Hughes-Stovin syndrome is an extremely rare disease known to cause multiple pulmonary artery aneurysms (PAAs) and venous thrombosis (1, 2). The patients can develop massive hemoptysis and the disorder can result in death. Although the use of systemic corticosteroids with a combination of immunosuppressants has been the mainstay of treatment, interventional treatments are required for a life-threatening hemoptysis. However, a thrombosis in the central veins can impede catheter pas- sage. In this report, we describe the use of percutaneous transhepatic venous embolization through the hepatic vein due to occluded common vascular pathways to the pulmonary artery.
Case Report
The institutional review board approved the study re- ported here. A 42-year-old male patient was admitted with acute abdominal pain. The patient had a history of deep vein thrombosis on the left lower extremity nine months prior to presentation and had been taking war- farin. The patient had had a recurrent oral ulcer for 10 years, but a genital ulcer, eye lesion or skin lesion was not revealed. The blood pressure was 120/80 mmHg and the heart rate was regular at 96 beats per minute.
On physical examination, the abdomen was rigid and flat and direct tenderness was felt in the right upper quadrant area. Laboratory investigations revealed a he- moglobin value of 14.3 g/dL that decreased to 9.3 g/dL the next day, and a white blood cell count of 9,800/μL.
The prothrombin time was prolonged 30.8 sec (normal, 9.5-13.2 sec) due to the warfarin therapy. The amylase level was increased to 3263 IU/L (normal, 25-115 IU/L) from acute pancreatitis probably due to a mass effect of a hematoma. A pathergy test of an intradermal injection of 0.1 ml normal saline into a forearm and the develop-
J Korean Radiol Soc 2007;57:141-144
─ 141 ─
Percutaneous Transhepatic Venous Embolization of Pulmonary Artery Aneurysm in Hughes - Stovin Syndrome
1Kyung Ah Kim, M.D., Man Deuk Kim, M.D., Do Yun Oh, M.D.2, Pil Won Park, M.D.2
1Department of Diagnostic Radiology, Bundang CHA General Hospital, Pochon CHA University
2Department of Internal Medicine, Bundang CHA General Hospital, Pochon CHA University
Received March 23, 2007 ; Accepted July 11, 2007
Address reprint requests to : Man Deuk Kim, M.D., Department of Diagnostic Radiology Bundang CHA General Hospital, Pochon CHA University, 351 Yatap-dong, Bundang-gu, Sungnam-si, Kyonggi-do 463- 712, Republic of Korea.
Tel. 82-31-780-5382 Fax. 82-31-780-5381 E-mail: [email protected]
Hughes-Stovin syndrome is an extremely rare entity. We present a case of a 42-year- old man, who developed deep vein and inferior vena cava (IVC) thrombosis, repeated internal bleeding and pulmonary artery aneurysms (PAAs). The patient presented with massive hemoptysis and with PAAs of a 2.5 cm maximum diameter. We describe the successful percutaneous transhepatic venous embolization of the PAAs due to occlud- ed common vascular pathways to the pulmonary artery.
Index words :Pulmonary artery Embolization Aneurysm
Computed tomography (CT) Cardiovascular
ment of a skin eruption (papule, nodule, pustule) was al- so negative.
Computed tomography (CT) of the abdomen revealed a hematoma and active bleeding in anterior pararenal space around the duodenal second portion with a focal, localized eccentric thrombosis of the inferior vena cava (IVC) at the level of renal vein confluence. Arteriogra- phy demonstrated multiple microaneurysms at the transverse pancreatic artery and the pancreaticoduode- nal artery; they were embolized with three 6-mm Tornado platinum microcoils (Cook, Bloomington, IN U.S.A.).
The patient had to stop anticoagulation therapy due to bleeding, and a Gu¨nther Tulip IVC filter (Cook) was temporarily placed via the right internal jugular vein.
Recovery was uneventful, and the patient was dis- charged in good condition after two weeks with antico- agulation therapy, again with warfarin for IVC thrombo- sis and the IVC filter was retrieved via the right internal jugular vein. However, after another 4 weeks, the pa- tient was readmitted to a local hospital because of mas- sive hemoptysis. When the patient was referred to our hospital, a contrast-enhanced CT scan revealed well de- marcated, two ovoid shaped vascular masses on the right lower lobe compatible with PAAs (maximum di- ameter 1.5 cm and 2.5 cm, respectively). The diagnosis of Hughes-Stovin syndrome was made only after finding the PAAs. The IVC was completely occluded and suprarenal placement of a Gu¨nther Tulip IVC filter (Cook) was performed. The left internal jugular vein was used for placement of the IVC filter since the right internal jugular vein was occluded. The only medical treatment of immunosuppressive therapy was done without considering an interventional procedure since the patient had been stable when referred and had re- fused to undergo an intervention.
On a follow-up chest CT scan 4 months later, one of two PAAs in the superior segment of the right lower lobe had spontaneously regressed. The second aneurysm in the posterior basal segment of the right lower lobe decreased in size, and was partially throm- bosed. The patient was readmitted with pain in the left inguinal and left lower quadrant 4 months later. CT re- vealed a hematoma of the left psoas muscle area and contrast extravasation. Arteriography revealed an aneurysm of the third left lumbar artery, and endovas- cular embolization with glue was performed successful- ly.
Three months later, the patient returned to the hospi-
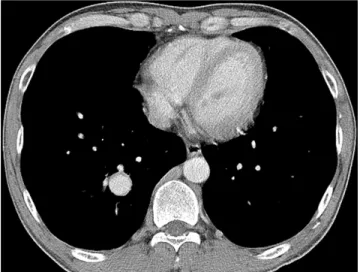
tal for blood-tinged sputum during coughing. A chest CT revealed that the PAA in the right lower lobe had in- creased in size measuring 2.5 × 2.0 cm (Fig. 1). Due to the risk of aneurysm rupture and massive hemoptysis, embolization of the PAA was planned, but the common venous access routes (jugular, subclavian, IVC) were to- tally occluded.
Therefore, the right hepatic vein via a percutaneous transhepatic venous approach was chosen for venous access. Fluoroscopic-guided puncture of the right hepat- ic vein was performed (Fig. 2A) by use of a NEFF percu- taneous access set (Cook). Right pulmonary arteriogra- phy demonstrated a PAA present on the right lower lobe (Fig. 2B). A 90 cm, 7-French introducer catheter (Vistabritetip, Cordis, Miami, FL U.S.A.) was advanced into the right posteromedial branch of the pulmonary artery, and the feeding artery was then subselected with use of the inner 5-French catheter (DAV, Cook,) with the coaxial system. Embolization of the feeding artery and the aneurysmal sac was then performed using twelve platinum coils (12 mm× 14 cm, Nester, Cook) until there was complete cessation of blood flow through the aneurysm (Fig. 2C). Withdrawing the guid- ing catheter, gelfoam embolization was performed to prevent tract bleeding. The patient had no respiratory symptoms after the procedure and the blood oxygena- tion level was within the normal range.
Post-procedural recovery was uneventful, and the pa- tient was discharged 7 days after embolization. No more blood-tinged sputum was reported and a follow-up chest plain film shows no evidence of recurrence of a pul- monary aneurysm in 16 months.
Kyung Ah Kim, et al: Percutaneous Transhepatic Venous Embolization of Pulmonary Artery Aneurysm in Hughes - Stovin Syndrome
─ 142 ─
Fig. 1. A chest CT scan reveals a pulmonary artery aneurysm has increased in size measuring 2.5 cm in the maximum diam- eter on the right lower lobe.
Discussion
Hughes and Stovin first described a syndrome consist- ing of multiple pulmonary aneurysms and peripheral venous thrombosis in 1959 (1). Patients can show di- verse symptoms from mild symptoms such as cough, dyspnea, headache and intermittent fever to severe symptom such as papilledema or massive hemoptysis (3, 4). The etiology is still unknown. Hughes and Stovin postulated that a congenital defect of the bronchial arter- ial wall results in inadequate nutrition to pulmonary ar- teries (1, 4, 5). In the setting of pulmonary embolic dis- ease, inflammation and vessel wall destruction occurs and aneurysms are formed. Another theory is that in-
fected emboli with organisms of low-grade virulence will cause mycotic aneurysms (1, 4, 5).
Hughes-Stovin Syndrome can be diagnosed in the case of PAAs combined with deep vein thrombosis without evidence of Behcet’s disease.
Until now, fewer than 30 cases have been published in the English language literature.
Several cases revealed that massive hemoptysis due to rupture of a PAA was the predisposing condition fol- lowed by death (6, 7).
In Hughes-Stovin syndrome, the pulmonary artery is usually involved with hemoptysis but there has been a report of hemoptysis caused by rupture of a bronchial artery aneurysm (8). In another case, deep vein throm- bosis and combined left hepatic artery aneurysms were
J Korean Radiol Soc 2007;57:141-144
─ 143 ─
A B
C
Fig. 2. A. Percutaneous transhepatic venousvenous ac- cess was attempted. An IVC filter is demonstrated on the suprarenal portion for IVC thrombosis.
B. A pulmonary artery angiogram reveals a 2.5 cm sized pulmonary artery aneurysm on the right lower lobe.
C. Angiography shows complete exclusion of the pul- monary artery aneurysm following embolization with twelve Nester coils.
reported (5).
This case showed pancreaticoduodenal and lumbar artery aneurysms that were ruptured as well as PAAs with progrssive deep vein and IVC thrombosis. The fre- quency of pulmonary involvement by Behcet’s disease is about 1-8% (9). When a pulmonary artery aneurysm is revealed, usually Bechet’s disease is suspected.
Nevertheless, if clinical symptoms such as a skin lesion or genital ulcer are not consistent with Behcet’s disease, the next step is to consider Hughes-Stovin syndrome.
The use of a pathergy test that has been accepted as one of the major criteria in Behcet’s disease shows a nega- tive finding for Hughes-Stovin syndrome.
Treatment for the PAAs is mainly the use of immuno- suppressive agents such as steroids, cyclophosphamide or azathioprine. Acican et al. (10) reported complete re- gression of a pulmonary aneurysm when azathioprine- steroid combination therapy was used in a patient with Bechet’s disease. This case also demonstrated that med- ical treatment could induce regression of a PAA though the partially regressed PAA later increased in size. If rapid resolution of a pulmonary aneurysm causing clini- cal symptoms is required, endovascular embolization or surgery can be considered.
Lobectomy is major method for surgical treatment of a pulmonary aneurysm. However, a lobectomy has signif- icant limitations. Pulmonary involvement in Hughes- Stovin syndrome shows a tendency of multiple pul- monary aneurysms in a few lobes, and close follow-up should be mandatory. Endovascular embolization with coils or other embolic agents is the ideal method for PAA treatment. This method can lead to rapid occlusion of an aneurysm and the procedures can be performed several times. The general condition of a patient will
more quickly recover than for surgery. However, a thrombosis in central veins can impede catheter pas- sage. To the best of our knowledge, this is the first re- port of the use of transhepatic venous embolization of PAA in Hughes-Stovin Syndrome.
We conclude that the percutaneous transhepatic ve- nous approach is a good alternative access route to treat PAAs in patients whose normal pathways are occluded due to a venous thrombosis.
References
1. Hughes JP, Stovin PG. Segmental pulmonary artery aneurysm with peripheral venous thrombosis. Br J Dis Chest 1959;53:19-27 2. Ammann ME, Karnel F, Olbert F, Mayer K. Radiologic findings in
the diagnosis of Hughes-Stovin syndrome. AJR Am J Roentgenol 1991;157:1353-1354
3. Weintraub JL, DeMayo R, Haskal ZJ, Susman J. SCVIR annual meeting film panel session: diagnosis and discussion of case 1:
Hughes-Stovin syndrome. J Vasc Interv Radiol 2001;12:531-534 4. Fischer A, Korman DS, West SG. Radiologic vignette: Hughes-
Stovin syndrome. Arthritis Rheum 2005;53:114-116
5. Mahlo HR, Elsner K, Rieber A, Brambs HJ. New approach in the diagnosis of and therapy for Hughes-Stovin syndrome. AJR Am J Roentgenol 1996;167:817-818
6. Kopp Wl, Green Ra. Pulmonary artery aneurysms with recurrent thrombophlebitis. The “Hughes-Stovin syndrome”. Ann Intern Med 1962;56:105-114
7. Durieux P, Bletry O, Huchon G, Wechsler B, Chretien J, Godeau P. Multiple pulmonary arterial aneurysms in Behcet’s disease and Hughes-Stovin syndrome. Am J Med 1981;71:736-741
8. Herb S, Hetzel M, Hetzel J, Friedrich J, Weber J. An unusual case of Hughes-Stovin syndrome. Eur Respir J 1998; 11:1191-1193 9. Hiller N, Lieberman S, Chajek-Shaul T, Bar-Ziv J, Shaham D.
Thoracic manifestations of Behcet disease at CT. Radiographics 2004;24:801-808
10. Acican T, Gurkan OU. Azathiopine-steroid combination therapy for pulmonary arterial aneurysms in Behcet’s disease. Rheumatol Int 2001;20:171-174
Kyung Ah Kim, et al: Percutaneous Transhepatic Venous Embolization of Pulmonary Artery Aneurysm in Hughes - Stovin Syndrome
─ 144 ─
대한영상의학회지 2007;57:141-144
Hughes-Stovin Syndrome 환자에서 경피경간정맥 폐동맥류의 색전: 증례 보고1
1포천중문 의과대학 분당차병원 영상의학과
김경아・김만득・오도연2・박필원2
Hughes-Stovin syndrome은 매우 드문 질환으로 심부 정맥 혈전과 폐동맥류를 동반한다. 저자들은 객혈을 동반 한 Hughes-Stovin syndrome으로 진단 받은 42세 남자 환자에서 심부 정맥혈전으로 인해 일반적인 방법으로는 폐동맥 접근이 어려워 경피경간 색전술로 치료한 1예를 경험 하였기에 이를 문헌 고찰과 함께 보고하고자 한다.