ISSN 2234-3806 • eISSN 2234-3814
http://dx.doi.org/10.3343/alm.2016.36.4.371 www.annlabmed.org 371
Ann Lab Med 2016;36:371-374
http://dx.doi.org/10.3343/alm.2016.36.4.371
Letter to the Editor
Diagnostic Hematology
A Novel KIT INDEL Mutation in Acute Myeloid
Leukemia With t(8;21)(q22;q22); RUNX1-RUNX1T1
Jun Hyung Lee, M.D.1, Chungoo Park, Ph.D.2, Soo-Hyun Kim, M.D.1, and Myung-Geun Shin, M.D.1
Department of Laboratory Medicine1, Chonnam National University Medical School and Chonnam National University Hwasun Hospital, Hwasun; School of Biological Sciences and Technology2, Chonnam National University, Gwangju, Korea
Dear Editor,
KIT (also known as c-KIT) is a receptor tyrosine kinase ex- pressed on various cell types [1]. KIT mutations are detected in approximately 5% of patients newly diagnosed with acute my- eloid leukemia (AML) and in 20-30% of patients with core-bind- ing factor AML [2, 3]. KIT mutations are predominantly pre- sented as one or two amino acid substitutions affecting codon 816. The most frequent mutation type, D816V, is detected in about 40% of cases with AML, where KIT is mutated [4]. In AML with t(8;21), the presence of KIT mutation at codon 816 is associated with a high white blood cell (WBC) count at diagno- sis, a high incidence of extramedullary leukemia, and high risk of relapse during the course of the disease [5]. Other less fre- quent types of KIT mutation are D816Y, D816H, and D816I.
KIT mutations present a prognostic significance. The National Comprehensive Cancer Network categorized AML with either t(8;21) or inv(16)/t(16;16) combined with KIT mutations as the intermediate-risk group [6]. We report a novel INDEL mutation in KIT codon 816, discovered in a woman with AML with t(8;21) (q22;q22); RUNX1-RUNX1T1.
A 35-yr-old woman was admitted for purpura in both lower limbs. The initial complete blood cell count indicated: WBC count, 20.1 ×109/L; hemoglobin, 8.2 g/dL; and platelet count, 15×109/L. A peripheral blood smear revealed leukocytosis with
45% of blasts. The bone marrow (BM) aspirate smear and cyto- chemical stains showed an increased number of myeloblasts (68%) and other myeloid precursors (Fig. 1A). The 197 bp- sized transcript of RUNX1 exon 6/RUNX1T1 exon 2 was de- tected in a multiplex PCR analysis of BM aspirates. In the cyto- genetic study, the karyotype was 46,XX,t(8;21)(q22;q22) [18]/46,XX[2]. The patient was diagnosed with AML with t(8;21) (q22;q22); RUNX1-RUNX1T1. In the screening test for KIT mu- tations using a real-time allele-specific PCR kit (Real-Q C-KIT;
BioSewoom, Seoul, Korea), a mutation was detected, which was not the D816V, D816Y, or D816H type (Fig. 1B). Conventional sequencing was performed to identify the mutation. Unlike the common mutation types presenting one or two ambiguous bases in codon 816, the sequencing result showed five consec- utive ambiguous bases through codon 815–817 (Fig. 1C). Allele separation by T-vector cloning using pGEM-T Easy Vector Sys- tems (Promega, Madison, WI, USA) and additional conventional sequencing were performed and a missense INDEL mutation NM_000222.2:c.2445_2449delAGACAinsGTTAC (p.D816_
I817delinsLL) was confirmed. To the best of our knowledge, this mutation has not yet been reported.
Three in-silico prediction tools were utilized to predict the ef- fect of the mutation on the KIT protein function and stability (Ta- ble 1). Using SIFT (Sorting Tolerant From Intolerant, version 1.03,
Received: December 31, 2015 Revision received: February 16, 2016 Accepted: March 14, 2016
Corresponding author: Myung-Geun Shin
Department of Laboratory Medicine, Chonnam National University Medical School and Chonnam National University Hwasun Hospital, 322 Seoyang- ro, Hwasun-eup, Hwasun-gun, Jeollanam-do 58128, Korea
Tel: +82-61-379-7950, Fax: +82-61-379-7984 E-mail: [email protected]
© The Korean Society for Laboratory Medicine.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Lee JH, et al.
Novel KIT INDEL mutation in AML with t(8;21)
372 www.annlabmed.org http://dx.doi.org/10.3343/alm.2016.36.4.371 Fig. 1. (A) Bone marrow aspirate smear showing blasts presenting an abundant granular cytoplasm with perinuclear clearing, large orange- pink granules, and distinct Auer rods (Wright-Giemsa stain, ×1,000). (B) Result of real-time allele-specific PCR for KIT mutation (Real-Q C-KIT). The amplification curve of the patient sample (threshold cycle [Ct]: 29.4) and the amplification curve of positive control (Ct: 26.1) for KIT mutation screening are presented as the green and red line, respectively. The other amplification curves for KIT mutation genotyp- ing such as D816V, D816Y, and D816H are not shown (not amplified). Rn is the normalized fluorescence signal of the reporter dye and ΔRn is Rn minus the baseline. The threshold of ΔRn is 0.1 and the cutoff value for KIT mutation positive is less than or equal to 38 as Ct.
(C) Results of sequencing analysis of codon 815–817 of the KIT. The original sequence of the patient is presented (upper sequence) as well as the sequence of the wild-type allele after allele separation (middle sequence) and the sequence of the mutant allele after allele-sep- aration (lower sequence). (D) Results of the in-silico prediction of protein structure and characteristics by SABLE. Wild-type (upper struc- ture); D816V mutation (middle structure); D816_I817delinsLL mutation (lower structure). The highlighted background (blue) represents hydrophobic amino acids. The detail properties are explained in the POLYVIEW-2D documentation (http://polyview.cchmc.org/polyview_
doc.html).
A Amplification plot
Cycle B
C D
Lee JH, et al.
Novel KIT INDEL mutation in AML with t(8;21)
http://dx.doi.org/10.3343/alm.2016.36.4.371 www.annlabmed.org 373
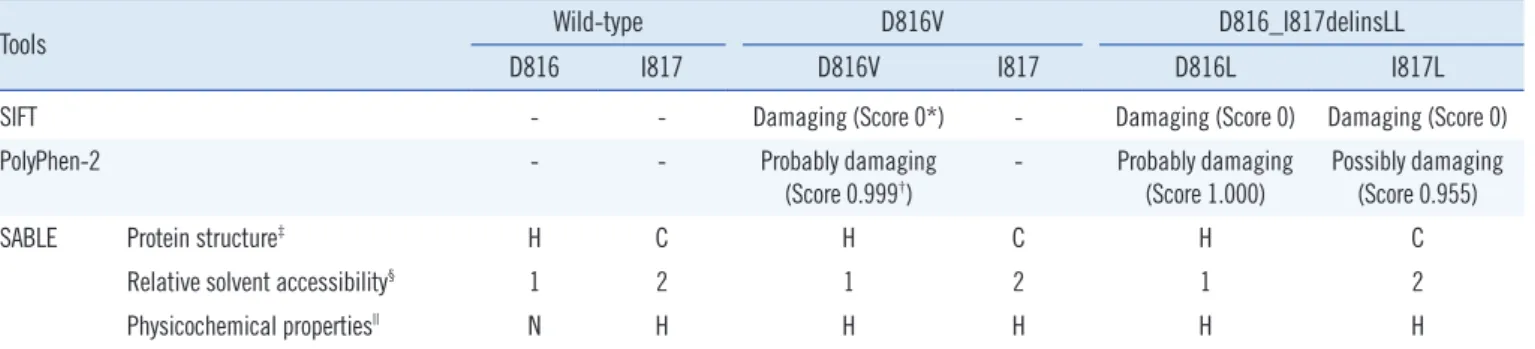
Table 1. Results of in-silico predictions about mutations in codon 816 and 817 of the KIT
Tools Wild-type D816V D816_I817delinsLL
D816 I817 D816V I817 D816L I817L
SIFT - - Damaging (Score 0*) - Damaging (Score 0) Damaging (Score 0)
PolyPhen-2 - - Probably damaging
(Score 0.999†) - Probably damaging
(Score 1.000) Possibly damaging (Score 0.955)
SABLE Protein structure‡ H C H C H C
Relative solvent accessibility§ 1 2 1 2 1 2
Physicochemical properties|| N H H H H H
*SIFT score: the amino acid substitution is predicted to be damaging when the score is ≤0.05, and tolerated when the score is >0.05; †PolyPhen-2 score is the probability of the substitution being damaging; ‡SABLE Protein structure: H (helix), E (beta strand), C (coil); §SABLE Relative solvent accessibility: level of exposure (0-completely buried, 9-fully exposed); ||SABLE Physicochemical properties: H-hydrophobic, N-negatively charged.
http://sift.jcvi.org/; J. Craig Venter Institute, La Jolla, CA, USA) [7], exploiting the degree of conservation of amino acid residues de- rived from functionally related protein sequences, D816L, I817L, and D816V mutations were predicted to be ‘damaging’, with a SIFT score equal to 0 (the amino acid substitution is predicted as ‘damaging’ if the score is ≤0.05). Using PolyPhen-2 (Poly- morphism Phenotyping v2, version 2.2.2, http://genetics.bwh.
harvard.edu/pph2/; Division of Genetics, Brigham & Women’s Hospital, Harvard Medical School, Boston, MA, USA) [8] to pre- dict the possible impact of an amino acid substitution on the structure and function of a protein using several features, includ- ing sequences, phylogenetic, and structural information, D816L and I817L were predicted to be ‘probably damaging’ with a score of 1.000, and ‘possibly damaging’ with a score of 0.955, respec- tively. By comparison, the D816V mutation was predicted to be
‘probably damaging’, with a score of 0.999. Using SABLE (Accu- rate prediction of Solvent AccessiBiLitiEs, version 2, http://sable.
cchmc.org/; Division of Biomedical Informatics, Children’s Hos- pital Research Foundation, Cincinnati, OH, USA) [9], which pre- dicts the relative solvent accessibility of amino acid residues and secondary structures in proteins using evolutionary profiles, the D816_I817delinsLL mutation was predicted to present physico- chemical properties similar to those of D816V when compared with both the wild-type and the D816V mutation (Fig. 1D). In the physicochemical property prediction, both D816V and D816_I817delinsLL were predicted to be hydrophobic, whereas the wild type D816 and I817 were predicted to be negatively charged and hydrophobic, respectively. Considering these in- silico prediction results, we concluded that the clinical signifi- cance of D816_I817delinsLL mutation would be similar to that of the pathogenic D816V mutation.
In the follow-up BM examination, one month after the induc- tion chemotherapy using idarubicin and cytarabine, the BM as-
pirate smear showed 14% of myeloblasts and the response was determined as resistant disease [10]. In the next follow-up BM examination, one month after re-induction chemotherapy using daunorubicin and cytarabine, 3% of myeloblasts were observed on the BM aspirate smear, and the patient was diagnosed with a morphological leukemia-free state.
This is the first report on a novel KIT INDEL mutation in exon 17, D816_I817delinsLL.
Authors’ Disclosures of Potential Conflicts of Interest
No potential conflicts of interest relevant to this article were re- ported.
Acknowledgments
This study was supported by the Leading Foreign Research In- stitute Recruitment Program (No. 2011-0030034) through the NRF funded by the Ministry of Education, Science and Technol- ogy (MEST), a grant from the National R&D Program for Cancer Control, Ministry of Health & Welfare, Republic of Korea (No.
2013-1320070) and grants from the Environmental Health Cen- ter funded by the Ministry of Environment, Republic of Korea.
REFERENCES
1. Lovly C, Sosman J, Pao W. KIT. My cancer genome. http://www.mycan- cergenome.org/content/disease/acute-myeloid-leukemia/kit/?tab=0 (Updated on Jun 16, 2015).
2. Patel JP, Gönen M, Figueroa ME, Fernandez H, Sun Z, Racevskis J, et al. Prognostic relevance of integrated genetic profiling in acute myeloid leukemia. N Engl J Med 2012;366:1079-89.
3. Döhner H, Weisdorf DJ, Bloomfield CD. Acute Myeloid Leukemia. N Engl J Med 2015;373:1136-52.
Lee JH, et al.
Novel KIT INDEL mutation in AML with t(8;21)
374 www.annlabmed.org http://dx.doi.org/10.3343/alm.2016.36.4.371 4. Wheeler S, Seegmiller A, Vnencak-Jones C. KIT c.2447A>T (D816V)
mutation in acute myeloid leukemia. http://www.mycancergenome.org/
content/disease/acute-myeloid-leukemia/kit/275/ (Updated on Sep 9, 2013).
5. Cairoli R, Beghini A, Grillo G, Nadali G, Elice F, Ripamonti CB, et al.
Prognostic impact of c-KIT mutations in core binding factor leukemias:
an Italian retrospective study. Blood 2006;107:3463-8.
6. National Comprehensive Cancer Network. Acute Myeloid Leukemia (Version 1.2015) http://www.nccn.org/professionals/physician_gls/pdf/
aml.pdf (Updated on Dec 3, 2014).
7. Kumar P, Henikoff S, Ng PC. Predicting the effects of coding non-syn- onymous variants on protein function using the SIFT algorithm. Nat Pro-
toc 2009;4:1073-81.
8. Adzhubei IA, Schmidt S, Peshkin L, Ramensky VE, Gerasimova A, Bork P, et al. A method and server for predicting damaging missense muta- tions. Nat Methods 2010;7:248-9.
9. Adamczak R, Porollo A, Meller J. Accurate prediction of solvent acces- sibility using neural networks-based regression. Proteins 2004;56:753- 67.
10. Cheson BD, Bennett JM, Kopecky KJ, Büchner T, Willman CL, Estey EH, et al. Revised recommendations of the international working group for diagnosis, standardization of response criteria, treatment outcomes, and reporting standards for therapeutic trials in acute myeloid leuke- mia. J Clin Oncol 2003;21:4642-9.