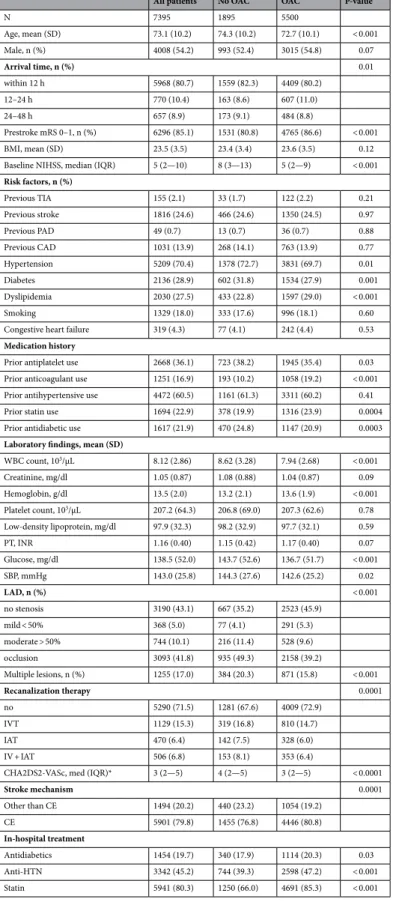
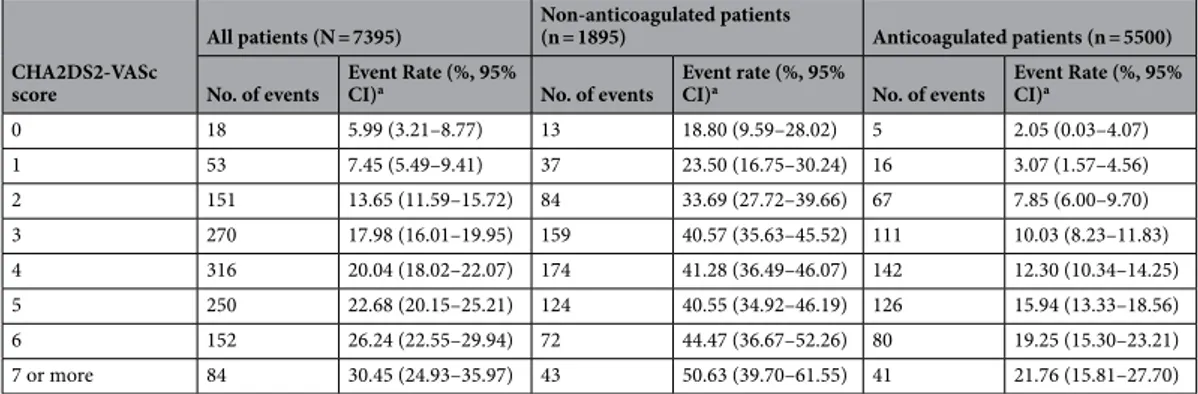
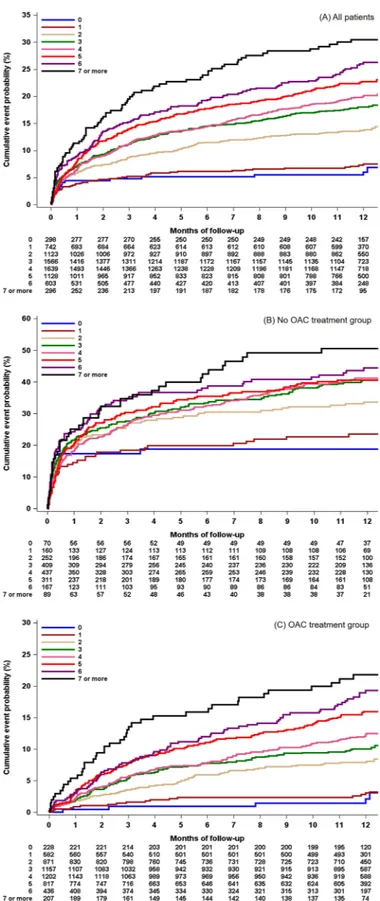
CHA2DS2-VASc score in acute ischemic stroke with atrial fibrillation: results from the Clinical Research Collaboration for Stroke in Korea
10
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
수치
관련 문서
Receiver operating characteristic (ROC) curves for favorable outcome and the baseline diffusion-weighted imaging (DWI) Alberta Stroke Program Early CT Score (ASPECTS) and lesion
We investigated the adherence to guidelines for ther- apy in AF patients hospitalized with acute ischemic stroke (AIS) before stroke onset and at discharge, with the aim of
The findings of this study show that a low baseline eGFR was strongly predictive of both poor functional outcome at 3 months after an acute ischemic stroke and
1,24 In our study, the patients with rhythm control that included cath- eter ablation were younger, had a lower risk of stroke (mean of CHA 2 DS 2 -VASc score 2.8±1.6),
Conclusions—Acute stroke in atrial fibrillation patients is associated with high rates of ischemic recurrence and major bleeding at 90 days. This study has observed that high CHA
Keywords Elderly; Ischemic stroke; Thrombolytic therapy; Outcome assessment.. nine, and hemoglobin); (3) vascular risk factors (hypertension, diabetes
This analysis investigated the incidence and predictors of isch- emic stroke events in patients undergoing successful catheter ablation of typical AFL. By utilizing CHA 2 DS 2
We investi- gated if temporary opening of occluded vessels using a stent retriever before final reperfu- sion might improve clinical outcome in acute ischemic stroke patients
