`
요추전방전위증 환자들에서 후방요추체간유합술로 자가골편 또는 Cage를 사용한 두 군간의 비교 *
한림대학교 의과대학 신경외과학교실
신필재·김창현·문재곤·이호국·황도윤
= Abstract =
Comparision of the Two Groups between Autologous Bone Chips and Cage as Posterior Lumbar Interbody Fusion in Spondylolisthesis Patients*
Pill Jae Shin, M.D., Chang Hyun Kim, M.D., Jae Gon Moon, M.D., Ho Kook Lee, M.D., Do Yun Hwang, M.D.
Department of Neurosurgery, College of Medicine, Hallym University, Seoul, Korea
bjective:Posterior lumbar interbody fusion(PLIF) with transpedicular screw fixation(TPSF) have many merits in the treatment of spondylolisthesis. The aim of this study was to compare cage PLIF group(PLIF using cage and TPSF) with chip PLIF group(PLIF using autologous bone chips and TPSF) as surgical treatment of spondylo- isthesis.
Methods:PLIF and TPSF were performed in 44 patients with spondylolisthesis from January 1994 to December 1998. The surgical methods were divided into two groups. One group was cage PLIF(20 patients), and the other group was chip PLIF(24 patients). We analyzed the change of anterior translation, change of intervertebral space height, fusion rate, clinical outcomes, and postoperative complications in two groups.
Result:There was no significant difference in reduction and maintenance of anterior translation between two groups. Intervertebral space height was increased in the two groups at immediate postoperative state. At last follow- up, it was decreased compared to preoperative height in chip PLIF group. In cage PLIF group, last follow-up height was decreased compared to immedate postoperative height, but it was significantly increased compared to preoperative height. Fusion rates were 70.9% and 90% in chip PLIF group and cage PLIF group, respectively. Exce- llent and good clinical outcomes were 79.2% in chip PLIF group and 85% in cage PLIF group, but there was no statistical significance. Complications were screw fracture(1 case), CSF leakage(1 case) in chip PLIF group and screw loosening and retropulsion of cage(1 case), CSF leakage(2 cases) in cage PLIF group.
Conclusion:PLIF using cage is better than PLIF using autologous bone chips in the maintenance of intervertebral space height and fusion rate. But there is no statistical difference of the clinical outcomes between the two groups.
Further studies, especially on long term follow-up, should be considered.
KEY WORDS:Posterior lumbar interbody fusion・Autologous bone chips・Cage・Spondylolisthesis.
서 론
요추전방전위증의 수술 방법 중 추경 나사못을 이용한 내
고정술과 후방요추체간유합술이 많은 장점을 가지고 있어 현재 보편적으로 사용되고 있는 방법이다
3)8)9)18)25). 후방요 추체간유합술 중 자가골편(autologous bone chips)만을 사 용하는 방법과 cage를 사용하는 방법은 각각의 장단점을 가지고 있다
20)21).
이에 저자들은 1994년 1월부터 1998년 12월까지 본원
OOOO
*본 논문은 4년차 전문의 응시용임.
신경외과에서 요추전방전위증으로 추경 나사못고정 후 후방 요추체간유합술을 시행한 환자들 중, 자가골편만을 이용한 환자들과 cage를 이용한 환자들 총 44례를 대상으로 전방 전위 변화, 추간강(intervertebral space) 높이 변화, 골유 합률, 임상 결과, 합병증 등을 비교 분석하여 요추전방전위 증의 수술적 치료에 있어 두 방법간의 우월성을 알아보고자 한다.
대상 및 방법
1. 대 상
1994년 1월부터 1998년 12월까지 본원 신경외과에서 요추전방전위증으로 진단된 환자들 중 추경 나사못고정 후 후방요추체간유합술로 자가골편을 이용한 군(24례, 이하 chip PLIF군)과 cage를 사용한 군(20례, 이하 cage PLIF군)을 대상으로 하였다.
총 44례중 여자가 31례, 남자가 13례로 여자가 많았다.
연령 분포는 35세부터 71세까지로서 평균 51세였으며, 50 대에서 24례로 가장 많았다.
2. 방 법
1) 방사선학적 소견 및 임상 결과 평가
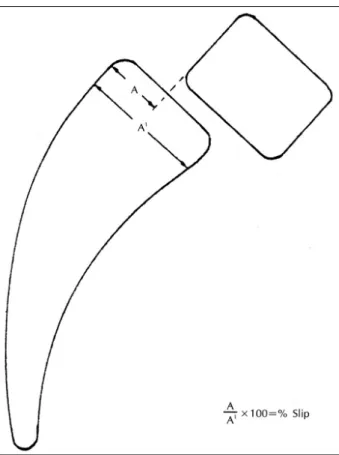
전방전위 정도의 측정은 Taillard의 방법
11)23)대로 중립에 서 측면상을 촬영하여 전위된 정도를 백분율로 나타내었다 (Fig. 1). 추간강 높이는 전방전위된 추체 하면의 중간 부위 에서 하부 추체의 상면과 수직으로 만나는 길이를 mm로 나타내었다. 전방전위 정도와 추간강 높이 모두 수술 전, 수 술 직후, 마지막 방문시의 정도를 비교 관찰하였다. 골유합 의 정도는 Brantigan과 Steffee의 분류
3)에 근거하였으며 (Table 1). 임상 결과의 평가는 변형된 Gill’s criteria
10)를 사용하였다(Table 2). 추적 관찰 기간은 4개월부터 56개월 까지 평균 7.4개월이었다.
2) 수술 방법
협부결손형은 Gill씨 술식
10)에 따라 불안전한 후궁을 하 관절을 포함하여 제거하였다. 협부결손부위의 육아조직을 완전히 제거하여 상부신경근이 나가는 신경공을 감압하고 하부신경근이 나가는 신경공의 협착이 있을 경우에도 신경 공 감압을 시행하였다. 퇴행형은 후궁 완전절제술, 척추관절 내측부분절제술을 시행하여 신경조직의 충분한 감압을 시도하 였다. 감압술 후 추경 위치에 유도핀을 삽입한 후 단순 측면 방사선 촬영으로 그 위치를 확인하고 적절한 내방각(medial angulation)을 주어 추경 나사못을 삽입하였다. 수핵 및 연 골성 골단판을 추체 전방까지 완전히 제거하고 피질성 골단 판을 노출시켰다. 총 44례 중 24례에서 후궁 제거시 얻어 진 골편을 2~4mm 크기의 피질・해면골 조각(cortico-
Table 1. Description of fusion result*
Grade 1 Obvious radiographic pseudoarthrosis 2 Probable radiographic pseudoarthrosis 3 Radiographic status uncertain
4 Probable radiographic fusion 5 Radiographic fusion
*:according to Brantigan JW and Steffee AD
3)Table 2. Criteria for assessment of clinical outcomes*
Criteria Contents Excellent Able to carry out all activities, no back or lower
extremity pain
Good Able to carry out all activities, mild or occasional back or lower extremity pain
Fair
Improved over preoperative status, mild or occasional back or lower extremity pain, some restriction of activity
Poor
Restriction of activity, moderate to severe back or lower extremity pain, reoperation for any reason
*:modified from Gill’s criteria
10)Fig. 1. The extent of anterior translation, or slip, is expressed
as a percentage obtained by dividing A by A1 and
multiplying by 100.
cancellous piece)으로 잘라 추간강에 조밀하게 채워 넣고, 골임팩터로 강하게 압축 시켰다. 나머지 20례에서는 후궁 제 거시 얻은 골편으로 채워진 cage를 이용하여 추간강을 충분 히 벌린 상태에서 후방요추체간유합술을 시행하였다. 이후 삽입된 추경 나사못에 plate나 rod를 사용하여 단단히 고정 하였다. 수술에 사용한 기구는 screwplate system인 St- ryker, screw-rod system인 Diapason이었으며, Stryker 는 단지 2례에서만 사용되었다. Cage는 CH cage 및 Ogi- val interbody cage(OIC)를 사용하였다.
수술 시간은 chip PLIF군의 경우 평균 248±42분, cage PLIF군은 260±37분으로 큰 차이는 없었다. 실혈량 또한 각각 평균 908±335ml, 893±269ml로 주목할 만한 차이 가 없었다. 환자가 특별히 불편해 하지 않는 한 수술 후 4
~7일부터 환자에게 보조기를 착용시키고 조기 보행을 권 하였다. 보조기는 약 3개월간 착용하도록 하였다.
3) 통계 처리
SAS 프로그램의 Duncan’s multiple range test를 이용 하였다.
결 과
1. 방사선학적 소견
전방전위는 두 군에서 모두 수술 전에 비해 수술 직후 유 의하게 전위가 줄었고, 추적 관찰에서는 수술 직후보다 전위 가 다시 증가했으나 수술 전보다는 감소된 상태를 유지하였 다. 그러나 이는 통계학적으로 유의한 수준은 아니었다(Ta- ble 3).
추간강 높이는 chip PLIF군에서 수술 직후 유의하게 증 가하였으나, 추적 관찰에서는 수술 직후에 비하여 유의하게 감소하여 수술 전보다도 높이가 감소하였다. Cage PLIF군 에서는 수술 직후 높이가 유의하게 증가하였으며, 추적 관 찰에서는 수술 직후에 비해 유의하게 감소하였으나 수술 전 에 비하여 유의하게 증가된 상태를 유지하였다(Table 4).
Grade 4, 5를 골유합된 상태로 볼 경우 chip PLIF군에서 는 70.9%, cage PLIF군에서는 90%로 cage PLIF군에서 더 높은 골유합률을 보였다(Table 5).
2. 임상 결과
Chip PLIF군과 cage PLIF군에서 Excellent와 Good의 좋은 결과를 보인 경우는 각각 79.2%, 85%로 cage PLIF 군에서 좀 더 나은 결과를 보였으나 유의성은 없었다(Ta- ble 6). Poor는 cage PLIF군의 1례에서 있었으며 추경 나 사못 이완 및 cage가 후방돌출된 환자였다(Fig. 2).
3. 합병증
수술 후 발생한 합병증은 chip PLIF군에서 추경 나사못 골 절 1례(Fig. 3)와 뇌척수액 유출 1례가 있었고, cage PLIF군 에서는 추경 나사못 이완 및 cage의 후방돌출 1례, 뇌척수 액 유출이 2례 있었다.
고 찰
요추전방전위증은 보존적 치료에 효과가 없는 지속적 동 통, 전방전위의 점진적 증가, 척수강 협착증 및 지속적인 신 경압박증상이 있는 경우 수술의 적응증이 되며 이는 10~
15%에 이른다
11)14). 수술은 충분한 신경근의 감압과 골유 합 및 내고정기구를 통한 척추의 안정성 획득에 목적이 있 다. 많은 종류의 내고정기구가 개발되었고 내고정기구의 사 용으로 골유합률이 증가되었다
7)8)13)16)25).
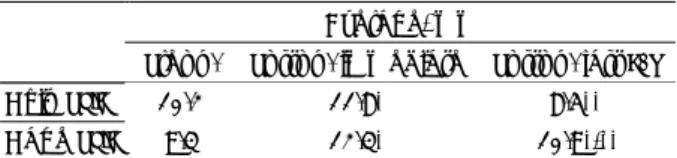
Table 3. Change of percent-slip Average, %
Preop. Postop. immediate Postop. last F/U
Chip PLIF 13.0 5.4* 9.3
Cage PLIF 12.3 7.1* 9.4
*:statistical significant to preop. (p<0.05) Table 4. Change of intervertebral space height
Average, mm
Preop. Postop. immediate Postop. last F/U
Chip PLIF 10.2 11.8* 8.5**
Cage PLIF 9.3 12.3* 10.9*,**
*:statistical significant to preop. (p<0.05)
**:statistical significant to postop. immediate. (p<0.05) Table 5. Rate of interbody fusion
No. of patients(%) Grade
Chip PLIF Cage PLIF 1 2( 8.3%) 1( 5.0%)
2 2( 8.3%) 0
3 3(12.5%) 1( 5.0%) 4 11(45.9%) 3(15.0%)
5 6(25.0%) 15(75.0%)
Total(%) 24(100%) 20(100%)
Table 6. Assessment of surgical outcomes No. of patients(%) Chip PLIF Cage PLIF Excellent 4(16.7%) 6(30.0%) Good 15(62.5%) 11(55.0%) Fair 5(20.8%) 2(10.0%)
Poor 0 1( 5.0%)
Total(%) 24(100%) 20(100%)
Fig. 2. Lateral plain X-ray films obtained in a 58-year-old man with isthmic spondylolisthesis at L5-S1 level.
A: Preoperative film showing anterior translation and decreased intervertebral space. B:Immedi- ate postoperative film demonstrating reduced an- terior translation and increased intervertebral space.
C:Postoperative 3months follow-up film revealing aggravated anterior translation and retropulsion of the cage.
A A A
A B B B B
C
C C
C
Fig. 3. Lateral plain X-ray films obtained in a 57-year-old woman with isthmic spondylolisthesis at L4–5 level.
A: Preoperative film showing anterior translation and collapsed intervertebral space. B:Immediate postoperative film showing reduced anterior tran- slation and distracted intervertebral space. C : Postoperative 56months follow-up film demonstra- ting recollapsed intervertebral space and screw fracture.
A A A
A B B B B
C
C
C
C
추경 나사못은 척추의 전・중・후주(anterior・middle・
posterior column)을 통하여 삽입되어 견고한 고정을 가능 하게 하고, 척추에 신연, 압축, 회전의 힘을 가할 수 있으며, 단일 분절에 사용될 수 있어 정상 분절의 운동을 보존할 수 있다. 또한, 추궁 절제 상태에서도 사용할 수 있어 현재 가 장 많이 사용되고 있는 내고정기구이다
8)9)18)25). 하지만 수 술 방법이 어렵고, 잘못 삽입되어 신경근 손상이 초래될 수 있으며, 추체나 추경 부위가 정상적으로 유지되어 있어야 하고, 심한 골다공증에서 기구 실패의 위험성이 크다는 단 점이 있다
8)25).
Cloward
5)6)가 요추 추간판으로 인한 요통의 치료에 후방 요추체간유합술을 도입한 이후 다양한 수술 방법이 시도되 었다. 후방요추체간유합술은 전주에 가해지는 하중을 감소 시켜 추경 나사못의 골절이나 이완을 방지하며, 궁극적으로 골유합률을 증가시킨다
3)9). 또한 추간강 높이를 증가시켜 신경공의 감압 효과도 있다. Yashiro 등
24)은 후방요추체간 유합술이 후측방유합술보다 전위정복 및 유지, 척추후만증 의 교정에 더 우수한 결과를 얻었다고 보고하였다.
Tullberg 등
21)은 65분절에서 carbon cage를 이용한 후 방요추체간유합술을 시행하여 89%의 골유합률을 얻었고 1례 를 제외한 모든 경우에서 추간강 높이를 유지하였으며, cage 는 능(ridge)과 지주(strut)가 있어 cage의 후방돌출 및 추 간강 높이의 감소 등을 예방할 수 있는 장점이 있다고 하였 다. 본 연구에서도 추간강 높이의 유지에는 cage PLIF군이 훨씬 유리하였는데, 이는 저자들이 사용한 CH cage 및 OIC 도 같은 장점이 있었기 때문이다. 또한 후궁 제거시 얻어진 자가골편을 cage에 사용함으로써 골조직 채취에 따른 합병 증을 예방할 수 있었다.
Niu 등
18)은 골유합률이 높을수록 전위정복의 유지가 잘된다 고 하였다. 본 연구에서는 cage PLIF군이 높은 골유합률을 나 타냈지만 전위정복의 유지에는 두군사이에 통계학적인 차이가 없었다. 하지만 수술 전에 비해 추적 관찰시 전방전위가 더 심 해진 경우가 chip PLIF군이 4례(16.6%), cage PLIF군이 1 례(5%)인 것을 고려해보면 장기간 추적 관찰시 cage PLIF군 이 전위정복의 유지에 더 우수하리라 생각된다.
본 연구의 cage PLIF군에서 90%의 높은 골유합률을 보 인 이유는 Enker 등
9)이 보고한대로 cage에 의한 요추체간 유합술시 추간강 높이의 유지가 잘되어 전주의 지지 역할이 충분하였고, 이로 인하여 추경 나사못에 가해지는 휨모멘트 (bending moment)가 감소하여 골유합 전까지 추경 나사못의 안정성이 유지되었기 때문으로 사료된다. 반면, chip PLIF군 에서는 Simmon
20)의 방법을 이용하여 추간강에 자가골편을 조밀하게 채워 넣고 골임팩터로 강하게 압축시켜 골유합면
을 증가시켰으나, 70.9%의 낮은 골유합률을 보였다. 이는 비교적 단단하지 못한 해면골들이 많아 전주의 지지 역할이 불충분하였기 때문으로 사료된다. 하지만 Chae 등
4)은 골이 식용 깔때기(funnel)와 골임팩터를 사용하여 최소한으로 신 경근을 견인하면서 자가 해면골만을 삽입하여, 91%의 높은 골유합률과 95.3%의 양호한 임상 결과를 얻었다고 보고 하 였다.
합병증으로 감염, 추경 나사못의 이상위치(malposition) 에 의한 신경근 손상, 기구 실패로서 추경 나사못의 이완 및 골절, 이식골 삽입시 신경근의 과다한 견인에 의한 신경근 손상 및 경막외 섬유화, 삽입골의 후방돌출, 뇌척수액 유출 등이 있다
1)12)15)17)19)22). 저자들의 경우 chip PLIF군이 cage PLIF군 보다 자가골편의 추간강내 삽입이 용이하여 신경근 견인이 적었을 것으로 생각되며, 적당한 지름과 길 이를 가진 추경 나사못의 선택과 세심한 수술 수기로써 기구 실패는 어느 정도 감소될 수 있었다. 하지만 추경 나사못은 골 유합이 이루어질 때까지 일시적인 내고정기구이므로
2)8)충분 한 골유합이 일어나기 전까지 보조기를 착용하고 무리한 활 동은 삼가는 것이 필요할 것으로 생각된다. 본 연구의 cage PLIF군에서 수술 3개월후 발생한 추경 나사못의 이완 및 cage의 후방돌출 1례는 환자의 술후 무리한 조기 활동이 원인이었으며, 재수술을 시행하였다. Chip PLIF군에서 발생 한 추경 나사못 골절 1례는 증상이 심하지 않아 추적 관찰 중이다. 뇌척수액 유출 3례는 모두 보존적으로 치료되었다.
이상의 결과들을 고려 해볼때 cage를 이용한 후방요추체 간유합술이 추간강 높이 유지와 골유합률에서 자가골편보다 효과적이나, 임상 결과에 대하여는 장기간의 추적 관찰이 필요하리라 생각된다.
결 론
전방전위의 정복과 유지에 있어서는 두군사이에 유의적인 차이가 없었으나 추간강 높이의 유지에는 cage를 이용한 군 이 더 우월하였다. 또한 골유합률도 cage를 이용한 군에서 현저히 우수하게 나타났다.
임상 결과가 cage를 이용한 군에서 좀 더 나았지만 통계 적으로 유의하지 않아, 향후 더 많은 임상예를 가지고 충분 한 기간의 추적 관찰이 필요하리라 사료된다.
•
논문접수일:1999년 7월 28일•
심사완료일:1999년 9월 27일•
책임저자:김 창 현150-071 서울 영등포구 대림 1동 한림대학교 의과대학 신경외과학교실
전화:02) 829-5175, 전송:02) 833-0219 E-mail:[email protected]
References
1) Ahn SY, Yu DJ, Song JK, et al:Surgical management of
patients with isthmic spondylolisthesis with transpedicular screw fixation and posterior lumbar interbody fusion using posterior movable segment. J Korean Neurosurg 25
:2250- 2257, 1996
2) Bae JK, Kwon CY, Eun JP, et al:Results of transpedicular
screw fixation in spondylolisthesis of the lumbar spine. J Ko- rean Neurosurg 26
:928-933, 1997
3) Brantigan JW, Steffee AD:A carbon fiber implant to aid
interbody lumbar fusion
;Two-year clinical results in the first 26 patients. Spine 18
:2106-2117, 1993
4) Chae IJ, Suh SW, Jung JH:A clinical study of the modified
posterior lumbar interbody fusion using cancellous chip graft.
J of Korean Spine Surg 5
:86-93, 1998
5) Cloward RB:Posterior lumbar interbody fusion updated.
Clin Orthop
(193
):16-19, 1985
6) Cloward RB:The treatment of ruptured lumbar interverte-
bral discs by vertebral body fusion. Indications, operative te- chnique, after care. J Neurosurg 10
:154-168, 1953
7) Davne SH, Myers DL:Complications of lumbar spinal fu-sion with transpedicular instrumentation. Spine 17
:S184- S189, 1992
8) Dickman CA, Fessler RG, Macmillan M, et al:Transpedi-
cular screw-rod fixation of the lumbar spine
;Operative technique and outcome in 104 cases. J Neurosurg 77
:860- 870, 1992
9) Enker P, Steffee AD:Interbody fusion and instrumentation.
Clin Orthop
(300
):90-101, 1994
10) Gill GG, Manning JG, White HL:Surgical treatment of
spondylolisthesis without spine fusion. Excision of the loose lamina with decompression of the nerve roots. J Bone and Joint Surg 37A
:493-520, 1955
11) Grobler LJ, Wiltse LL:Classification, and non-operative
and operative treatment of spondylolisthesis. in Frymoyer JW.
The adult spine, 2nd ed. Lippincott-Raven, 1997, pp1865-1921
12) Hadjipavlou A, Enker P, Dupuis P, et al:The causes of fai-
lure of lumbar transpedicular spinal instrumentation and fusion
;A prospective study. International Orthop 20
:35-42, 1996
13) Hanley EN Jr:The indication for lumbar spinal fusion with
and without instrumentation. Spine 20
:S143-S153, 1995
14) Lee YK, Cho YD, Cho J, et al:Clinical analysis of 54 caseswith spondylolisthesis. J Korean Neurosurg 27
:1109-1116, 1998
15) Lin PM:Posterior lumbar interbody fusion technique;
Com- plications and pitfalls. Clin Orthop
(193
):90-102, 1985
16) Lorenz M, Zindrick M, Schwaegler P, et al:A comparison ofsingle level fusions with and without hardware. Spine 16
:S455-S458, 1991
17) Masferrer R, Gomez CH, Karahalios DG, et al:Efficacy of
pedicle screw fixation in the treatment of spinal instability and failed back surgery
;A 5-year review. J Neurosurg 89
:371-377, 1998
18) Niu CC, Chen WJ, Chen LH, et al:Reduction-fixation spinal
system in spondylolisthesis. Am J Orthop 25
:418-424, 1996
19) Simmons JW:Posterior lumbar interbody fusion. in Frymo-yer JW. The adult spine, 2nd ed, Lippincott-Raven, 1997, pp2225-2252
20) Simmons JW:Posterior lumbar interbody fusion with post-
erior elements as chip grafts. Clin Orthop
(193
):85-89, 1985
21) Tullberg T, Brandt B, Rydberg J, et al:Fusion rate after po-sterior lumbar interbody fusion with carbon fiber implant
;1- year follow-up of 51 patients. Eur Spine J 5
:178-182, 1996
22) Wetzel FT, LaRocca H:The failed posterior lumbar inter-body fusion. Spine 16
:839-845, 1991
23) Wiltse LL, Winter RB:Terminology and measurement of
spondylolisthesis. J Bone and Joint Surg 65A
:768-772, 1983
24) Yashiro K, Homma T, Hokari Y, et al:The Steffee variablescrew placement system using different methods of bone gra- fting. Spine 16
:1329-1334, 1991
25) Zindrick MR:The role of transpedicular fixation systems for