전염성 연속종의 한약 치료에 대한 임상 연구 동향 - 2000년대 이후 발표된 임상 연구 논문을 중심으로 -
도태윤․박슬기․이선행․이진용
경희대학교 대학원 소아과학교실
Received: October 25, 2018 ∙ Revised: November 16, 2018 ∙ Accepted: November 16, 2018 Corresponding Author: Lee Jin Yong
Pediatrics of Clinical Korean Medicine, College of Korean Medicine, Kyung Hee University, 23, Kyungheedae-ro, Dongdaemun-gu, Seoul, 130-872, Republic of Korea.
Tel: +82-2-958-9172, Fax: +82-2-958-9171 E-mail: [email protected]
ⓒ The Association of Pediatrics of Korean Medicine. All rights reserved. This is an open-access article distributed under the tenus of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Review of Clinical Studies of Herbal Medicine Treatment for Molluscum Contagiosum
Doh Tae Yun․Park Sul Gi․Lee Sun Haeng․Lee Jin Yong Department of Korean Pediatrics, Graduate School, Kyung Hee University Objectives
The purpose of this study is to investigate recent clinical studies on the effect of herbal medicine in molluscum contagiosum in China, and to seek better methods to treat and study for molluscum contagiosum in Korea.
Methods
We searched the clinical studies from the China Academic Journal (CAJ) in China National Knowledge Infrastructure (CNKI) by key words ‘传染性软疣’, ‘治疗’, ‘中医治疗’, ‘中药’ from January 2001 to August 2018.
We analyzed the literature in regards to the treatment methods and results.
Results
Among the 103 searched studies, 9 randomized controlled trials, 2 controlled clinical trials, and 16 case studies were selected and analyzed. In most of the studies, the effectiveness of herbal medicine on molluscum contagiosum was significantly high. The most commonly used herbs for oral administration were Isatidis Radix (板藍根), Coicis Semen (薏苡仁), Cyperi Rhizoma (香附子), Equiseti Herba (木賊), Poria (茯苓), Lithospermi Radix (紫草), Isatidis Folium (大靑葉) and Lonicerae Flos (金銀花). The most commonly used herbs for external applications were Isatidis Radix (板藍根), Lonicerae Flos (金銀花), Cyperi Rhizoma (香附子), Equiseti Herba (木賊), Dictamni Radicis Cortex (白 鮮皮), Isatidis Folium (大靑葉) and Brucea javanica (鴉膽子).
Conclusions
Based on the results of the clinical studies from China, the use of Korean medicine for treatment of molluscum contagiosum has been shown to be effective in relieving symptoms. Based on the result of this study, it will be possible to widen the scope of Korean medicine on infectious disease, such as molluscum contagiosum. Additional clinical studies and experimental studies need to be performed to solidify these findings.
Key words: Molluscum contagiosum, Herbal medicine, Chinese journal
대한한방소아과학회지 제33권 제1호(2019년 2월) J Pediatr Korean Med. February, 2019;33(1):1-16 ISSN 1226-8038(Print), 2287-9463(Online), https://doi.org/10.7778/jpkm.2019.33.1.01
Ⅰ. Introduction
전염성 연속종 (Molluscum contagiosum)은 Poxvirus 에 속하는 Molluscum contagiosum virus (MCV-1,2)에 의하여 발생되는 질환으로, 만성적인 국소 감염을 일 으킨다1). 임상적으로 중심부가 함몰된 직경이 2-5mm 의 둥근 반구형 구진이 특징인 전염성 질환이다2). 전염 성 연속종은 전 세계적으로 보고되고 있는 질환으로, 소아에서 흔한 질환이며, 미국에서는 전체 소아의 5%
이내에서 발생하는 것으로 보고되어 있다3).
전염성 연속종은 후천성 면역 결핍증 환자나 항암 치료, 면역 억제제 치료를 받는 성인에게 호발하는 것 으로 보고되어 면역기능 저하와 관계가 있는 것으로 알려져 있다4). 또한 전염성 연속종이 있는 환아에서 아 토피 피부염의 유병률이 일반적인 소아 인구집단에서 의 아토피 피부염의 유병률보다 훨씬 높게 나타나는 것으로 보고되는 등, 아토피 피부염과의 상관관계도 보고되고 있다5).
전염성 연속종은 Poxvirus에 속한 다른 많은 바이러 스들과 동일하게 직접적인 피부 접촉에 의하여 퍼지며, 병변 부위를 만지거나 긁는 등의 자가 접종에 의하여 퍼질 수 있다6). 성인에 있어서 성기 부위에 발생할 때 는 성전염성 질환으로 분류된다.
전염성 연속종의 서양 의학적 치료 방법으로는 냉 동요법 (Cryotherapy), 큐렛이나 작은 핀셋을 이용한 소 파술을 사용하거나 국소 발포제 (Topical blistering agent)인 Cantharidin9), 유사분열 억제제인 Podophyllotoxin10) 등이 최선의 치료법 (First-line therapy)으로 제시되고 있으며, 그 외에도 Imiquimod 등을 이용한 면역 치료
11,12)
등이 시도되고 있다. 전염성 연속종에 사용되는 서양 의학적 치료 중 냉동요법이나 소파술은 효과적이 긴 하지만, 국소적인 통증과 출혈을 종종 유발하며, 소 아가 치료에 순응하기 어려운 경우가 많다. 특히 문제 가 되는 것은 통증으로, 소아에 있어서 이는 질환 자체 보다 더 심각할 수 있다13). 따라서 서양 의학적 치료 외의 다른 치료법이 요구되고 있는 실정이다.
하지만 새로운 치료의 필요성에도 불구하고, 국내에 서 시행된 전염성 연속종의 한의학적 치료에 대한 임 상연구는 그 수가 매우 적은 편으로, Hwang 등14)과 Kim 등15)의 한약 치료 증례 보고, Park 등의 봉약침16), Sweet Bee Venom17)을 이용한 증례 보고 이외의 연구가 존재하지 않아 전염성 연속종의 한의학적 치료에 대한
연구가 부족한 실정이다.
이에 비해서 중의학에서는 전염성 연속종에 한의학 적 치료가 적용되고 있음을 검색을 통하여 확인하였기 에, 본 연구에서는 중국에서 2000년도 이후에 진행되 고 있는 전염성 연속종의 한약 치료에 대한 임상 연구 를 분석하여 치료 동향 및 유효성을 평가하고, 향후 전 염성 연속종에 대하여 한약 치료를 적용할 수 있는 기 본적인 자료로 삼고자 한다.
Ⅱ. Materials and Methods
1. 문헌 검색
문헌 검색의 검색원으로는 중국의 전자 데이터베 이스 검색 사이트인 중국학술정보원 (China National Knowledge Infrastructure, CNKI)을 사용하였다. 검색범 위는 醫藥衛生科技에서 中醫學, 中藥學, 中西醫結合 에 한정하였고, 검색 기간은 2000년 1월부터 2018년 8월까지 출판된 문헌으로 범위를 정하였다. 검색어는 질병명인 ‘传染性软疣’로 검색을 시행하였다. 그 후 in- tervention을 의미하는 ‘治疗’, ‘中医治疗’, ‘中药’을 사용 하였고, 결과 내 검색을 시행하여 최종적으로 문헌을 선택하였다. 중영문 교차 검색을 하였으며, 검색일은 2018년 8월 30일이었다.
2. 문헌 선택 및 제외 기준
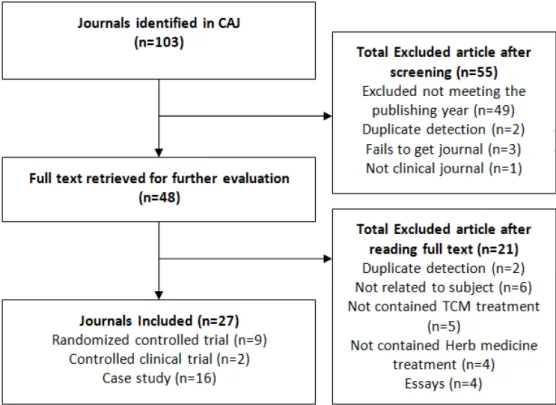
처음 ‘传染性软疣’를 사용하여 검색한 결과 총 103 편의 문헌이 검색되었고, 2000년 이전에 작성된 문헌 (49편)과 스크리닝을 통하여 중복된 문헌 (2편), 구할 수 없었던 문헌 (3편), 비논문 (1편)을 1차로 배제하여 총 48편의 문헌이 1차로 검색되었다. 이 후 연구자가 문헌의 전체를 검토하여 중복된 문헌 (2편), 전염성 연 속종 외의 다른 질환이 포함된 문헌 (6편), 한의학적 치 료가 사용되지 않은 문헌 (5편), 한약 치료 외의 다른 한의학적 치료를 사용한 문헌 (4편), 의안 (4편)을 제외 하였다. 한약 치료의 경우 내복, 외용, 혼합 치료로 분 류하였으며, 혼합 치료의 경우, 한약 내복과 외용의 병 행 치료, 한약 내복과 소파술의 병행 치료 이외의 다른 치료를 한 경우 문헌 선택에서 제외하였다. 이렇게 총 27편의 문헌을 고찰 대상 문헌으로 선정하였다. 이 중 Randomized controlled trial (RCT)은 9편, Controlled clinical trial (CCT)은 2편, Case study는 16편이었다 (Fig. 1).
전염성 연속종의 한약 치료에 대한 임상 연구 동향 -2000년대 이후 발표된 임상 연구 논문을 중심으로- 3
3. 자료수집 및 추출항목
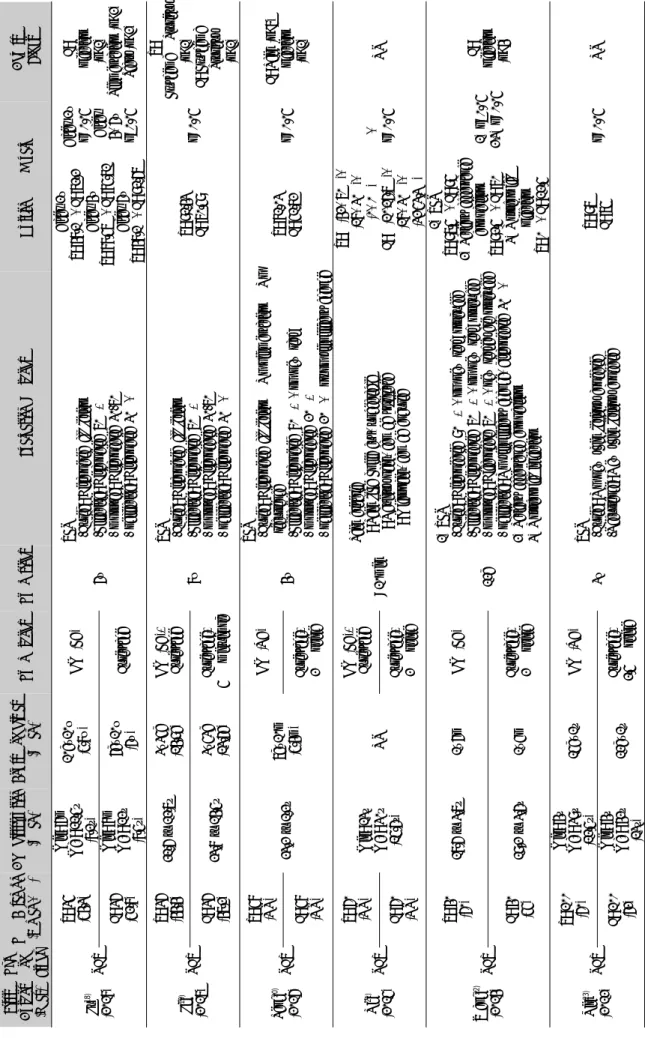
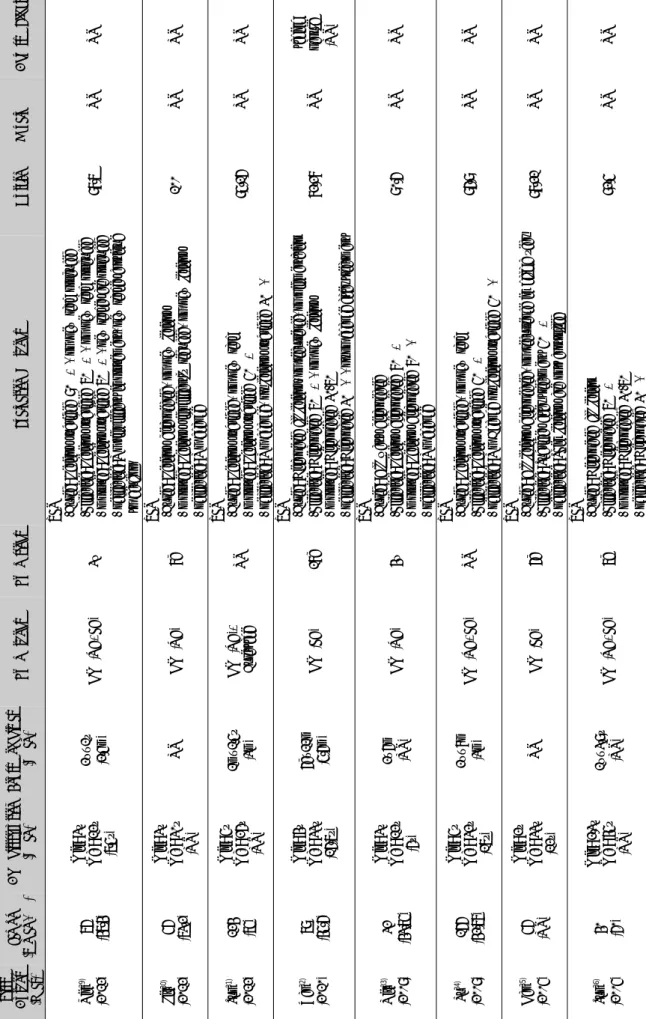
선정된 문헌을 대상으로 최신 연도의 문헌을 처음 으로 하여 자료를 수집하였다. 각 문헌에서 연구 대상 의 인구통계학적 정보, 치료 방법, 치료 기간, 평가 지 표와 치료 결과 및 기타 항목에 관한 정보를 추출하였 으며, 이를 요약하여 RCT, CCT 문헌에 대한 표 (Table 1)와 Case study 문헌에 대한 표 (Table 2)로 정리하였다.
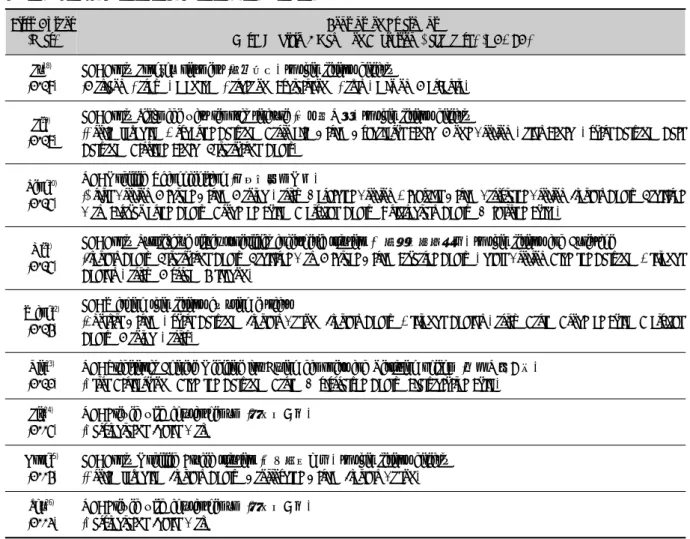
그리고 세 종류 문헌에서 중재로 사용된 한약 치료의 방법은 각각 따로 표로 정리하였다 (Table 3, 4, 5).
또한 정리한 표를 토대로 전염성 연속종의 한약 치 료 중 내복 치료, 외용 치료에 사용된 본초를 빈도별로 각각 정리하였다 (Table 6, 7).
Ⅲ. Results
1. 연도별 분포
연도별 분포는 RCT의 경우 2018년 1편18), 2017년 1편19), 2016년 1편20), 2015년 1편21), 2014년 1편22), 2012년 1편23), 2005년 1편24), 2004년 1편25), 2003년 1 편26)이었다. CCT의 경우 2004년 1편27), 2001년 1편28) 으로 나타났으며, Case study의 경우 2012년 3편29-31),
2010년 1편32), 2009년 2편33,34), 2005년 2편35,36), 2003년
2편37,38), 2002년 2편39,40), 2001년 4편41-44)으로 나타났다.
2. 연구 대상, 질병 이환 기간 및 치료 기간
전염성 연속종의 치료 대상이 되는 환자의 연령은 Mean ± Standard deviation의 형태로 제시한 연구가 4편
19,20,22,41)
, 연령의 최솟값, 최댓값을 제시하고 평균을 표 시한 연구가 13편18,21,23,27,29,32,33-35,37,38,42,44)
, 연령의 최솟 값과 최댓값만을 표시한 연구가 9편24,26,28,30,31,36,39,40,43)
으로 나타났다. 환자의 연령을 표시하지 않은 연구도 1편25) 있었다. 연구 대상의 연령은 연구마다 다양하게 나타났으며, 그 중 최소 연령은 생후 6개월이 된 환아 였으며, 최대 연령은 58세 환자였다.
전염성 연속종의 질병 이환 기간 (Course of disease) 은 Mean ± Standard deviation의 형태로 제시한 연구 1 편19), 질병 이환 기간의 최솟값, 최댓값을 제시하고 평 균을 표시한 연구가 7편18,20,29,31,32,34,42)
, 질병 이환 기간 의 최솟값, 최댓값만을 표시한 연구가 11편22-24,26,28,33,35, 36,39,43,44)
, 질병 이환 기간을 범위로 나누어 층화시켜 표 시한 연구가 1편38)으로 나타났다. 질병 이환 기간을 제 시하지 않은 경우도 7편21,25,27,30,35,40,41)
있었다. 질병 이 환 기간 또한 연구마다 다양하게 나타났으며, 질병 이 환 기간의 최솟값은 3일, 최댓값은 3년이었다.
Fig 1. Flow chart of the Chinese journals selection process
First Author (Year)
Type of StudyT & C sample (Female. %)Age distribution (Mean)Course of disease (Mean)Tx methodsTx periodsEvaluation MethodsOutcome & P valueAdverse Effect Lu18) (2018)RCT T: 35 (54.3) Min: 6m Max: 11.5y (8.1y)
10d~10w (5.8w)HM (EA) 6w TER -Cured: Disappered all lesion -Effective: Disappered 70%↑ -Improved: Disappeared 30-70% -Ineffective: Disappared 30%↓
After 2w T: 48.1%, C: 72.2% After 4w T: 88.57%, C: 85.71% After 6w T: 48.1%, C: 91.67%
After 2w p<0.05 After 4, 6w p>0.05 C: Infection (n=1) Pigmentation (n=2) Scars (n=2)C: 36 (52.8)
Min: 8m Max: 12y (8.5y)
6d~10w (6w)Curettage Li19) (2017)RCT
T: 36 (44.4)21.6 ± 12.7y3~35d (14.9d)HM (EA)+ Curettage 8w TER -Cured: Disappered all lesion -Effective: Disappered 70%↑ -Improved: Disappeared 30-70% -Ineffective: Disappared 30%↓
T: 91.43% C: 70.59%p<0.05 T: Erythema & Pruritus (n=1) C: Erythema & Pruritus (n=1)
C: 36 (47.2)23.8 ± 14.5y3~53d (13.6d)Curettage+ 5% Imiquimod Peng20) (2016)RCT T: 58 (NR) 23.2 ± 1.2y7d~10m (5.4m)
HM (OA) 4w
TER -Cured: Disappered all lesion & No pigmentation & No recurrence -Effective: Disappered 80%↑, no new rash -Improved: Disappeared 20%↑ -Ineffective: Disappared 20%↓ or no significant change
T: 81.03% C: 51.72%p<0.05C: Pain (n=7) Infection (n=1)C: 58 (NR)Curettage+ 2% Iodine Ni21) (2015)RCT
T: 60 (NR)Min: 13y Max: 30y (15.6y)NR HM (EA)+ Curettage <10min
Pain criteria I : Pain like knife cut, unbearable II : Obvious pain, can be tolerated III : Micropain, can be endured T: I (42, 70%), II (18, 30%), III (0, 0%) C: I (10,16.7%), II (18, 30%), III (32,53.3%)
I, III p<0.05NR C: 60 (NR)Curettage+ 2% Iodine Wang22) (2014)RCT
T: 40 (60)18.6 ± 3.7y1~6mHM (EA) 12d 1) TER -Cured: Disappeared 90%↑, no new rash produced -Effective: Disappeared 70%↑, no new rash produced -Improved: Diaappeard 70%↑, new rashes are produced -Ineffective: No significant change, disappeared 30%↓ 2) Patient acceptance comparison 3) Nosocomial infection 1) TER T: 97.5%, C: 95% 2) Patient acceptance comparison T: 92.5%, C: 70% 3) Nosocomial Infection T: 0%, C: 12.5%
1) p>0.05 2,3) p<0.05
C: Infection (n=4) C: 40 (55)19.2 ± 3.6y1~5mCurettage+ 2% Iodine Qin23) (2012)RCT
T: 100 (60) Min: 4y Max: 39y (12.5y)15d~1yHM (OA) 3wTER -Cured: No new skin lesions appeared -Recurrence: New skin lesions appeared
T: 97% C: 75%p<0.05NR C: 100 (62)
Min: 4y Max: 42y (13y)12d~1yCurettage+ 2.5% Iodine
Table 1. Analysis of Articles (RCTs and CCTs)
5
First Author (Year)
Type of StudyT & C sample (Female. %)Age distribution (Mean)Course of disease (Mean)Tx methodsTx periodsEvaluation MethodsOutcome & P valueAdverse Effect Liu24) (2005)RCT T: 49 (NR)Min: 18y Max: 39y (NR)1w~2m HM (OA)+ Curettage 5d TER -Cured: No new lesion -Effective: Number of new rash /Previous rash 10%↓ -Improved: Number of new rash /Previous rash 10~20% -Ineffective: Number of new rash /Previous rash 20%↑
T: 87.76% C: 53.33%NRNR C: 45 (NR)Curettage Kong25) (2004)RCT
T: 46 (NR) NRNR
HM (EA) 3w
TER -Cured: Completely subside, leaving pale red pigmentation or hypopigmentation -Effective: Subsides 50%↑, leaving carcass scars or small ulcers -Ineffective: Subsides 50%↓, continues to increase T: 97.83% C: 64.60%p<0.05 T: Pain (n=4) Burning sensation (n=37) Pigmentation (n=8) Hypopigmentation (n=6) Atrophy (n=3)
C: 42 (NR)0.5% peptide Butylamine Shu26) (2003)RCT
T: 49 (NR)Min: 19y Max: 39y (NR)1w~2m HM (OA)+ Curettage 5d TER -Cured: No new lesion -Effective: Number of new rash /Previous rash 10%↓ -Improved: Number of new rash /Previous rash 10~20% -Ineffective: Number of new rash /Previous rash 20%↑
T: 87.76% C: 53.33%p<0.05NR C: 42 (NR)Curettage Miao27) (2004)CCT60 (66.7)
Min: 12y Max: 29y (14.5y)NR
Group1: Curettage+ 2% Iodine 10min
Pain criteria I: Pain like knife cut, unbearable II: Obvious pain, can be tolerated III: Micropain, can be endured Group 1: I (45), II (15), III (0) Group 2: I (40), II (20), III (0) Group 3: I (12), II (16), III (32)
NRNR
Group2: Curettage+ HM (EA) Group3: Curettage+ 2% Iodine+ Lidocaine pad Jiang28) (2001)CCT97 (57.7)
Min: 11y Max: 50y (NR)NRHM (EA) 1wCured rate Cured: lesions diappearedT: 100% C: 100%NRNR Curettage T: Treatment, C: Control, M: Male, F: Female, TER: Total effective rate, RCT: Randomized controlled trial, CCT: Controlled clinical trial, NR: Not reported, HM: Herbal medicine, OA: Oral administration, EA: External application
First Author (Year)
Sample (Female. %)Age distribution (Mean)Course of disease (Mean)Tx methodsTx periodsEvaluation MethodsOutcome & P valueAdverse Effect Qin29) (2012)76 (47.4) Min: 3y Max: 12y (7.5y)
2w~1y (2.5m)HM (OA+EA)3w TER -Cured: Lesions subsided 90%↑, no new rash produced -Effective: Lesions subsided 70%↑, no new rash produced -Improved: Lesions subsided 70%↑, new rashes are produced -Ineffective: No significant improvement, new rashes continue to develop
98.7% NRNR Liu30) (2012)56 (73.2)
Min: 3y Max: 30y (NR)NRHM (OA)8d TER -Cured: Lesions disappeared, no new lesions -Improved: Lesions significantly reduced, no new lesions -Ineffective: No change
100% NRNR Sun31) (2012)124 (75)
Min: 5y Max: 26y (NR) 1m~1.5y (3m)HM (OA)+ CurettageNR TER -Cured: Lesions subsided, no new rash -Improved: Lesions subsided 50%↑ -Ineffective: No change, or lesions subsided 30%↓
95.16%NRNR Yan32) (2010)79 (45.6)
Min: 4y Max: 33y (16.7y) 6d~11m (5.6m)HM (EA)18d TER -Cured: Disappered all lesions, no recurrence, no pigmentation -Effective: Disappered 70%↑, no new lesions -Improved: Disappeared 30-70% -Ineffective: Disappared 30%↓, or no change after treatment
82.28%NRItching papule (NR) Niu33) (2009)32 (43.75)
Min: 3y Max: 12y (6y) 2~6m (NR)HM (OA)4w TER -Cured: All warts disappeared -Effective: Lesions disappeared 80%↑ -Improved: Lesions disappeared 80%↓ -Ineffective: No change
90.6%NRNR Pu34) (2009)166 (42.78)
Min: 5y Max: 32y (17y) 2w~8m (3m)HM (OA+EA)NR TER -Cured: Lesions subsided, no new rash -Effective: Lesions subsided 50%↑ -Ineffective: No Change or lesions subsided 50%↓
96.9%NRNR Han35) (2005)56 (NR)
Min: 2y Max: 33y (12y)NRHM (EA)6d TER -Cured: All lesions disappeared, no recurrence in half a year -Effective: Subsides after treatment 50%↑ -Ineffective: Skin lesions are not controlled
98.21%NRNR Sun36) (2005)40 (60)
Min: 2.3y Max: 45y (NR) 1w~3.9y (NR)HM (OA+EA)7d TER -Cured: Disappered all lesion -Effective: Disappered 70%↑ -Improved: Disappeared 30-70% -Ineffective: Disappared 30%↓
92.5%NRNR
Table 2. Analysis of Articles (Cases)