INTRODUCTION
Many patients who undergo rotator cuff repairs have preoperative shoulder stiffness. However, the exact incidence and magnitude of shoulder stiffness in rotator cuff patients have never been deeply studied [1,2].
Although the exact etiology is not known, several different factors have been suggested to explain the occurrence of rotator cuff tears with stiffness; presence of trauma, diabetes, bursal inflammation, capsulitis, fatty infiltration, and atrophy of the muscles, are known factors relating to injured rotator cuff tendons [3]. Preoperative shoulder
stiffness can affect the surgical outcomes of a rotator cuff repair, and it can also lead to discomfort during daily activities. Patients with rotator cuff tears and combined shoulder stiffness often have difficulty performing passive and active exercises after postoperative immobilization due to severe pain and advanced stiffness. In these patients, the conventional treatment for shoulder stiffness is conservative management before the rotator cuff repair, but some have proposed a concomitant manipulation and rotator cuff repair of rotator cuff tears with shoulder stiffness [4,5].
Whether the rotator cuff tears or the shoulder stiffness Background: Some patients with rotator cuff tears have preoperative shoulder stiffness, and this may affect the functional outcomes after repair of the rotator cuffs. The purpose of this study was to evaluate the outcomes of closed manipulation and arthroscopic repair of rotator cuff tears in patients with combined preoperative shoulder stiffness.
Methods: Of the 200 patients who underwent arthroscopic rotator cuff repair from January 2008 to December 2012, 18 patients had preoperative shoulder stiffness at the time of repair. The incidence of preoperative shoulder stiffness was 9.0%
(18 of 200 patients). All patients underwent closed manipulation and arthroscopic rotator cuff repair concomitantly, and had a sling with an abduction pillow for 6 weeks except when changing clothes. All patients were evaluated preoperatively and at a minimum of 1year followup using the visual analog scale (VAS) for pain, Constant score, and ultrasonograpy.
Results: The mean preoperative VAS and Constant scores were 7.6 and 50.6, respectively. The mean VAS score at the last followup was 2.8, and the mean Constant score was 82.4. The functional outcomes improved compared with the preoperative state (P < 0.001). Results were in 9 cases “excellent”, in 5 cases “good”, in 2 cases “fair”, and in 2 cases “poor”.
Of the 5 patients who showed severe shoulder stiffness preoperatively, 2 later showed poor functional outcomes. Repair integrities noted postoperatively were 12 intact cuffs, 5 partialthickness tears, and 1 fullthickness tear, as determined by the Naqvi classification.
Conclusion: We suggest that concomitant closed manipulation and arthroscopic rotator cuff repair could be a simple and an effective surgical treatment for rotator cuff tears combined with shoulder stiffness.
Keywords: Rotator cuff tear; Rotator cuff repair; Stiff shoulder; Joint capsule release
Outcomes of closed manipulation and arthroscopic repair for rotator cuff tears combined with shoulder stiffness
Sung-Weon Jung, Byung-Woo An, Sang-Soo Kang, Seung-Bo Shim, Min Jeong
Department of Orthopaedic Surgery, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea
Copyright © 2014 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received December 23, 2013; Revised May 15, 2014; Accepted May 16, 2014
Correspondence to: Sung-Weon Jung, Department of Orthopaedic Surgery, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, 158 Paryong-ro, Masanhoewon-gu, Changwon 630-723, Korea. Tel: +82-55-290-6030, Fax: +82-55-290- 6888, E-mail: [email protected]
Arthroscopy and Orthopedic Sports Medicine
AOSM
should be prioritized in the treatment has been continually debated. It is generally thought that these two operations cannot be performed in conjunction as protection and immobilization of the affected shoulder are critical after a rotator cuff repair, whereas passive or active stretching exercises are critical for shoulder stiffness. If a rotator cuff is repaired without prior treatment of the stiff shoulder, the healing process of the cuff repair and postoperative adhesion often cause progression of shoulder stiffness.
On the other hand, if a stiff shoulder is managed before the rotator cuff repair, additional injury to the rotator cuff can occur as a result of forceful manipulation of a shoulder with an impingement syndrome. Furthermore, there is no universal agreement on the acceptable level of stiffness at the time of cuff repair, and immediate postoperative stretching exercises for stiff shoulders may worsen the condition of the repaired cuff tear [6]. Some studies have reported that the relationship between arthroscopic capsular release, rehabilitation after rotator cuff repair and the development of postoperative stiffness is uncertain [7,8]. This study investigated the outcomes of closed manipulation and arthroscopic rotator cuff repair of patients with rotator cuff tears combined with shoulder stiffness.
METHODS
Patient selection
Of the 200 patients who underwent arthroscopic rotator cuff repair from January 2008 to December 2012 at our institute, 18 patients with preoperative shoulder stiffness were included in our study. All surgeries were performed by a single surgeon (S.W.J.). With respect to defining a stiff shoulder, there is still an unresolved controversy as to whether the position of the arm is on the side or with 90o abduction when measuring external rotation (ER) to determine stiffness. As done by Brislin et al. [9], we defined shoulder stiffness as total active and passive forward flexion (FF) of < 100o, and total passive ER of < 30o with the arm in 90o of abduction, because we thought these limits were more clinically acceptable considering the patients’ daily lives. In addition, the diagnosis of shoulder stiffness was made only when these motion deficits persisted for 90 days. Patients with massive (> 5 cm) rotator cuff tears, advanced glenohumeral arthritis, revision surgery, conversion to open repair, or an acromioclavicular arthritis that required distal clavicle resection were excluded from this study. However, there is
no universal agreement on the acceptable level of stiffness at the time of cuff repair, and an unacceptable level at which point an immediate postoperative stretching exercise would worsen the condition of the repaired cuff tear. Capsular release was not performed in any case. This study included 7 men and 11 women with a mean age of 58.7 years (range, 48-72 years). The mean duration of symptoms before surgery was 5.5 months (range, 3-24 months). All patients were followedup for at least 20.2 months (range, 24-60 months). The rotator cuff tears were categorized according to the DeOrio and Cofield [10] classification system and shoulder stiffness were categorized as mild (FF 80o-99o, ER 20o-29o), moderate (FF 60o-79o, ER 10o-19o), or severe (FF < 60o, ER <10o). This study was approved by the Institutional Review Board Committee of Samsung Medical Center.
Preoperative and postoperative evaluations
Examinations were performed 1 day before the operation and at least 1 year after the operation. Pre and post
operative subjective pain was measured with a visual analog scale (VAS), with 0 indicating “no pain” and 10 indicating “extremely severe pain.” The Constant score was used for clinical assessment [11]. Active and passive range of motion (ROM) of shoulder, including FF, abduction, internal rotation, and ER, at the side and in 90o of abduction were measured with a goniometer and the shoulder strength at flexion and at abduction was assessed with an Isobex Dynamometer (Cursor AG, Bern, Switzerland). All measurements were made at 90o in the scapular plane of abduction, and a maximum of 25 points was awarded for the ability to hold 11 kg or more at 90o in the plane of the scapula. Results were divided as “excellent”
(81-100 points), “good” (61-80 points), “fair” (41-60 points), and “poor” (< 40 points).
Objective outcome assessments were made by post
operative ultrasonography. Cuff integrity was classified into 3 categories; an intact cuff, a partialthickness tear, and a fullthickness tear, using the classification system by Naqvi et al. [12]. Further, cuff integrity was also classified according to the extent of fatty degeneration of rotator cuffs as described by Goutallier et al. [13].
Operative technique
After the patient was positioned in the lateral decubitus position, physical examination was performed under general anesthesia. Closed manipulation of the shoulder was performed before the operation. With the arm
positioned at 90˚ of abduction, the shoulder was externally rotated to 90˚ and then internally rotated to 90˚. Next, the arm was positioned into full elevation to 180˚. All of these procedures were performed while an assistant stabilized the scapula and no fractures were observed in our study.
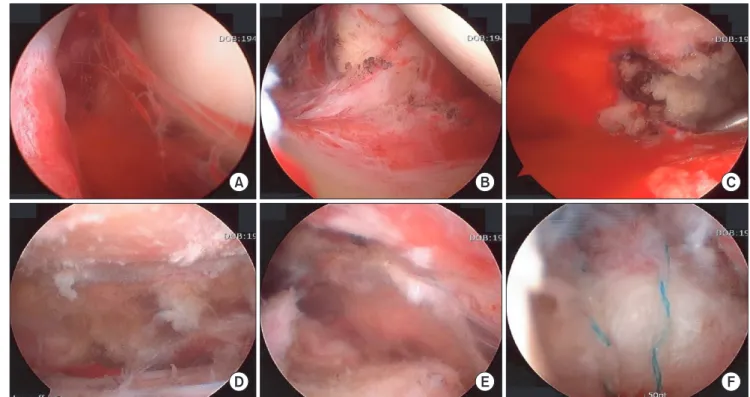
The arthroscope was then placed in the posterior portal, whereas a shaver and an electrocautery probe were inserted anteriorly. All inflamed tissue was debrided and electrocauterized. The capsular release was not performed in any cases. The subscapularis tendon and the biceps and glenohumeral ligaments were carefully preserved (Fig.
1A, B).
Next, the arthroscope was inserted into the subacromial space through the posterior portal. To alleviate bursitis, a thorough bursectomy was performed with a shaver.
Subacromial decompression was performed with a 5.0
mm burr through a lateral portal. A flat undersurface to the acromion was created (Fig. 1C, D). The extent of the tear was determined intraoperatively under direct arthroscopic visualization after debridement of the degenerated tendon edges. Mediallateral and anterior
posterior tension was tested with a cuff grasper. To achieve a repair that was as tension free as possible, we performed marginal convergence as needed after determining the
tear pattern. The bone bed of the footprint on the greater tuberosity was prepared with electrocautery, a power shaver, and a burr. The suture anchors were placed on the bone bed after we determined the number of anchors needed. The suture was passed 10 to 20 mm from the cuff margin with an antegrade suture passer (Viper; Arthrex, Naples, FL, USA) or a retrograde suture passer (Banana Lasso; Arthrex). The sutures for each anchor were “tied as you go” in a posterior to anterior direction or with an arthroscopic MasonAllen double row bridge repair technique, as suggested by Lee et al. [14] (Fig. 1E, F). After the surgery was completed, the glenohumeral joint and subacromial space were infiltrated with 10 mL of 0.5%
bupivacaine and 160 mg of triamcinolone acetonide into each site [15]. A sling with an abduction pillow was applied at the operating room on all patients, which the patient was instructed to wear fulltime, even when sleeping, for 6 weeks except when changing of clothes.
Passive stretching exercise was not allowed postoperative.
After 6 weeks, after allowing sufficient time to prevent re
tear, active and activeassisted exercises were begun in the same manner as usually performed for rotator cuff tears without stiffness (Table 1). No formal physical therapy was implemented. Immediate active motion was allowed in
Fig. 1. (A) After manipulation, arthroscopic findings showed hemarthrosis and inflammation of the shoulder joint. (B) Arthroscopic joint debridement was performed. (C) Arthroscopic findings showed severe bursitis and bleeding of the subacromial joint. (D) Arthroscopic debridement and acromioplasty were performed. (E) Arthroscopic findings showed a small rotator cuff tear. (F) The arthroscopic repair technique was performed.
the elbow, wrist, and digits. The return to full, unrestricted activities usually began at 3 to 6 months postoperatively and was based on the initial size of the tear, the strength of the repair, and the patient’s rehabilitation progress. The rehabilitation protocol for patients with shoulder stiffness did not differ from that of patients without shoulder stiffness.
Statistical analysis
The nonparametric Wilcoxon signed rank test was used as appropriate to assess differences between the pre and postoperative means. The level of statistical significance was set to Pvalue < 0.05 (5%). All analyses were performed with SPSS version 15.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
According to the classification of DeOrio and Cofield [10], there were 11 small tears, 6 mediumsized tears, and 1 large tear. The mean followup period was 20.2 months (range, 12-60), and the mean duration of symptoms before surgery was 5.5 months (range, 3-24).
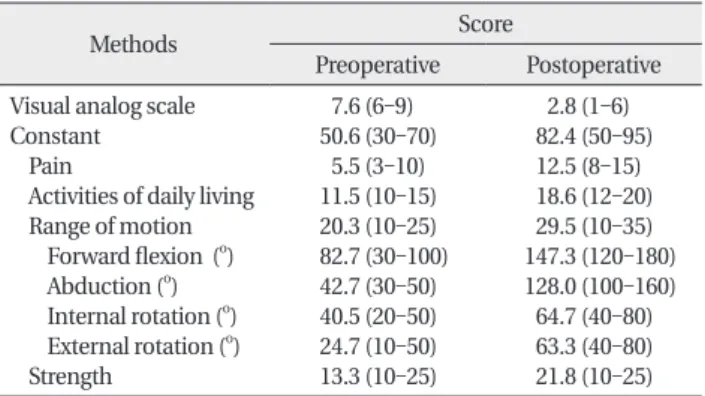
The mean VAS score improved from 7.6 (range, 6-9)
points preoperatively to 2.8 (range, 1-6) points at the last followup (P < 0.001). The mean Constant score improved from 50.6 (range, 30-70) points to 82.4 (range, 50-95) points (P < 0.001). The mean preoperative FF was 82.7o; abduction, 42.7o; internal rotation, 40.5o; and ER, 24.7o. The mean postoperative FF was 147.3o; abduction, 128o; internal rotation, 64.7o; and ER, 63.3o. The mean strength score improved from 13.3 (range, 10-25) points to 21.8 (range, 10-25) points (P < 0.001). There was a significant improvement in all VAS and Constant scores compared with the preoperative values (Table 2).
The functional results of the 18 patients were in 9 cases
“excellent”, 5 cases “good”, 2 cases “fair”, and 2 cases
“poor”. When divided into the shoulder stiffness, the mild stiffness group had 6 “excellent”, 1 “good”, 0 “fair”, and 0
“poor” functional results. The moderate stiffness group had 3 “excellent”, 1 “good”, 2 “fair”, and 0 “poor” functional results. The severe stiffness group had 0 “excellent”, Table 1. Summary of patients’ characteristics
Cases Male : Female
Age (yr)
Followup period (mo)
Preoperative symptom duration (mo) DeOrio and Cofield classification Small
Medium Large
7 : 11 58.7 (48-72) 20.2 (12-60) 5.5 (3-24)
11 6 1 Values are presented as number or mean (range).
Table 2. Functional results
Methods Score
Preoperative Postoperative Visual analog scale
Constant Pain
Activities of daily living Range of motion Forward flexion (o) Abduction (o) Internal rotation (o) External rotation (o) Strength
7.6 (6-9) 50.6 (30-70)
5.5 (3-10) 11.5 (10-15) 20.3 (10-25) 82.7 (30-100) 42.7 (30-50) 40.5 (20-50) 24.7 (10-50) 13.3 (10-25)
2.8 (1-6) 82.4 (50-95) 12.5 (8-15) 18.6 (12-20) 29.5 (10-35) 147.3 (120-180) 128.0 (100-160) 64.7 (40-80) 63.3 (40-80) 21.8 (10-25) Values are presented as mean (range).
All the Pvalue of each item was < 0.001.
Table 3. Functional results according to the degree of stiffness Preoperative
stiffness Excellent Good Fair Poor
Overall (n=18) Mild (n=7) Moderate (n=6) Severe (n=5)
9 6 3 0
5 1 1 3
2 0 2 0
2 0 0 2 Constant classification: excellent, 81-100 points; good, 61-80 points;
fair, 41-60 points; poor, < 40 points.
Table 4. Repair integrity according to tear size of rotator cuff Preoperative
tear size Intact cuff Partialthickness tear
Fullthickness tear Overall (n=18)
Small (n=11) Medium (n=6) Large (n=1)
12 8 4 0
5 3 2 0
1 0 0 1 Naqvi classification: repaired rotator cuff integrities were classified into 3 categories; intact cuff, a partialthickness tear, and a fullthickness tear.
Table 5. Repair integrity according to fatty degeneration of rotator cuff Preoperative
fatty degeneration
Intact cuffa) (n=12)
Partialthicknessa) tear (n=5)
Fullthicknessa) tear (n=1) Grade 1 (n=11)b)
Grade 2 (n=6)b) Grade 3 (n=1)b) Grade 4 (n=0)b)
8 4 0 0
3 2 0 0
0 0 1 0
a)Naqvi classification of rotator cuff after repair of the rotator cuff.
b)Goutallier classification of fatty degeneration: grade 0, no fatty deposits; grade 1, some fatty streaks; grade 2, more muscle than fat;
grade 3, as much muscle as fat; grade 4, less muscle than fat.
3 “good”, 0 “fair”, and 2 “poor” functional results; how ever, none of these 5 patients underwent a revision mani pu
lation or surgery (Table 3).
Repair integrities as determined by Naqvi classification were 12 cases of intact cuffs, 5 cases of partialthickness tears, and 1 case of fullthickness tear (Table 4). Presence of repair integrities according to the fatty degeneration of rotator cuff were 11 cases (of 11) of grade 1, 6 cases (of 6) of grade 2, and 0 cases (of 1) of grade 3 (Table 5).
DISCUSSION
Open or arthroscopic rotator cuff repairs have been considered contraindicated in patients with stiffness because postoperative stiffness may lead to poor func
tional outcomes. Postoperative stiffness is the one of the most common complication of rotator cuff repair, and this is reported to be closely related to the presence of preoperative stiffness or longterm immobilization because rotator cuff repair is regarded as a shoulder tightening procedure [16]. It is well known that post
operative stiffness leads to discouraging or poor functional outcomes.
With respect to defining a stiff shoulder, there is still an unresolved controversy as to whether the position of the arm is on the side or with 90o abduction when measuring ER to determine stiffness [17]. As done by Brislin et al. [9], we defined shoulder stiffness as total active and passive FF of < 100o, and total passive ER of < 30o with the arm in 90o of abduction, because we thought these limits, which are 50% of the range of a normal shoulder, were more clinically acceptable considering the patients’ daily lives.
Although the ideal preoperative state of the shoulder stiffness at the time of repair of rotator cuff tears is full recovery of motion after conservative treatment, there is no set level of acceptable stiffness at the time of cuff repair.
Generally, in the 2stage treatment of rotator cuff tears with shoulder stiffness, the rotator cuff repair is performed after recovery of passive ROM. However, it is difficult to obtain full recovery of passive motion preoperatively.
Some patients may withdraw from rehabilitation due to severe pain during stretching exercises, while others withdraw as their shoulder pain fails to improve. This may be due to an underlying pathology such as an impingement syndrome or a rotator cuff tear.
Chuang et al. [15] reported the results of onestage treatment of rotator cuff tears and shoulder stiffness by arthroscopic capsular release, manipulation, and
rotator cuff repair, and noted that overall satisfactory results were achieved. In their study, the results did not differ significantly between patients with and without shoulder stiffness. They noted that a secure repair of the rotator cuff is fundamental to the success in immediate postoperative stretching exercises. Chuang et al. [15]
reported that a rapid recovery and an improvement of ROM can be achieved by using a single arthroscopic repair. They performed concomitant rotator cuff repair and passive stretching exercises immediately after surgery and achieved overall satisfactory results with or without capsular release. Cho and Rhee [18] reported that after a single arthroscopic surgery with concomitant mani
pulation for patients with fullthickness rotator cuff tears and stiffness, the final outcomes were as good as those in patients without stiffness, but the return of ROM took longer in those patients undergoing mani
pulation. Capsular release was not performed, and full ROM was still not achieved at the last followup. In general, arthroscopic capsular release allows a visually controlled release of the capsule and ligaments, reducing the potential complications of a more traumatic manipulation.
Intrinsic rotator cuff degeneration and outlet or extrinsic acromial spur impingement are reportedly the major causes of rotator cuff lesions. Arthroscopic findings indicate that articular side tears are mainly associated with intrinsic degenerative changes, whereas bursal side tears are associated with subacromial impingement by extrinsic acromial spurs. Therefore, management of both extrinsic subacromial impingement and intrinsic degeneration of the rotator cuffs are principle approaches to treat rotator cuff lesions or tears. The most important finding of rotator cuff repairs was the high rate of retear.
To prevent retear, double row repair rather than single row repair and 6weeks immobilization than immediate passive exercise should be adopted.
Frozen shoulders and preoperative stiffness with rotator cuff tears share some common features. Ko and Wang [19] reported that primary and secondary shoulder stiffness may have similar etiology and clinical course.
The possible causes of primary and secondary shoulder stiffness that was suggested were age (between 40 to 60 years old age), minor traumatic incident, diabetes (10%- 20% of diabetes), cardiac disease, pulmonary disease, and neurologic conditions. They found similar expressions of inflammatory cytokines and myofibroblasts in the joint capsule and bursa. They also found that secondary
shoulder stiffness usually persisted longer if the underly
ing pathology did not improve. Therefore, they concluded that these different types of shoulder disorders might share a similar pathological mechanism and that pre
operative stiffness is not a predisposing factor for post
operative stiffness.
An interesting finding in our study was the effect of the rehabilitation protocol after rotator cuff repair and manipulation. The relationship between rehabilitation after rotator cuff repair and the development of post
operative stiffness is still debatable. Trenerry et al. [20]
reported that patients with restricted motion for 6 weeks after rotator cuff repair were no different in FF and ER compared with their nonstiff cohort by 76 weeks after surgery. In line with this, Parsons et al. [21] reported that delayed rehabilitation after arthroscopic rotator cuff repair is justifiable, and early restriction of ROM does not lead to longterm stiffness after arthroscopic rotator cuff repair, even in patients who are clinically stiff in the early postoperative period. As such, the immobilization period might be somewhat long in patients with large to massive tears, even with stiff shoulders. We also believe that stiffness can be resolved after arthroscopic release and manipulation, even in patients who were on abduction brace for 6 to 8 weeks. Even though postoperative stiffness is one of the most common complications, a retear has more serious functional consequences than stiffness.
Oh et al. [22] conducted a retrospective comparative
study of patients with and without preoperative shoulder stiffness. They found that mild or moderate preoperative shoulder stiffness does not affect the clinical outcomes of rotator cuff repair if arthroscopic capsular release with manipulation is added to the cuff repair procedure. In those patients with stiffness, only arthroscopic anterior release of the capsule was performed, whereas posterior and inferior releases were not used.
Our study has some limitations. First, we evaluated a small number of patients over a relatively short followup period. Studies that include a greater number of patients and a longer followup period are required to verify our findings. Second, we did not compare our findings with those of a control group without shoulder stiffness. Finally, this was a retrospective study based on observations of outcomes in a case series of patients who underwent a specific surgery.
We achieved overall satisfactory results in most patients, except for those with severe preoperative stiffness. So, we suggest that closed manipulation and arthroscopic rotator cuff repair could be a simple and an effective surgical treatment for rotator cuff tears with stiffness.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Tauro JC. Stiffness and rotator cuff tears: incidence, arthroscopic findings, and treatment results. Arthroscopy 2006;22:581-6.
2. Weber SC, Abrams JS, Nottage WM. Complications associated with arthroscopic shoulder surgery. Arthroscopy 2002;18(2 Suppl 1):88-95.
3. Chung SW, Huong CB, Kim SH, Oh JH. Shoulder stiffness after rotator cuff repair: risk factors and influence on outcome.
Arthroscopy 2013;29:290-300.
4. Bhatia S, Mather RC 3rd, Hsu AR, et al. Arthroscopic manage- ment of recalcitrant stiffness following rotator cuff repair: a retrospective analysis. Indian J Orthop 2013;47:143-9.
5. Denard PJ, Lädermann A, Burkhart SS. Prevention and management of stiffness after arthroscopic rotator cuff repair:
systematic review and implications for rotator cuff healing.
Arthroscopy 2011;27:842-8.
6. Namdari S, Green A. Range of motion limitation after rotator cuff repair. J Shoulder Elbow Surg 2010;19:290-6.
7. Holloway GB, Schenk T, Williams GR, Ramsey ML, Iannotti JP.
Arthroscopic capsular release for the treatment of refractory postoperative or post-fracture shoulder stiffness. J Bone Joint Surg Am 2001;83:1682-7.
8. Huberty DP, Schoolfield JD, Brady PC, Vadala AP, Arrigoni P, Burkhart SS. Incidence and treatment of postoperative stiffness following arthroscopic rotator cuff repair. Arthroscopy 2009;25:880-90.
9. Brislin KJ, Field LD, Savoie FH 3rd. Complications after arthro- scopic rotator cuff repair. Arthroscopy 2007;23:124-8.
10. DeOrio JK, Cofield RH. Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am 1984;66:563-7.
11. Constant CR, Murley AH. A clinical method of functional assess- ment of the shoulder. Clin Orthop Relat Res 1987;(214):160-4.
12. Naqvi GA, Jadaan M, Harrington P. Accuracy of ultrasonography and magnetic resonance imaging for detection of full thickness rotator cuff tears. Int J Shoulder Surg 2009;3:94-7.
13. Goutallier D, Postel JM, Gleyze P, Leguilloux P, Van Driessche S.
REFERENCES
Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears. J Shoulder Elbow Surg 2003;12:550-4.
14. Lee BG, Cho NS, Rhee YG. Modified Mason-Allen suture bridge technique: a new suture bridge technique with improved tissue holding by the modified Mason-Allen stitch. Clin Orthop Surg 2012;4:242-5.
15. Chuang TY, Ho WP, Chen CH, Lee CH, Liau JJ, Huang CH. Arthro- scopic treatment of rotator cuff tears with shoulder stiffness: a comparison of functional outcomes with and without capsular release. Am J Sports Med 2012;40:2121-7.
16. Warner JJ, Greis PE. The treatment of stiffness of the shoulder after repair of the rotator cuff. Instr Course Lect 1998;47:67-75.
17. Papalia R, Franceschi F, Vasta S, Gallo A, Maffulli N, Denaro V.
Shoulder stiffness and rotator cuff repair. Br Med Bull 2012;104:
163-74.
18. Cho NS, Rhee YG. Functional outcome of arthroscopic repair with concomitant manipulation in rotator cuff tears with stiff shoulder.
Am J Sports Med 2008;36:1323-9.
19. Ko JY, Wang FS. Rotator cuff lesions with shoulder stiffness:
updated pathomechanisms and management. Chang Gung Med J 2011;34:331-40.
20. Trenerry K, Walton JR, Murrell GA. Prevention of shoulder stiffness after rotator cuff repair. Clin Orthop Relat Res 2005;(430):94-9.
21. Parsons BO, Gruson KI, Chen DD, Harrison AK, Gladstone J, Flatow EL. Does slower rehabilitation after arthroscopic rotator cuff repair lead to long-term stiffness? J Shoulder Elbow Surg 2010;19:1034-9.
22. Oh JH, Kim SH, Lee HK, Jo KH, Bin SW, Gong HS. Moderate pre- operative shoulder stiffness does not alter the clinical outcome of rotator cuff repair with arthroscopic release and manipulation.
Arthroscopy 2008;24:983-91.