 부합 하는 것은 아니지만, 일반적으로 척추관절병증의 특징을 가지는 질환은 미분화척추관절염(undifferentiaed SpA)로 정의된다. 이 질환들은 유전적으로 HLA-B27과 밀접하게 연관되어 있고, 공통적으로 천장관절염(sacroiliitis) 및 척추 염(spondylitis), 주로 하지에 비대칭적으로 침범하는 소수 관절염, 부착부염(enthesitis)과 같은 근골격증상과 포도막 염(uveitis), 건선(psoriasis)과 같은 근골격외 장기 이환의 임상적 특징을 보인다.
1강직척추염과 척추관절염의 유병률은 인종과 민족에 따 라 다르며, HLA B27의 유병률에 비례하여 나타난다. 서구 에서는 강직척추염(ankylosing spondylitis)의 연간 발병률 은 100,000명당 약 0.5∼8.2명 정도이며, 유병률은 0.2∼
1.2%로 보고되고 있다. 또한 남성 대 여성의 유병률은 2:1∼
3:1 정도이며, HLA-B27 양성인 사람의 약 5∼6%에서 강 직척추염이 발생하는 것으로 알려져 있다. 척추관절염의 유병률은 강직척추염의 두 배 정도인 0.3∼2.5%로 보고되 고 있다.
2,3이에 본 종설에서는 척추관절염의 진단과 치료 에 대하여 정리해 보고자 한다.
진 단
척추관절염의 분류기준 자체는 역학 및 임상 연구에 사
용하기 위해 만들어진 것이지만 진단에도 도움을 줄 수 있
다. 강직척추염과 관련된 최초의 분류기준은 1961년에 만
들어진 분류기준이며, 이 분류기준은 이후 ‘수정 뉴욕 기
준’(Modified New York Criteria for AS)이라고 알려진
1984년의 분류기준 형태로 정착되었다(Table 1).
4수정 뉴
욕 기준에 따르면 염증성 요통, 요추 운동의 제한, 흉부 확
장능 감소의 임상기준 중 1개 이상을 만족하고, 2∼4 등급
의 양측 천장관절염 또는 등급 3∼4의 편측 천장관절염의
방사선학적 기준을 만족하는 경우, 확정 강직척추염으로
진단될 수 있다. 하지만 방사선학적 손상은 일반적으로 서
서히 진행되기 때문에, 첫 증상이 발생한 후 강직척추염으
로 확진 판정을 받기까지 10년이 지연되는 경우도 발생하
Table 1. Modified New York Criteria For AS (1984) CLINICAL CRITERIA
Low back pain and stiffness for more than 3 months that improves with exercise but are not relieved by rest Limitation of motion of the lumbar spine in both the sagittal and frontal planes
Limitation of chest expansion RADIOLOGIC CRITERIA
Sacroiliitis: grade ≥ 2 bilateral or grade 3 or 4 unilateral GRADING
Definite AS if the radiologic criterion is associated with at least one clinical variable Probable AS if
The three clinical criteria are present
The radiologic criterion is present without the clinical criteria
AS: ankylosing spondylitis (Van der Linden S et al. Arthritis Rheum 1984;27:361).
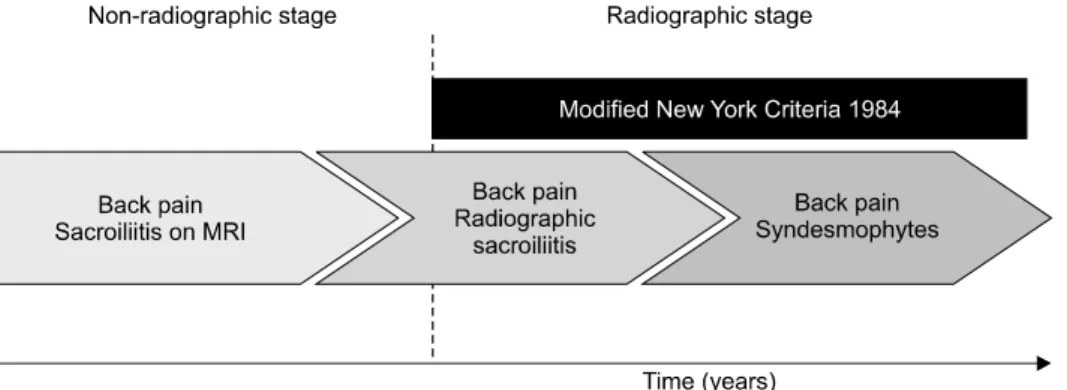
Fig. 1. The concept of axSpA. AxSpA comprises established AS at one end and an early stage of axSpA (referred to as
‘nonradiographic axSpA') at the other end. A substantial proportion of patients with nonradiographic axSpA will develop post- inflammatory structural damage of the SIJ that can be seen on plain radiographs over time. axSpA: axial spondyloarthritis (Rudwaleit, M., Khan, M. A. & Sieper, J. Arthritis Rheum. 52, 1000-1008 (2005)).
며, 분류기준을 따르게 되면 방사선학적 천장관절염을 보 이지 않는 조기 질환을 배제하게 될 수 있다(Fig. 1). 또한 요추 운동의 제한이나 흉부 확장능의 감소는 보통 질병이 상당히 경과한 이후에 관찰되고, 급성 염증을 반영하지 못 한다는 점, 축형(axial) 증상에만 집중을 하여 MRI 결과라 던가 HLA-B27 여부, 척추관절염의 가족력, NSAID에 대한 반응과 같은 임상적으로 중요한 다른 여러 척추 외의 증상 에 대해서는 고려하지 않게 된다는 점 등의 한계도 있다.
척추관절염에서 방사선학적 변화가 오기 전 조기 질환에 대한 관심이 확대되었고, 이전 기준의 한계점을 보완한 새 로운 분류기준의 필요성이 증대됨에 따라, ASAS (Assess- ment of Spondylo Arthritis international Society)에서는 대 규모의 단면 연구를 거쳐 두 개의 주요한 증상에 따라, 축형 (axial)과 말초형(peripheral) 척추관절염으로 구분한 새로 운 분류기준을 제안하였다.
5ASAS의 새로운 분류기준은 척추관절염의 여러 임상적 특징과 HLA-B27 결과, 단순X
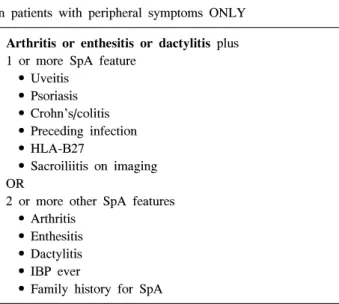
선 촬영에서 이상이 나타나기 전 급성 염증 병변을 발견할 수 있는 MRI의 소견 등을 기준에 포함하였고, 강직척추염 의 분류기준에서 제외되었던 방사선학적 천장관절염이 없 는 초기 척추관절염도 포함하였다(Table 2). 또한 척추증상 대신 말초관절염이나 부착부염, 손발가락염과 같은 말초 증상이 주증상인 환자를 대상으로 말초형 척추관절염의 분 류기준도 제시되었다(Table 3).
5,6임상양상
1. 염증성 요통
염증성 요통은 강직척추염을 의심하게 하는 가장 중요한
소견으로, 환자가 ASAS에서 제시한 다음 5가지 항목((1)
발생연령 40세 미만 (2) 서서히 발생 (3) 운동으로 호전 (4)
휴식으로 호전되지 않음 (5) 야간 통증 및 기상 시 호전)
중 4개 이상의 항목에 해당되면 염증성 요통으로 간주될
Table 2. ASAS classification criteria for axial SpA
In patients with 3 months or more, of back pain and age of onset < 45 Sacroiliitis on imaging
aplus 1 or more SpA feature OR
HLA-B27 plus 2 or more other SpA features SpA features:
• Inflammatory back pain (IBP) • Arthritis
• Enthesitis (heel) • Uveitis
• Dactylitis • Psoriasis • Crohn’s/colitis
• Good response to NSAIDs • Family history of SpA • HLA-B27
• Elevated CRP
a