Ⅰ. INTRODUCTION
Clear cell odontogenic carcinoma (CCOC) is often considered as a rare tumor, first described by Hansen in 1985.(1) Formerly known as clear cell odontogenic tumor, a locally aggressive benign tumor in the WHO classification of 1992,(2) it was renamed CCOC and classified among malignant tumors after the revision of this classification in 2005. It is still considered a malignant tumor in the 2017 classification.(3)
CCOC is an extremely rare neoplasm. It’s described very few in the English-language literature.(4,5) Thus, it is not easy to notice such disease. Also, treatment plan and procedures are uncertain to some clinicians.
CCOC has no specific clinical and radiographic features,
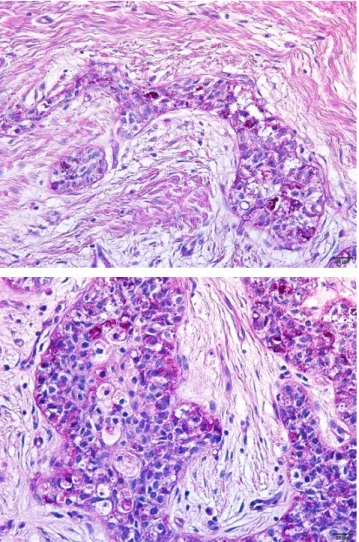
which make its diagnosis difficult. Histopathologically, CCOC is characterized by sheets and islands of vacuolated and clear cells(6) and by the presence of agglomerates of cells with eosinophilic cytoplasm. Long-term follow-up is suggested in the literature because of its potential for recurrence and distant metastases.(7)
This case report presents the histopathological and clinical features of clear cell odontogenic carcinoma excised from the mandible.
Ⅱ. CASE REPORT
A 53-year-old woman with good general health visited the oral and maxillofacial surgery department at the Seoul St.
Mary's Hospital of Catholic University of Korea, with paresthesia on #35 area. She was taking medicine for hypertension and
하악에 발생한 투명세포 치성암종: 증례 보고
이승준*, 최민호, 천승우, 이종호, 김창현, 박재억
가톨릭대학교 서울성모병원 구강악안면외과
<Abstract>
Clear Cell Odontogenic Carcinoma of the Mandible: A Case Report
Seung Joon Lee
*, Min Ho Choi, Seung Woo Cheon, Jong Ho Lee, Chang Hyen Kim and Je Uk Park Department of Oral and Maxillofacial Surgery, Seoul St. Mary’s Hospital, The Catholic University of Korea
Clear cell odontogenic carcinoma (CCOC) is an extremely rare odontogenic neoplasm; Only a few cases have been reported in the English literatures. It displays a propensity for the mandible, most commonly presenting in the fifth to seventh decades, with a female predilection. The clinical and radiological manifestations are multiple and the diagnosis is histological. Histological feature is of large islands and strands of uniform cells with round or ovoid nuclei and clear cytoplasm. Clinically, painless swelling is the most common symptom, followed by pain, teeth mobility, and paresthesia. CCOC has a good prognosis after surgery. This case report presents the histopathological and clinical features of CCOC excised from the mandible.
Key words : Clear cell odontogenic carcinoma, CCOC, Mandible
Korean Journal of Oral and Maxillofacial Pathology 2019;43(3):97-101 ISSN:1225-1577(Print); 2384-0900(Online) Available online at http://journal.kaomp.org https://doi.org/10.17779/KAOMP.2019.43.3.006
* Correspondence: Seung Joon Lee, Department of Oral and Maxillofacial Surgery, Seoul St. Mary’s hospital, The Catholic University of Korea Tel: +82-2-2258-1781, E-mail: [email protected]
ORCID: 0000-0003-0309-7429