pISSN 1598-2629 · eISSN 2092-6685
Stevens–Johnson Syndrome and Toxic Epidermal
Necrolysis Associated with Acetaminophen Use during Viral Infections
Ga-Young Ban
1,2, Seun-Joo Ahn
1, Hye-Soo Yoo
1, Hae-Sim Park
1and Young-Min Ye
1,2*
1Department of Allergy & Clinical Immunology, Ajou University School of Medicine, 2Ajou Regional Pharmacovigilance Center, Ajou University Hospital, Suwon 16499, Korea
http://dx.doi.org/10.4110/in.2016.16.4.256
INTRODUCTION
Cutaneous adverse drug reactions (ADR) range from trivial manifestations, such as morbilliform eruptions, to severe life-threatening reactions, including Stevens–
Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN). SJS/TEN is characterized by severe epithelial detachment of both the skin and mucosal membranes.
SJS/TEN is caused by drugs, infections, vaccination, malignant disorders, and radiotherapy (1,2). The principal drugs inducing SJS/TEN are antibacterial sulfonamides, beta-lactam antibiotics, anticonvulsants, non-steroidal anti-inflammatory drugs, and allopurinol (1,2). SJS/TEN can also be developed by interactions between drugs and viral infections.
Viruses interact with the immune system and can trigger severe cutaneous adverse reactions (SCAR) in several ways (3). Viral infections can influence drug metabolism, drug presentation to lymphocytes by dendritic cells, and production of cytokines/chemokines during the course of mounting an effector response by the infected host (3).
Cells of the innate immune system (principally dendritic cells) are activated by a variety of signals, including pathogen-associated-molecule patterns and bacterial and viral genomes via Toll-like receptors. Mature antigen- presenting cells activated in this manner effectively initiate T-cell responses (3). The CD137 protein expressed by monocytes co-operates with CD137L of CD8+ T-cells to expand the numbers of the latter cell type, which play a major role in the development of SJS/TEN (4).
Received on February 19, 2016. Revised on May 18, 2016. Accepted on May 30, 2016.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.
org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
* Corresponding Author. Young-Min Ye, Department of Allergy & Clinical Immunology, Ajou University School of Medicine, Ajou Regional Pharmacovigilance Center, Ajou University Hospital, Worldcup-ro 164, Youngtong-gu, Suwon 16499, Korea. Tel: 82-31-219-5150; Fax: 82-31-219-5154;
E-mail: [email protected]
Abbreviations: ADR, Adverse drug reaction; IVIG, Intravenous immunoglobulin; MIF, Macrophage migration inhibition factor; SCAR, Severe cutaneous adverse reactions; SJS, Stevens–Johnson syndrome; TEN, Toxic epidermal necrolysis
An association between drug treatment for viral infections and severe cutaneous adverse reactions has been noted. We investigated six patients diagnosed with Stevens–Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) after being prescribed acetaminophen for suspected viral illnesses. Multiplex analysis was performed to measure cytokine levels in sera before and after treatment. IL-2Ra levels significantly decreased during the convalescence phase.
Although acetaminophen is relatively safe, the drug can trigger SJS/TEN in patients with suspected viral infections.
T-cells and monocytes may be key components of the link between viral infection and acetaminophen-induced SJS/
TEN.[Immune Network 2016;16(4):256-260]
Keywords: Severe cutaneous adverse reaction, Acetaminophen, Viral infection
In the present study, we report six SJS/TEN patients that are suspected to be developed by interaction between acetaminophen and viral infection. The cytokine/
chemokine levels of activated T-cells and monocytes were measured in an effort to identify the possible serum biomarker that helps evaluating the therapeutic response or prognosis of SJS/TEN.
MATERIALS AND METHODS
Study subjects
Between December 2010 and January 2011, six patients were referred to the Allergy Clinic of Ajou University Hospital for treatment of fever and blistering lesions of the skin and mucosal membranes. Based on their drug exposure histories preceding the onset of symptoms and clinical presentations including erythematous macules progressing to vesicles/bullae and mucositis, we diagnosed one case of SJS and five cases of TEN (5).
We listed all drugs taken within 8 weeks prior to the development of SCAR and acetaminophen was considered to be the major culprit drug regarding the duration of medication intake or the latent period. All patients had taken acetaminophen for 3~7 days.
This study was approved by the Institutional Review Board of the hospital and written informed consent was obtained from the all subjects.
viral markers
Complete differential blood cell counts, serologic study of cytomegalovirus (CMV), Epstein-Barr virus (EBV), and human immunodeficiency virus (HIV) were performed.
Polymerase chain reaction (PCR) assays for influenza virus and CMV were also conducted.
Multiplex analysis for measuring cytokines
The serum levels of the following cytokines/chemokines were measured: regulated on activation normal T-cell expressed and secreted (RANTES), tumor necrosis factor-a (TNF-a), monocyte chemotactic peptide-1 (MCP-1), macrophage migration inhibition factor (MIF), interleukin-2 receptor a (IL-2Ra), and interleukin-10 (IL- 10). Sera were obtained before and after treatment and all tests were performed using a Bio-Plex ProTM Assays multiplex platform (Bio-Plex; Bio-Rad Laboratories, Hercules, CA, USA).
RESULTS
Clinical manifestations of the 6 patients with SJS/TEN probably induced by acetaminophen ingestion
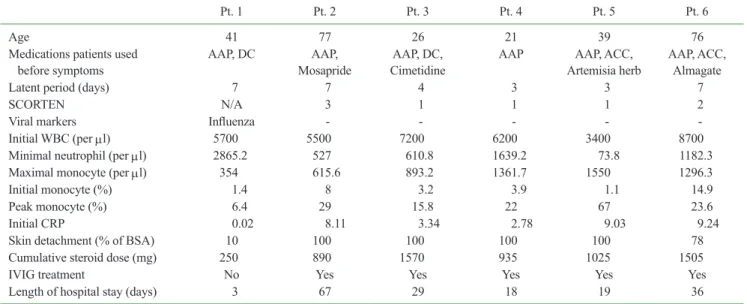
The mean severity-of-illness score for TEN (SCORTEN) (6) was calculated within the first 24 h after admission (Table I). All patients had constitutional symptoms suggestive of viral infection before commencement of acetaminophen treatment. One patient with SJS (Patient 1)
Table I. Clinical characteristics of the study subjects
Pt. 1 Pt. 2 Pt. 3 Pt. 4 Pt. 5 Pt. 6
Age 41 77 26 21 39 76
Medications patients used
before symptoms AAP, DC AAP,
Mosapride AAP, DC,
Cimetidine AAP AAP, ACC,
Artemisia herb AAP, ACC, Almagate
Latent period (days) 7 7 4 3 3 7
SCORTEN N/A 3 1 1 1 2
Viral markers Influenza - - - - -
Initial WBC (per ml) 5700 5500 7200 6200 3400 8700
Minimal neutrophil (per ml) 2865.2 527 610.8 1639.2 73.8 1182.3
Maximal monocyte (per ml) 354 615.6 893.2 1361.7 1550 1296.3
Initial monocyte (%) 1.4 8 3.2 3.9 1.1 14.9
Peak monocyte (%) 6.4 29 15.8 22 67 23.6
Initial CRP 0.02 8.11 3.34 2.78 9.03 9.24
Skin detachment (% of BSA) 10 100 100 100 100 78
Cumulative steroid dose (mg) 250 890 1570 935 1025 1505
IVIG treatment No Yes Yes Yes Yes Yes
Length of hospital stay (days) 3 67 29 18 19 36
AAP, acetaminophen; DC, dihydrocodeine; ACC, acetylcysteine; SJS, Stevens-Johnson Syndrome; TEN, toxic epidermal necrolysis; SCORTEN, severity-of-illness score for toxic epidermal necrolysis; WBC, white blood cell; CRP, C-reactive protein; BSA, body surface area; IVIG, intravenous immunoglobulin; Pt., patient; N/A, not available. Data are presented as mean±standard deviation (range) or n (%).
was confirmed to be infected with influenza virus. All of the five patients with TEN showed monocytosis or marked neutropenia within 1 week after admission. All patients were prescribed corticosteroids, and five TEN patients received intravenous immunoglobulin (IVIG) (2.0 g/
kg). Oseltamivir was prescribed to treat influenza for SJS patient. Although one patient was admitted to the ICU, there was no mortality.
Changes in serum cytokines/chemokine levels before and after treatment
The initial and recovery phase cytokine/chemokine levels
are shown in Fig. 1. Among 6 chemokines what we measured in the sera from the patients, only IL-2Ra was significantly decreased from the baseline. The levels of IL- 10 and TNF-a showed a tendency to be decreased in the recovery phase as compared with the baselines, however, because of small numbers of subjects, no statistical significance was obtained.
DISCUSSION
Some reports on possible interactions of viruses and
Figure 1. Comparison of serum cytokine levels before and after treatment in patients with Stevens–Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN). *p<0.05. RANTES, regulated on activation normal T-cell expressed and secreted; TNF-a, tumor necrosis factor-a; MCP-1, monocyte chemotactic peptide-1; MIF, macrophage migration inhibition factor; IL-2Ra, interleukin-2 receptor a; IL-10, interleukin-10 (Normal range: RANTES, 100.0~2282.0 pg/ml; TNF-a, 6.0~98.0 pg/ml; MCP-1, 2.0~48.0 pg/ml; MIF, 6.0~2003.0 pg/ml; IL-2Ra, 28.0~594.0 pg/ml; and IL-10, 0.4~2.0 pg/ml).
drugs in terms of induction of non-immediate cutaneous ADRs have appeared. Ampicillin-induced maculopapular exanthema developing in patients with infectious mononucleosis, and the increased risks of development of SCAR in AIDS patients, are well-known examples of such interactions (7). In the absence of concurrent viral infection, the suspect drugs did not stimulate T-cell proliferation in patients showing SCAR (8). Although drugs are widely accepted to be leading causes of SJS/
TEN, acetaminophen is generally recognized to be safe, and rarely associated with development of SCAR (9).
Based on the previous studies that noted viral infection can have synergistic immunologic effect on adverse drug reaction and previously reported drug lists with a risk to induce SJS/TEN (9,10), we report the six cases of SJS/
TEN whose major culprit was acetaminophen. Although changes in pharmacokinetics during viral infections and drug- and drug-metabolites-related toxicity has been noted in virally infected cells (7,10), however, immunological and pharmacological interactions between viruses and drugs remain to be elusive. Considering that flu was epidemic at that time in Korea, marked monocytosis, neutropenia, and a positive influenza PCR observed in their initial laboratory tests suggested that those patients were under viral infection which could make further activate their immune system against the causative drug (11,12). Typically, mean latent period between the exposure to culprit drugs and onset of the adverse drug reactions is 4~28 days (9,10,13). However, the reported latency times of TEN cases are varied depending on the causative drugs, combined medications, and conditions of the patients (10). Kim et al. reported that two cases of TEN associated with acetaminophen ingestion under upper respiratory tract infection (14). Similarly with our cases, TENs were developed within 2 to 3 days after medication with acetaminophen in the previous report (14). Taken together, we can speculate that although the acetaminophen is an unusual offending drug of SJS/TEN, it is prone to cause SJS/TEN when it comes with viral infection.
Cytotoxic T-cells/monocytes play important roles in SJS/TEN development via Fas/Fas ligand, perforin, granzyme, granulysin and soluble apoptosis-inducing factors (e.g. TNF-a, IFN-g) (4). MIF and IL-2Ra trigger T-cell proliferation (2,15), in addition, RANTES and MCP-1 exert potent chemotactic effects on T-cells/
monocytes (16) and play role in SJS/TEN. In contrast, IL- 10 generated by T-regulatory cells plays a predominantly anti-inflammatory role by inhibiting the recognition function of dendritic cells (17). In the previous studies,
the levels of TNF-a, IL-2Ra, and IL-10 were increased in the sera of TEN patients (17), in addition, the RANTES level was significantly upregulated in the lesions caused by SCAR (18). MIF was suggested to be used to identify the drug adversely affecting TEN patients (19). In the present study, we found that the IL-2Ra level decreased significantly after treatment. Two patients (Patient 2 and 5) with remarkable decline in IL-2Ra levels visited our hospital 7 days after the onset of their skin lesions, in contrast, the remaining four visited within 2 days. This finding may explain why only two patients showed a greater decline in IL-2Ra levels. Patient 2 admitted to the ICU who stayed for the longest duration (67 days) showed the highest IL-2Ra level at baseline whereas the SJS patient (Patient 1) who stayed for the shortest duration (3 days) had the lowest IL-2Ra level at baseline.
Additionally, the baseline MCP-1 levels were found to have strong positive correlations with IL-2Ra and MIF levels (r=0.829, p=0.042, respectively) in the same individuals. These data are consistent with a previous study (17) that reported that more severe forms of SCAR resulted in higher production of inflammatory cytokines.
Our data collectively suggest that longer periods before appropriate treatment can increase IL-2Ra levels, thereby prolonging hospital stays. Taken together, measuring the IL-2Ra levels may be helpful to evaluate the therapeutic response and predict the prognosis of SCAR. Although it is possible that viral infections may interact with commonly administered medications or their metabolites to cause SCAR, much larger epidemiologic studies will be needed to prove these associations. Therefore, further studies, including larger numbers of patients, are required to elucidate the exact relationship of IL-2Ra, MCP-1 and MIF levels with clinical prognosis.
In conclusion, although acetaminophen is relatively safe, the drug can trigger SJS/TEN in patients with suspected viral infections. A large scale study regarding the role of measuring inflammatory cytokine/chemokine levels of activated T-cells/monocytes in evaluating therapeutic response and predicting the prognosis of SJS/TEN is warranted.
ACKNOwLEDGEMENTS
This research was supported by a grant from the Ministry of Food and Drug Safety to operation of the Regional Pharmacovigilance Center in 2016.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES
1. Letko, E., D. N. Papaliodis, G. N. Papaliodis, Y. J. Daoud, A.
R. Ahmed, and C. S. Foster. 2005. Stevens-Johnson syndrome and toxic epidermal necrolysis: a review of the literature. Ann.
Allergy Asthma Immunol. 94: 419-436.
2. Pereira, F. A., A. V. Mudgil, and D. M. Rosmarin. 2007. Toxic epidermal necrolysis. J. Am. Acad. Dermatol. 56: 181-200.
3. Torres, M. J., C. Mayorga, and M. Blanca. 2009. Nonimmediate allergic reactions induced by drugs: pathogenesis and diagnostic tests. J. Investig. Allergol. Clin. Immunol. 19: 80- 90.
4. Tohyama, M., and K. Hashimoto. 2012. Immunological mechanisms of epidermal damage in toxic epidermal necrolysis. Curr. Opin. Allergy Clin. Immunol. 12: 376-382.
5. Harr, T., and L. E. French. 2010. Toxic epidermal necrolysis and Stevens-Johnson syndrome. Orphanet. J. Rare Dis. 5: 39.
6. Barron, S. J., M. T. Del Vecchio, and S. C. Aronoff. 2015.
Intravenous immunoglobulin in the treatment of Stevens- Johnson syndrome and toxic epidermal necrolysis: a meta- analysis with meta-regression of observational studies. Int. J.
Dermatol. 54: 108-115.
7. Shiohara, T., and Y. Kano. 2007. A complex interaction between drug allergy and viral infection. Clin. Rev. Allergy Immunol. 33: 124-133.
8. Blazquez, A. B., J. Cuesta, and C. Mayorga. 2011. Role of dendritic cells in drug allergy. Curr. Opin. Allergy Clin.
Immunol. 11: 279-284.
9. Kim, K. J., D. P. Lee, H. S. Suh, M. W. Lee, J. H. Choi, K.
C. Moon, and J. K. Koh. 2005. Toxic epidermal necrolysis:
analysis of clinical course and SCORTEN-based comparison of mortality rate and treatment modalities in Korean patients.
Acta Derm. Venereol. 85: 497-502.
10. Mockenhaupt, M. 2011. The current understanding of Stevens- Johnson syndrome and toxic epidermal necrolysis. Expert Rev.
Clin. Immunol. 7: 803-813.
11. Beldomenico, P. M., S. Telfer, S. Gebert, L. Lukomski, M.
Bennett, and M. Begon. 2008. Poor condition and infection:
a vicious circle in natural populations. Proc. Biol. Sci. 275:
1753-1759.
12. Segel, G. B., and J. S. Halterman. 2008. Neutropenia in pediatric practice. Pediatr. Rev. 29: 12-23.
13. Sohn, K. H., S. Y. Oh, K. W. Lim, M. Y. Kim, S. Y. Lee, and H. R. Kang. 2015. Sorafenib induces delayed-onset cutaneous hypersensitivity: a case series. Allergy Asthma Immunol. Res.
7: 304-307.
14. Kim, E. J., H. Lim, S. Y. Park, S. Kim, S. Y. Yoon, Y. J. Bae, H. S. Kwon, Y. S. Cho, H. B. Moon, and T. B. Kim. 2014.
Rapid onset of Stevens-Johnson syndrome and toxic epidermal necrolysis after ingestion of acetaminophen. Asia Pac. Allergy 4: 68-72.
15. Shimizu, T. 2005. Role of macrophage migration inhibitory factor (MIF) in the skin. J. Dermatol. Sci. 37: 65-73.
16. Alam, R. 1997. Chemokines in allergic inflammation. J.
Allergy Clin. Immunol. 99: 273-277.
17. Nomura, Y., M. Aihara, S. Matsukura, Y. Ikezawa, T. Kambara, Y. Aihara, Y. Takahashi, and Z. Ikezawa. 2011. Evaluation of serum cytokine levels in toxic epidermal necrolysis and Stevens-Johnson syndrome compared with other delayed-type adverse drug reactions. J. Dermatol. 38: 1076-1079.
18. Yawalkar, N., M. Shrikhande, Y. Hari, H. Nievergelt, L. R.
Braathen, and W. J. Pichler. 2000. Evidence for a role for IL-5 and eotaxin in activating and recruiting eosinophils in drug- induced cutaneous eruptions. J. Allergy Clin. Immunol. 106:
1171-1176.
19. Halevy, S., and E. Livni. 1997. The role of macrophage migration inhibition factor in toxic epidermal necrolysis. Int. J.
Dermatol. 36: 776-778.