Background: In this study we assessed the mid-term results of arthroscopic augmentation with porcine dermal xeno- grafts for irreparable rotator cuff tears.
Methods: Between February 2010 and February 2012, ten patients with irreparable rotator cuff tears were treated with arthroscopic augmentation with porcine dermal xenografts. All patients were followed up for at least three years. Clinical scores the University of California, Los Angeles (UCLA) scoring system, the Constant score, and the American Shoulder and Elbow Surgeons (ASES) shoulder score were evaluated both preoperatively and postoperatively in all patients. We evaluated repair status in terms of radiological outcome through magnetic resonance imaging after a mean 10.3 months of operation.
Results: The study population consisted of seven men and three women with a mean age of 64.9 years (range, 53–72 years) and a mean follow-up of 42.5 months (range, 36.2–47.1 months). The clinical outcome significantly improved for all patients. The mean UCLA score increased from 15.50 preoperatively to 30.10 postoperatively (P < 0.001). The mean Constant score improved from 59.80 to 83.90 (P = 0.001), and the mean ASES score, from 58.60 to 85.30 (P = 0.001). How- ever, there were no significant differences between the intact group and the retear group in terms of clinical results. Mag- netic resonance imaging at the follow-up examinations demonstrated patch continuity between the native cuff and the greater tubercle in five patients (50%). We did not observe any significant difference between the intact group and retear group in terms of, preoperatively, the size of the tear, degree of muscle atrophy, smoking status, use of steroids, and, post- operatively, the rehabilitation protocol.
Conclusion: We found that arthroscopic repairs using porcine dermal xenografts for irreparable massive rotator cuff tears is associated with improved clinical outcome in most patients, despite a retear rate of 50%. Thus, we conclude that por- cine dermal patch augmentation can be one of the treatment options for patients with either reparable subscapularis or infraspinatus.
Keywords: Arthroscopic repair; Irreparable massive rotator cuff tear; Porcine dermal xenograft
Mid-term results of arthroscopic porcine dermal xenograft augmentation for irreparable massive rotator cuff tears: a 3-year follow-up study
Sang Jin Cheon, Ji Min Lee, Sung Jin An, Hyo Yeol Lee
Department of Orthopedic Surgery, School of Medicine, Pusan National University, Busan, Korea
Copyright © 2017 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received November 8, 2016; Revised April 24, 2017; Accepted April 25, 2017
Correspondence to: Sang Jin Cheon, Department of Orthopedic Surgery, Pusan National University Hospital, School of Medicine, Pusan National University, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea. Tel: +82-51-240-7248, Fax: +82-51-247-8395, E-mail: [email protected] Arthroscopy and
Orthopedic Sports Medicine
AOSM
INTRODUCTION
The clinical outcomes of open or arthroscopic repairs of rotator cuff tears have been commonly reported to be favorable. Yet the anatomical repair of large-to-massive rotator cuff tears, of cuff tears combined with severe fatty infiltration or muscle atrophy, or of those with severe adhesions to the surrounding tissues has been shown to be difficult, and the occurrence of re-tears have been re-
ported to be high among even those successfully treated [1–4]. Alternative surgical treatments for irreparable mas- sive rotator cuff tears include debridement and subacro- mial decompression [3,5,6], arthroscopic partial repair [2], tendon transfer [7–9], arthroplasty [10,11], and allograft- ing or xenografting [12–17]. For allografts and xenografts, example graft source are autografts or allografts of the fascia lata, freeze-dried rotator cuff allografts [15], and composites such as the Gore tex [17] and poly-L-latic acid
[18], autogenous biceps tendons [19]. Each treatment shows varying clinical outcomes, and neither the relative benefits of treatments nor indications/contraindications for each treatment have not been established. Current literature describes a mixture of outcomes for the treat- ment of massive rotator cuff tears. For instance, in their study of 16 patients with massive rotator cuff tears, Nevi- aser et al. [15] reported that freeze-dried graft augmen- tation was associated with either decreased or resolved pain and with good or excellent clinical outcomes in all patients save two. In another study, Ito and Morioka [20]
found that patch augmentation was associated with less re-tears than the McLaughlin technique for cuff repairs, while Moore et al. [19] suggested that allograft transplan- tations are not effective for massive rotator cuff tears.
Recently, several animal studies have reported that augmentation using grafts derived from human, bovine, or porcine small intestine or the dermis improves the repair prospects of irreparable massive rotator cuff tears [21]. The importance of grafts as scaffolds for mechanical support at the repair site and as stimulants of cell prolif- eration and differentiation for expedited tendon-to-bone healing have also been highlighted [18]. Here, we report the clinical outcomes of using all-arthroscopic repair using PermacolTM (Tissue Science Laboratories plc, Al- dershot, UK), a porcine freeze-dried dermal xenograft, to treat anatomically irreparable massive rotator cuff tears.
METHODS
This study was approved by the Institutional Review Board of Pusan National University Hospital (IRB No.
D-1208-001-001).
We enrolled a total of ten patients with irreparable massive rotator cuff tears combined with severe muscle atrophy between February 2010 and February 2012 at Pusan National University Hospital (Fig. 1). The follow- ing inclusion criteria were used (1) massive rotator cuff tears deemed irreparable through magnetic resonance imaging (MRI) or arthroscopy; (2) tears that do not reach the greater tuberosity (and thus does not lend itself to anatomical repair); (3) patients aged 60 years or younger who are active and has a will to be treated; and (4) non- responsiveness to 6 to 8 months of conservative treat- ment. Conversely, patients with massive rotator cuff tears that could be anatomically repaired with tension; pa- tients noncompliant to postoperative rehabilitation; and patients who presented with infection or inflammation were excluded from the study.
Among the ten patients, three had had a total of 1 to 3 primary/revision repairs of the rotator cuff tears at an external hospital. In this study, the first two patients were treated using a 1.0-mm-thick PermacolTM but the subsequent eight patients were treated using a 1.5-mm- thick PermacolTM, because the 1.0-mm-thick graft was considered to be too thin (Fig. 2). In eight patients, we
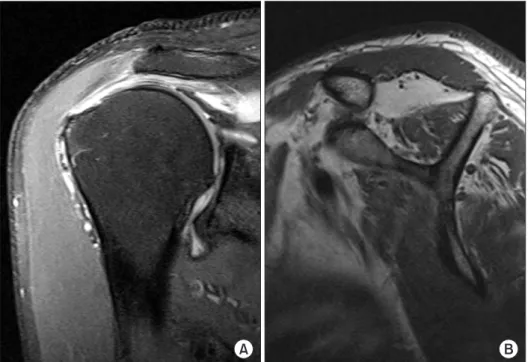
Fig. 1. A 56-year-old man with large rotator cuff tear of right shoulder and substantial fatty muscle degeneration.
(A) Preoperative magnetic resonance imaging shows massive rotator cuff tear and medial retraction with thinning of tendons. (B) Preoperative sagittal oblique image shows fatty degenerated and atro- phied muscles.
A B
used a margin convergence technique to avoid apply- ing tension to the area of deficit, and thus to prevent its enlargement, and performed bridging graft repair using PermacolTM. The bridging graft repair involved either us- ing a simple suture to implant the PermacolTM to the torn medial tendon or a suture and suture anchor to implant the PermacolTM to the lateral tendon and unto the greater tuberosity. In the remaining two patients, only the bridg- ing graft repair with PermacolTM was performed. We ob- served concomitant subscapularis tendon tears in nine of ten patients. Amongst them, we performed a combined debridement and subscapularis tendon repair in five pa- tients and debridement alone in the rest, because the se- verity of the subscapularis tear of the latter set of patients prevented us from making an anatomical repair (Table 1).
Each patient was followed up for at least three years.
The following parameters of clinical outcome were mea-
sured both at the preoperative examination and at the final follow-up: the University of California, Los Angeles (UCLA) score; the Constant score; and the American Shoulder and Elbow Surgeons (ASES) score. The patients were also assessed radiologically through MRI after an average 10.3 months postoperatively.
To compare the risk factors between patients with and those without ruptures of the graft, we analyzed the fol- lowing factors: size of cuff tear; extent of muscle atrophy and fatty infiltration; smoking status; preoperative adre- nocortical hormone use; preoperative superior displace- ment of the humeral head, that is, the acromiohumeral distance; and the commencement period of postopera- tive rehabilitation (early vs. late). The preoperative fatty infiltration of the rotator cuff muscles was measured us- ing the Goutallier’s global fatty degeneration index [22], and the progression of muscle atrophy was assessed Table 1. Detailed demographic data of patients
Case no.
Sex/
age (yr)
Permacol™
thickness (mm)
Previous surgery history
Margin convergence technique
Subscapularis tendon repair
Tear size (mm)
Fatty infiltration Width (AP) Height (ML)
1 F/61 1.0 – – – 4.9 5.2 Grade 2
2 M/70 1.0 – + – 5.1 5.4 Grade 3
3 M/59 1.5 – + + 5.2 5.7 Grade 3
4 F/71 1.5 + + – 5.4 5.6 Grade 4
5 M/53 1.5 + + + 4.6 5.4 Grade 2
6 M/56 1.5 + + + 5.1 5.6 Grade 2
7 M/56 1.5 – – – 4.7 5.7 Grade 3
8 F/72 1.5 – + + 5.1 5.5 Grade 4
9 M/69 1.5 – + – 5.0 5.3 Grade 4
10 F/68 1.5 – + + 4.9 5.6 Grade 4
Stage 0, corresponds to a completely normal muscle, without any fatty streak; Stage 1, the muscle contains some fatty streaks; Stage 2, the fatty infiltra- tion is important, but there is still more muscle than fat; Stage 3, there is as much fat as muscle; Stage 4, more fat than muscle is present.
F, female; M, male; AP, anterior-posterior; ML, medial-lateral.
Fig. 2. Arthroscopic repair by use of a porcine dermal xenograft (PermacolTM; Tissue Science Laboratories plc, UK). (A) The arthroscopic photograph shows right massive rotator cuff tear. (B) The torn rotator cuff tendon is repaired partially using suture anchor. (C) Arthroscopic placement of a porcine dermal xenograft to bridge the defect between native cuff and greater tubercle was performed.
A B C
using oblique sagittal MRI as determined through a posi- tive tangent sign [23]. The superior displacement of the humeral head was evaluated pre- and postoperatively using the shoulder and the supraspinatus outlet MRI ra- diographs [24].
In all patients, a common postoperative rehabilitation protocol, which involved applying a shoulder abduction brace for six weeks, was conducted. The first five patients to receive rehabilitation were permitted to begin pendu- lum exercises from the day after the operation and pas- sive range of motion (ROM) exercises within two weeks of the operation. However, the subsequent five patients were not permitted to begin pendulum exercises until the 4th postoperative week, and passive ROM exercises were begun with caution from the 5th postoperative week in these patients. In all patients, active assisted ROM exer- cises were begun after a week of passive ROM exercises, and muscle strengthening exercises, from the 12th post- operative week.
To analyze the statistical significance of the differences between the preoperative and postoperative values, we
conducted statistical tests, such as the paired t-test, on SPSS (for Windows 12.0; SPSS Inc., Chicago, IL, USA). Sta- tistical significance was set as a P-value of less than 0.05 and a confidence interval of 95%.
RESULTS
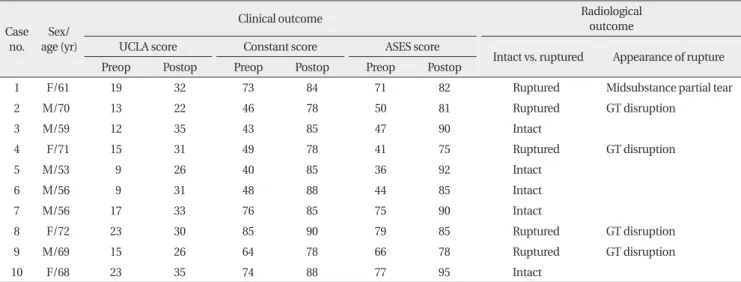
The study population consisted of seven male patients and three female patients. The average age of the patients at the time of operation was 64.9 years (range, 53–72 years), and the average follow-up period was 42.5 months (range, 36.2–47.1 months). We found that the average UCLA score significantly improved from a preoperative score of 15.5 (‘average’ in 2 patients; ‘poor’ in 8 patients) to a postoperative score of 30.10 (‘fair’ in 9 patients; ‘av- erage’ in 1 patient) (P < 0.001). Likewise, the respective improvements in the average Constant and ASES scores were both statistically significant (Tables 2, 3).
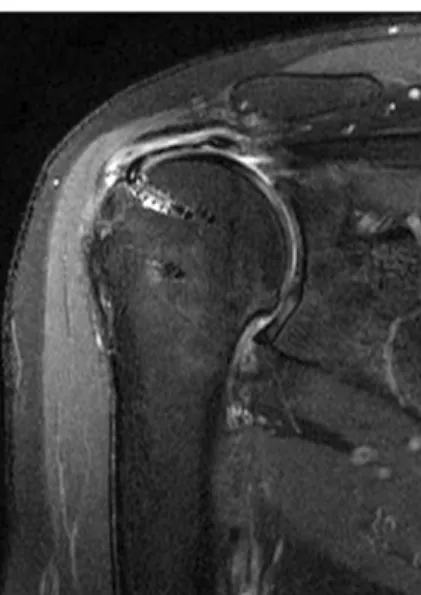
During an MRI follow-up at an average 10.3 months of operation, we found that there were five patients with ruptured grafts and five patients with intact grafts (Fig.
3). Follow-up MRI revealed that the two patients who were treated using the 1.0-mm-thick PermacolTM had torn grafts whereas only three in eight patients who were treated using the 1.5-mm-thick PermacolTM had torn grafts, while five didn’t (Table 1). Among the patients with ruptured grafts, one patient was shown to have a history of three operations for a rotator cuff tear. The patient, in spite of improved clinical parameters, later received a revision treatment of debridement due to unsatisfac- Table 2. Clinical and radiological outcomes
Case no.
Sex/
age (yr)
Clinical outcome Radiological
outcome
UCLA score Constant score ASES score
Intact vs. ruptured Appearance of rupture
Preop Postop Preop Postop Preop Postop
1 F/61 19 32 73 84 71 82 Ruptured Midsubstance partial tear
2 M/70 13 22 46 78 50 81 Ruptured GT disruption
3 M/59 12 35 43 85 47 90 Intact
4 F/71 15 31 49 78 41 75 Ruptured GT disruption
5 M/53 9 26 40 85 36 92 Intact
6 M/56 9 31 48 88 44 85 Intact
7 M/56 17 33 76 85 75 90 Intact
8 F/72 23 30 85 90 79 85 Ruptured GT disruption
9 M/69 15 26 64 78 66 78 Ruptured GT disruption
10 F/68 23 35 74 88 77 95 Intact
UCLA score, University of California, Los Angeles score; ASES score, American Shoulder and Elbow Surgeons shoulder score; Preop, preoperative; Po- stop, postoperative; F, female; M, male; GT, greater tubercle.
Table 3. Clinical assessment
Preoperative Postoperative P-value UCLA score 15.50 ± 5.06 30.10 ± 4.23 < 0.001 Constant score 59.80 ± 16.37 83.90 ± 4.46 0.001 ASES score 58.60 ± 16.58 85.30 ± 6.43 0.001 Values are presented as mean ± standard deviation.
UCLA score, University of California, Los Angeles score; ASES score, American Shoulder and Elbow Surgeons shoulder score.
tory treatment outcomes. We kept a vigilant eye on the treatment progress of the other four patients because the clinical outcomes of their treatment had been favorable.
There were no postoperative complications, such as infection or graft-versus-host disease, in any of the pa- tients until the final follow-up. We compared the follow- ing risk factors between our two groups of patients: size of cuff tears; extent of muscle atrophy and fatty infiltra- tion; smoking status; preoperative use of adrenocortical steroids; preoperative acromiohumeral distance; and commencement period of postoperative rehabilitation.
Rotator cuff tears with deficits that required arthroscopic patch grafts were assessed and the area of deficit was measured arthroscopically and intraoperatively. The area of the deficit that required patch augmentation did not statistically differ between the two groups (Table 4).
We found that compared to the intact group the rup- tured group had more severe fatty infiltration in terms of the Goutallier fatty index, while the intact group had more severe muscle atrophy, determined using the posi- tive tangent sign, than the ruptured group. However, these differences were not tested statistically on account of a small study population. In terms of smoking status and preoperative adrenocortical hormone use, we found that the ruptured group had a greater proportion of non- Fig. 3. At postoperative 10 months, the oblique coronal magnetic reso-
nance imaging shows that the intact patch continuity between native cuff and greater tubercle.
Table 4. Risk factor analysis
Parameter Intact group (n = 5) Ruptured group (n = 5) P-value
Size of tear (mm)
Width (AP) 4.90 ± 0.25 5.10 ± 0.19 NS
Height (ML) 5.60 ± 0.12 5.40 ± 0.16 NS
Reduction of acromiohumeral distance (mm)
X-ray (AP) 8.21 ± 0.12 6.55 ± 0.10 < 0.001
X-ray (outlet view) 6.17 ± 0.07 5.54 ± 0.13 < 0.001
MR (coronal) 5.18 ± 0.05 4.54 ± 0.13 < 0.001
MR (sagittal) 5.70 ± 0.09 4.14 ± 0.12 < 0.001
Goutallier fatty index
2 2 1
3 2 1
4 1 3
Smoking history
+ 2 1
– 3 4
Steroid injection history
+ 2 4
– 3 1
Postoperative rehabilitation protocol
Early 2 4
Late 3 1
Values are presented as mean ± standard deviation or number only.
AP, anterior-posterior; ML, medial-lateral; MR, magnetic resonance; NS, not significant.
smokes and users of steroid hormones than the intact group, but again the statistical significance of these dif- ferences was not evaluated.
We found that patients with ruptured grafts had a sig- nificantly more severe superior displacement of the hu- meral head preoperatively than patients with intact grafts (Table 4). The commencement period of postoperative rehabilitation, in particular when ROM exercises were be- gun, was within two and four weeks of the operation for four and one cases, respectively, in the ruptured group, and within two and four weeks for two and three cases, respectively, in the intact group. Though not with statis- tical significance, these data suggest that in general the ruptured group received rehabilitation more quickly than the intact group.
DISCUSSION
In this study, we found that the clinical outcomes im- proved in all patients who were treated by arthroscopic PermacolTM implant augmentation. Favorable clinical outcomes were observed in patients under 60 years of age; in patients treated using a 1.5-mm-thick, as opposed to a 1.0-mm-thick, PermacolTM; and in patients whose subscapularis tendon or infraspinatus tendon could be at least partially repaired.
It is still difficult to treat irreparable massive rotator cuff tears despite technological advancements in arthroscopic procedures generally because of severe muscle atrophy and fatty infiltration. Various surgical treatment options have been described in the literature, yet it is unclear whether there exists a gold standard of treatment or whether indications or contraindications exist that sug- gests the choice of one treatment over another. Recently, there has been substantial research investigating the ef- fectiveness of novel approaches to treat these irreparable rotator cuff tears, with the aim to restore the anatomical continuity, such as augmentation, allografting, or xeno- grafting [12–17].
Ideally, grafts for cuff augmentation should originate from the body and be biologically inactive; an ideal graft would therefore have optimal tensile strength and stimu- late invasion and revascularization of the fibroblasts before the tensile strength of the graft is lost, enhancing healing. Animal studies using PermacolTM have shown mixed outcomes. For instance, tissue ingrowth was observed without complications such as host-versus- graft reaction or immune responses after subscapularis
tendon repairs using porcine dermal xenografts in adult dogs [25]. In rabbits, conversely, a graft consisting of five constituents including PermacolTM was reported to be associated with prominent host reaction and decomposi- tion responses [26].
In a randomized control study, Iannotti et al. [12] re- ported that patients treated with porcine small intestine submucosa xenografts were associated with poorer clini- cal outcomes than those treated without the porcine graft. They found that xenografts derived from the dermis was not only stronger than porcine small intestine sub- mucosa xenografts but also associated with less reduc- tion failure caused by suture loosening, as well as less allergic response, toxicity, and graft reaction [14].
PermacolTM is a porcine dermal collagen implant lack- ing of non-collagenous materials, such as cells, DNA, and RNA. This acellular implant has very similar properties to human tissue, and its scaffold contains elastin fibers that have been sterilized using gamma radiation [27]. Cross- linked with hexamethylene disocyanate, the implant is resistant towards collagenase breakdown that cause absorption and degradation of collagen and, therefore, promotes soft tissue engineering and regeneration [28].
Using PermacolTM, Soler et al. [29] reported initial opti- mistic outcomes for arthroscopic augmentation in four patients with massive rotator cuff tears but found that all patients exhibited ruptured grafts by the 6-month follow- up. Thus, the authors of the study suggested, in spite of its many advantages, against PermacolTM for irreparable massive rotation cuff tears. Conversely, Badhe et al. [14]
reported using ultrasound and MRI that PermacolTM for massive rotator cuff tears was associated with favorable clinical outcomes at one-year follow-up and that eight in ten patients (with an average age of 66 years) had intact grafts by the final follow-up. Furthermore, none of these patients had showed any postoperative complications.
Thus, they concluded that in most patients with massive rotator cuff tears PermacolTM for arthroscopic cuff aug- mentation is safe and effective.
In this study, patients with irreparable massive cuff tears were treated using an all-arthroscopic rotator cuff repair with a bridging graft technique and PermacolTM implant. We found that the clinical indices significantly improved in all patients after treatment. However, we observed at the follow-up MRI that one patient, who had the poorest radiological outcomes among the study population, had a ruptured graft. And despite improved clinical parameters the patient was unsatisfied with the
treatment outcomes and, therefore, received revision treatment. In the other four patients found radiologically to have ruptured graft were monitored for progress since these patients were satisfied with treatment outcomes and had significantly improved clinical parameters.
We found that the intact group had less fatty infiltration than the ruptured group, although we observed some degree of muscle atrophy in the intact group. Among the five patients who underwent a combined subscapularis tendon repair, only a single patient presented with a ruptured graft, while ruptures were observed in all four patients who had irreparable tears. In addition, in this study all patients treated using a 1.0-mm-thick Perma- colTM implant had ruptures, compared to only three out of eight patients treated using 1.5-mm-thick PermacolTM. Together, these findings suggest that subscapularis ten- don repair and PermacolTM thickness may be important determinants of arthroscopic augmentation. Reporting the biomechanical properties and the appearances of ruptures within different types of grafts, Barber et al. [30]
observed that the PermacolTM implants failed by the su- ture techniques—the isthmus pull-through and the side pull-through—but not by the end pull-through. Similarly, we found that four in five cases had a rupture in the foot- print between the PermacolTM and the greater tuberosity of the humerus [30].
In this study, we found that certain graft rupture-de- pendent differences were seen among the various factors assessed in this study. However, the small study popula- tion restricted us from testing the statistical significance of the observed differences. Therefore, future studies with a greater number of study participants are needed.
Major limitations of this study are that the study had a small study population and that there were no controls, meaning that the relative contribution of PermacolTM towards the beneficial clinical outcomes cannot be de- termined empirically or its association established. And
because radiological examinations were performed on average after 10 postoperative months, while clinical ex- aminations were performed on average 42 months post- operatively, we did not evaluate the possibility of ruptures occurring after 10 months. Further, our study population was not homogeneous in terms of the implant used and the rehabilitation protocol: a subset of patients were treated with a 1.0-mm-thick PermacolTM while another subset, with a 1.5-mm-thick PermacolTM and some pa- tients began rehabilitation exercises two weeks earlier than others. Lastly, although the clinical outcomes of the 3-year follow-up suggest an improvement associated with the use of the porcine xenografts, a longer follow-up may reveal more or altered clinical effects. Further ran- domized control studies investigating the effectiveness and the long-term outcomes of PermacolTM are required.
Here, we found that all-arthroscopic rotator cuff re- pairs using porcine freeze-dried dermal xenografts may provide enhanced clinical outcomes for massive rota- tor cuff tears that are untreatable through arthroscopic repairs. Yet despite the favorable clinical outcomes of arthroscopic porcine dermal augmentation, we observed that postoperative MRI findings were associated with a high incidence of ruptures of the graft implant. For these reasons we suggest that the use of arthroscopic porcine dermal augmentation for massive rotator cuff tears is restricted to patients in whom either the subscapularis tendon or the infraspinatus tendons can be partially re- paired. More studies with greater statistical power should be performed investigating the effectiveness of and the indications for arthroscopic porcine dermal augmenta- tion in patients with irreparable rotator cuff tears.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Boes MT, McCann PD, Dines DM. Diagnosis and management of massive rotator cuff tears: the surgeon’s dilemma. Instr Course Lect 2006;55:45-57.
2. Duralde XA, Bair B. Massive rotator cuff tears: the result of par- tial rotator cuff repair. J Shoulder Elbow Surg 2005;14:121-7.
3. Gartsman GM. Massive, irreparable tears of the rotator cuff. Re- sults of operative debridement and subacromial decompression.
J Bone Joint Surg Am 1997;79:715-21.
4. Gerber C, Fuchs B, Hodler J. The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am 2000;82:505-15.
5. Klinger HM, Steckel H, Ernstberger T, Baums MH. Arthroscopic debridement of massive rotator cuff tears: negative prognostic factors. Arch Orthop Trauma Surg 2005;125:261-6.
6. Liem D, Lengers N, Dedy N, Poetzl W, Steinbeck J, Marquardt B. Arthroscopic debridement of massive irreparable rotator cuff tears. Arthroscopy 2008;24:743-8.
7. Elhassan B, Endres NK, Higgins LD, Warner JJ. Massive irrepara- ble tendon tears of the rotator cuff: salvage options. Instr Course Lect 2008;57:153-66.
8. Gerber C, Maquieira G, Espinosa N. Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears. J Bone Joint Surg Am 2006;88:113-20.
9. Pearsall AW 4th, Madanagopal SG, Karas SG. Transfer of the latissimus dorsi as a salvage procedure for failed debridement and attempted repair of massive rotator cuff tears. Orthopedics 2007;30:943-9.
10. Glanzmann MC, Flury M, Simmen BR. Reverse shoulder arthro- plasty as salvage procedure after deltoid muscle flap transfer for irreparable rotator cuff tear: a case report. J Shoulder Elbow Surg 2009;18:e1-2.
11. John M, Pap G, Angst F, et al. Short-term results after reversed shoulder arthroplasty (Delta III) in patients with rheumatoid ar- thritis and irreparable rotator cuff tear. Int Orthop 2010;34:71-7.
12. Iannotti JP, Codsi MJ, Kwon YW, Derwin K, Ciccone J, Brems JJ.
Porcine small intestine submucosa augmentation of surgical repair of chronic two-tendon rotator cuff tears. A randomized, controlled trial. J Bone Joint Surg Am 2006;88:1238-44.
13. Sano H, Mineta M, Kita A, Itoi E. Tendon patch grafting using the long head of the biceps for irreparable massive rotator cuff tears.
J Orthop Sci 2010;15:310-6.
14. Badhe SP, Lawrence TM, Smith FD, Lunn PG. An assessment of porcine dermal xenograft as an augmentation graft in the treatment of extensive rotator cuff tears. J Shoulder Elbow Surg 2008;17(1 Suppl):35S-9S.
15. Neviaser JS, Neviaser RJ, Neviaser TJ. The repair of chronic massive ruptures of the rotator cuff of the shoulder by use of a freeze-dried rotator cuff. J Bone Joint Surg Am 1978;60:681-4.
16. Audenaert E, Van Nuffel J, Schepens A, Verhelst M, Verdonk R.
Reconstruction of massive rotator cuff lesions with a synthetic interposition graft: a prospective study of 41 patients. Knee Surg Sports Traumatol Arthrosc 2006;14:360-4.
17. Hirooka A, Yoneda M, Wakaitani S, et al. Augmentation with a Gore-Tex patch for repair of large rotator cuff tears that cannot be sutured. J Orthop Sci 2002;7:451-6.
18. Lenart BA, Martens KA, Kearns KA, Gillespie RJ, Zoga AC, Wil- liams GR. Treatment of massive and recurrent rotator cuff tears augmented with a poly-l-lactide graft, a preliminary study. J Shoulder Elbow Surg 2015;24:915-21.
19. Moore DR, Cain EL, Schwartz ML, Clancy WG Jr. Allograft recon- struction for massive, irreparable rotator cuff tears. Am J Sports Med 2006;34:392-6.
20. Ito J, Morioka T. Surgical treatment for large and massive tears of the rotator cuff. Int Orthop 2003;27:228-31.
21. Aurora A, McCarron J, Iannotti JP, Derwin K. Commercially avail- able extracellular matrix materials for rotator cuff repairs: state of the art and future trends. J Shoulder Elbow Surg 2007;16(5 Suppl):S171-8.
22. Goutallier D, Postel JM, Bernageau J, Lavau L, Voisin MC. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res 1994;(304):78-83.
23. Mellado JM, Calmet J, Olona M, et al. Surgically repaired massive rotator cuff tears: MRI of tendon integrity, muscle fatty degenera- tion, and muscle atrophy correlated with intraoperative and clini- cal findings. AJR Am J Roentgenol 2005;184:1456-63.
24. Saupe N, Pfirrmann CW, Schmid MR, Jost B, Werner CM, Zanetti M. Association between rotator cuff abnormalities and reduced acromiohumeral distance. AJR Am J Roentgenol 2006;187:376- 82.
25. Dejardin LM, Arnoczky SP, Ewers BJ, Haut RC, Clarke RB. Tissue- engineered rotator cuff tendon using porcine small intestine submucosa. Histologic and mechanical evaluation in dogs. Am J Sports Med 2001;29:175-84.
26. Derwin KA, Baker AR, Spragg RK, Leigh DR, Iannotti JP. Commer- cial extracellular matrix scaffolds for rotator cuff tendon repair.
Biomechanical, biochemical, and cellular properties. J Bone Joint Surg Am 2006;88:2665-72.
27. Harper C. Permacol: clinical experience with a new biomaterial.
Hosp Med 2001;62:90-5.
28. Jarman-Smith ML, Bodamyali T, Stevens C, Howell JA, Horrocks M, Chaudhuri JB. Porcine collagen crosslinking, degradation and its capability for fibroblast adhesion and proliferation. J Mater Sci Mater Med 2004;15:925-32.
29. Soler JA, Gidwani S, Curtis MJ. Early complications from the use of porcine dermal collagen implants (Permacol) as bridging con- structs in the repair of massive rotator cuff tears. A report of 4 cases. Acta Orthop Belg 2007;73:432-6.
30. Barber FA, Herbert MA, Coons DA. Tendon augmentation grafts:
biomechanical failure loads and failure patterns. Arthroscopy 2006;22:534-8.