Cefepime-Induced Encephalopathy in a Tertiary Medical Center in Korea
INTRODUCTION
Cefepime is a widely used fourth-generation cephalosporin. It is commonly used as a first-line antibiotic to treat various infectious diseases such as neutropenic fever, urinary tract infections, hospital-acquired pneumonia, bacterial meningitis, and skin, intra-ab- dominal, and gynecological infections.
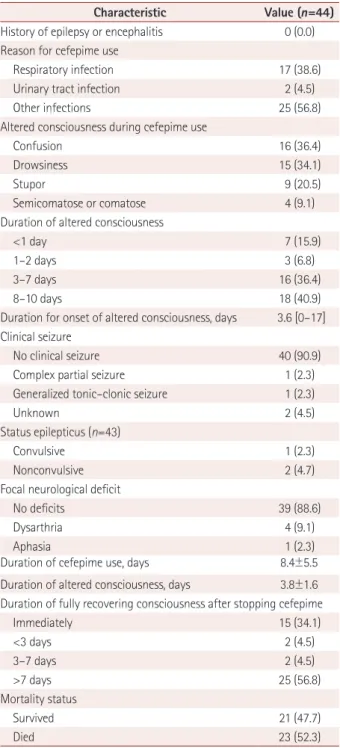
1The clinical features of cefepime-induced en- cephalopathy (CIE) are confusion, agitation, myoclonic jerks, epileptic seizures, coma, and convulsive status epilepticus.
2CIE was recently classified as a type-1 antibiotic-asso- ciated encephalopathy (AAE).
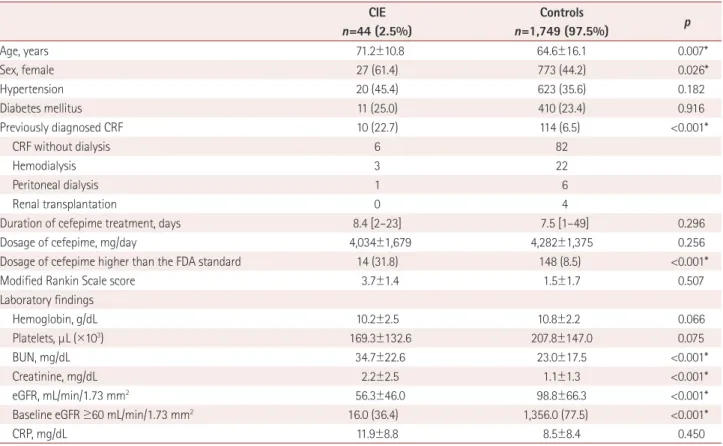
3In type-1 AAE, seizures are observed more frequently than in psychosis. Predisposing factors for CIE include a high cefepime dosage, reduced drug renal clearance, and older age.
4-6The reported incidence of CIE has ranged from 0.2% to 7.0%.
2,7-9Appa et al.
2reported an incidence at their center of 1 (0.2%) in 480 courses of cefepime. Naeije et al.
7reported Ji-Ye Jeon
a,bYong Won Cho
bHye-Jin Moon
b,ca
Department of Neurology, Kyungpook National University Chilgok Hospital, School of Medicine, Kyungpook National University, Daegu, Korea
b
Department of Neurology, Dongsan Medical Center,
Keimyung University School of Medicine, Daegu, Korea
c
Department of Neurology, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea
pISSN 1738-6586 / eISSN 2005-5013 / J Clin Neurol 2020;16(3):408-415 / https://doi.org/10.3988/jcn.2020.16.3.408
Received May 23, 2019 Revised March 12, 2020 Accepted March 16, 2020 Correspondence Hye-Jin Moon, MD Department of Neurology, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine,
170 Jomaru-ro, Bucheon 14584, Korea Tel +82-32-621-6569
Fax +82-32-621-5018
E-mail [email protected]
cc