Korean J Gastroenterol Vol. 76 No. 6, 327-330 https://doi.org/10.4166/kjg.2020.126 pISSN 1598-9992 eISSN 2233-6869
CASE REPORT
Korean J Gastroenterol, Vol. 76 No. 6, December 2020 www.kjg.or.kr
방사선 치료로 치유된 대장 Mucosa-associated Lymphoid Tissue 림프종: 증례보고 및 문헌고찰
이면재, 명은, 오형훈, 주영은
전남대학교 의과대학 내과학교실
Colonic Mucosa-associated Lymphoid Tissue Lymphoma Treated by Radiation Therapy:
Report of a Case and Literature Review
Myeon-Jae Lee, Eun Myung, Hyung-Hoon Oh and Young-Eun Joo
Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea
Mucosa-associated lymphoid tissue (MALT) lymphoma predominantly involves the gastrointestinal tract, with the stomach being the most commonly affected site. Colonic involvement is quite rare. Hence, the etiology, clinical characteristics, treatment, and outcome of colonic MALT lymphoma are not well established. This paper reports a case of MALT lymphoma of the transverse co- lon, presenting as a subepithelial tumor in a 50-year-old woman. The patient received 3,060 cGy in 17 fractions with external beam radiation therapy for three weeks. At 2 months after radiation therapy, a colonoscopy examination revealed complete reso- lution and a scar change of the lesion. The follow-up at 24 months revealed no evidence of tumor recurrence after radiation therapy. (Korean J Gastroenterol 2020;76:327-330)
Key Words: Mucosa-associated lymphoid tissue lymphoma; Radiotherapy
Received October 7, 2020. Revised November 9, 2020. Accepted November 9, 2020.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2020. Korean Society of Gastroenterology.
교신저자: 주영은, 58128, 화순군 화순읍 서양로 264, 전남대학교 의과대학 내과학교실
Correspondence to: Young-Eun Joo, Department of Internal Medicine, Chonnam National University Medical School, 264 Seoyang-ro, Hwasun-eup, Hwasun 58128, Korea. Tel: +82-62-220-6296, Fax: +82-62-225-8578, E-mail: [email protected], ORCID: https://orcid.org/0000-0003-0422-2439
Financial support: None. Conflict of interest: None.
INTRODUCTION
Mucosa-associated lymphoid tissue (MALT) lymphoma is a distinct subtype of non-Hodgkin lymphomas that occurs in ap- proximately 5% of non-Hodgkin lymphomas. Most MALT lym- phomas are found in the gastrointestinal tract, with the stom- ach being the most common site. On the other hand, colonic MALT lymphoma is a rare disease that comprises only 2.5%
of MALT lymphomas.1-3 Therefore, the etiology, clinical charac- teristics, treatment, and outcomes of colonic MALT lymphoma are not completely understood. The disease was previously treated by single or combination of surgery, endoscopic re-
section, conventional chemotherapy, rituximab, or radiation therapy.1-3 This paper reports a case of a 50-year-old woman with MALT lymphoma arising in the transverse colon that was treated successfully with radiation therapy alone with a review of the relevant literature.
CASE REPORT
A 50-year-old woman visited Chonnam National University Hwasun Hospital with a 2-year history of constipation. She denied any prior medical history or other symptoms, such as fever, weight loss, general weakness, anorexia, abdominal
328 이면재 등. 대장 MALT 림프종의 방사선 치료 1예
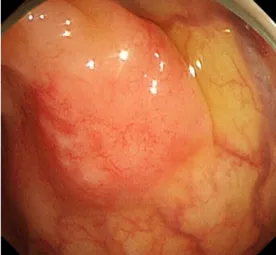
The Korean Journal of Gastroenterology Fig. 1. Colonoscopy shows a 20 mm sized subepithelial tumor with
hyperemic mucosa arising in the transverse colon.
A B
Fig. 2. Microscopic findings. (A) Endoscopic biopsy specimens show a diffuse and dense infiltration of small-sized lymphocytes and a lymphoepithelial lesion in the colonic mucosa (H&E staining, ×400). (B) Immunohistochemical staining shows infiltrative small-sized lymphocytes with positive for B-cell marker CD20 (×400).
pain, hematochezia, and melena. She was afebrile, and her blood pressure and pulse were normal. Her abdomen was soft, not distended, and there was no tenderness. The liver and spleen were not palpable, and there were no palpable superficial lymph nodes. The laboratory examinations re- vealed the following: white blood cell count 5,000/mm3 (normal: 6,000-10,000), hemoglobin 13.0 g/dL (normal:
12-16), platelet count 287,000/mm3 (normal:
130,000-450,000), BUN 10.6 mg/dL (normal: 8-23), crea- tinine 0.6 mg/dL (normal: 0.5-1.3), serum albumin 4.2 g/dL (normal: 3.0-5.0), AST 22 U/L (normal: 5-37), ALT 13 U/L (normal: 5-40), ALP 72 U/L (normal: 39-117), and LDH 376 IU/L (normal: 218-472). The total bilirubin was 0.74 mg/dL with 0.35 mg/dL direct fraction (normal: 0.2-1.2/0.05-0.3).
HBsAg was negative. The anti-HBs was positive, and anti-HCV
was negative. The beta-2-microglobulin level was 1,924 μg/L (normal: 970-2,640).
Contrast-enhanced neck, chest, abdomen, and pelvis CT was performed, and bone marrow aspiration was negative for lymphoma involvement. Esophagogastroduodenoscopy re- vealed chronic gastritis with intestinal metaplasia. The histol- ogy study and CLO test were negative for a Helicobacter pylori (H. pylori) infection. Colonoscopy showed a 20 mm sized sub- epithelial tumor with hyperemic mucosa arising in the trans- verse colon (Fig. 1), and a colonoscopy biopsy was performed.
Routine histology and staining using hematoxylin-eosin re- vealed a diffuse and dense infiltrate of small-sized lympho- cytes and a lymphoepithelial lesion in the colonic mucosa (Fig.
2A). An immunohistochemical examination was performed to clarify the nature of the cells. The tumor cells were positive for CD20 (Fig. 2B) and negative for CD3 and Bcl-6. In addition, the Ki-67 labeling index was 30%. The biopsy specimens were interpreted as MALT lymphoma. The tumor was diagnosed as a MALT lymphoma of the transverse colon and classified as stage IE according to the Ann Arbor staging classification.
Radiation therapy was performed after a discussion with the authors’ multidisciplinary medical team, including a medical oncologist, radiation oncologist, gastroenterologist, and surgeon. Before treatment, the target of radiation therapy was indicated by hemoclips (Fig. 3A) because the lesion was not detected in the abdomen CT scan. The patient received 3,060 cGy in 17 fractions with external beam radiation therapy for 3 weeks. Two months after the radiation therapy was com- plete, a colonoscopy examination revealed complete reso- lution with the endoscopic and histologic disappearance of
Lee MJ, et al. Colonic MALT Lymphoma 329
Vol. 76 No. 6, December 2020
A B
Fig. 3. Colonoscopy findings. (A) The target of radiation therapy is indicated by a hemoclip. (B) After radiation therapy, a follow-up colonoscopy revealed complete resolution and scar change in the lesion.
the lesion and a scar change of the lesion (Fig. 3B). The pa- tient has been on a regular followed-up schedule at the out- patient clinic and has shown no evidence of recurrence at 24 months after radiation therapy.
DISCUSSION
MALT lymphoma is a subtype of non-Hodgkin lymphoma that is classified as an extranodal marginal zone B cell lym- phoma of the MALT type.4 The stomach is the most common site of MALT lymphoma involvement, but colon involvement is very rare.1-4
Colonic MALT lymphoma typically occurs in patients be- tween 50 and 75 years. The gender predisposition ranges from equal to a female predominance. The clinical pre- sentation is often asymptomatic, followed by abdominal dis- comfort and pain, hematochezia, tenesmus, mucoid stool, constipation, or palpable mass. The most common site is the rectum, followed by the right-side colon, sigmoid colon, and transverse colon. The main endoscopic appearance was a sin- gle lesion or multinodular polypoid lesions, followed by a sub- epithelial tumor, flat elevation, mucosal edema, erythema, and loss of vascularity.1-3 The patient in this study was a 50-year-old woman with an asymptomatic MALT lymphoma of the transverse colon, presenting as a subepithelial tumor found incidentally on screening colonoscopy.
Colonic MALT lymphomas are treated with various modal- ities, including single surgery or a combination of surgery with
endoscopic resection, chemotherapy, rituximab alone, or radi- ation therapy. Colonic MALT lymphoma has an indolent nature and favorable clinical behavior. On the other hand, its rarity and indolent nature mean that the treatment and outcome of colonic MALT lymphoma are not well established.
Gastric MALT lymphoma constitutes approximately 70% of MALT lymphomas of the gastrointestinal tract. The disease is associated strongly with a H. pylori infection, and H. pylori eradication is a standardized therapy for localized gastric MALT lymphoma.4-6 Although several reports have shown that colonic MALT lymphomas can be successfully treated with H.
pylori eradication,7-9 the relationship between colonic MALT lymphoma and H. pylori infection is unclear.
Radiation therapy is an effective modality in dealing with MALT lymphomas arising in other organs, and its recurrence is not always in the original area of disease.4 Therefore, early colonic MALT lymphoma may be treated safely by non-surgical management, avoiding the morbidity and mortality that is as- sociated with surgical resections.10 In the present case, the lesion was stage IE and limited to the transverse colon. As MALT lymphoma has an indolent nature and was a localized lesion, definitive treatment with radiation therapy was plan- ned after discussion with the multidisciplinary medical team.
Because the tumor was not detected in the abdomen CT scan, the tumor was marked by hemoclips before radiation therapy.
At 2 months after radiation therapy, the colonoscopy examina- tion revealed complete resolution and scar change of the lesion. Twenty-four months after radiation therapy, the patient
330 이면재 등. 대장 MALT 림프종의 방사선 치료 1예
The Korean Journal of Gastroenterology
showed no tumor recurrence. Previously, limited cases of lo- calized colonic MALT lymphomas were treated successfully with radiation therapy alone ranging from 30 to 45 Gy, but it did not appear to be used widely over the world.2,3,11-13
The present case and previous reports suggest that radia- tion therapy alone may be a feasible and safe treatment, al- lowing for organ preservation, and is considered to treat such a localized colonic MALT lymphoma.10 On the other hand, fur- ther follow-up will be needed to determine the long-term effi- cacy of this treatment approach and its side effects, such as radiation colitis.
REFERENCES
1. Tannoury J, Amiot A, Lemonnier F, et al. Colonic mucosa-asso- ciated lymphoid tissue lymphoma: a case series. Leuk Lymphoma 2020;61:582-587.
2. Won JH, Kim SM, Kim JW, Park JH, Kim JY. Clinical features, treatment and outcomes of colorectal mucosa-associated lym- phoid tissue (MALT) lymphoma: literature reviews published in English between 1993 and 2017. Cancer Manag Res 2019;11:
8577-8587.
3. Jeon MK, So H, Huh J, et al. Endoscopic features and clinical out- comes of colorectal mucosa-associated lymphoid tissue lymphoma. Gastrointest Endosc 2018;87:529-539.
4. Violeta Filip P, Cuciureanu D, Sorina Diaconu L, Maria Vladareanu A, Silvia Pop C. MALT lymphoma: epidemiology, clin- ical diagnosis and treatment. J Med Life 2018;11:187-193.
5. Hatakeyama M. Malignant Helicobacter pylori-associated dis- eases: gastric cancer and MALT lymphoma. Adv Exp Med Biol 2019;1149:135-149.
6. Salar A. Gastric MALT lymphoma and Helicobacter pylori. Med Clin (Barc) 2019;152:65-71.
7. Matsuo S, Mizuta Y, Hayashi T, et al. Mucosa-associated lym- phoid tissue lymphoma of the transverse colon: a case report.
World J Gastroenterol 2006;12:5573-5576.
8. Matsumoto T, Iida M, Shimizu M. Regression of mucosa-asso- ciated lymphoid-tissue lymphoma of rectum after eradication of Helicobacter pylori. Lancet 1997;350:115-116.
9. Raderer M, Pfeffel F, Pohl G, Mannhalter C, Valencak J, Chott A.
Regression of colonic low grade B cell lymphoma of the muco- sa associated lymphoid tissue type after eradication of Helicobacter pylori. Gut 2000;46:133-135.
10. Petrosky JA, Hallac A, Agbroko SO, et al. Management of asymp- tomatic mucosa-associated lymphoid tissue lymphoma of the colon found incidentally on colonoscopy. Clin Gastroenterol Hepatol 2017;15:1130-1132.
11. Foo M, Chao MW, Gibbs P, Guiney M, Jacobs R. Successful treat- ment of mucosa-associated lymphoid tissue lymphoma of the rectum with radiation therapy: report of a case. Dis Colon Rectum 2008;51:1719-1723.
12. Kelley SR. Mucosa-associated lymphoid tissue (MALT) variant of primary rectal lymphoma: a review of the English literature. Int J Colorectal Dis 2017;32:295-304.
13. Piotrowski R, Kramer R, Kamal A. Image of the month. Extranodal marginal zone B-cell (mucosa-associated lymphoid tissue) lym- phoma of the colon presenting as an obstructing mass. Clin Gastroenterol Hepatol 2008;6:e18-e19.