대한소화기학회지 2005;45:348-353
서 론
췌장암은 전 세계적으로 증가하는 추세이며 우리나라의,
경우 연2,500명 정도의 환자가 발생한다. 2002년 사망원인 통계에 따르면 췌장암에 의한 사망률은10만 명당 명으로6 전체 암 사망률 중 위이며 이는5 , 10년 전의3.7명보다 증
Correspondence to: Sung Rok Kim, M.D.
Department of Internal Medicine, Inje University College of Medicine 761-1 Sanggye-dong, Nowon-gu, Seoul 139-707, Korea Tel: +82-2-950-1990, Fax: +82-2-950-1954
E-mail: [email protected] 접수: 2004년 8월 28 ,일 승인: 2005년 3월 7일
연락처: 김성록, 139-707, 서울시 노원구 상계동 761-1 인제대 상계백병원 내과
Tel: (02) 950-1990, Fax: (02) 950-1954 E-mail: [email protected]
* 본 논문은2000년도 인제대학교 학술연구비 보조에 의한것임.
진행 췌장암의 젬시타빈 , 5-FU, 시스플라틴 복합화학요법에 관한 상 연구 2
인제대학교 의과대학 상계백병원 내과학교실
최상봉 이활연 유영진 김성록
A Phase II Study of Combination Chemotherapy with Gemcitabine, A Phase II Study of Combination Chemotherapy with Gemcitabine,A Phase II Study of Combination Chemotherapy with Gemcitabine, A Phase II Study of Combination Chemotherapy with Gemcitabine,
5-fluorouracil, and Cisplatin for Advanced Pancreatic Cancer 5-fluorouracil, and Cisplatin for Advanced Pancreatic Cancer 5-fluorouracil, and Cisplatin for Advanced Pancreatic Cancer 5-fluorouracil, and Cisplatin for Advanced Pancreatic Cancer
Sang Bong Choi, Sang Bong Choi,Sang Bong Choi,
Sang Bong Choi, M.D., Hwal Youn Lee,Hwal Youn Lee,Hwal Youn Lee,Hwal Youn Lee, M.D., Young Jin Yuh,Young Jin Yuh,Young Jin Yuh, M.D.,Young Jin Yuh, and Sung Rok Kim,Sung Rok Kim,Sung Rok Kim,Sung Rok Kim, M.D.
Department of Internal Medicine, Inje University Collage of Medicine, Sanggye Paik Hospital, Seoul, Korea
Background/Aims:
Background/Aims:
Background/Aims:
Background/Aims: Gemcitabine has been the standard regimen for advanced pancreatic cancer, but the effect on the response rate and survival is still disappointing, leading to many trials of combination chemotherapy. 5-FU and cisplatin were combined with gemcitabine in this trial, as they are synergistic with gemcitabine and each other as well. This study was aimed to assess the effectiveness and safety of combination chemotherapy with gemcitabine, 5-FU, and cisplatin for advanced pancreatic cancer. Methods:Methods:Methods:Methods: Patients with advanced pancreatic cancer were entered into this study. Gemcitabine at a dose of 800 mg/m2on day 1 and 8, 5-FU 1,000 mg/m2/day from day 1 to 3 for 72 hours, and cisplatin 60 mg/m2 on day 2, 24 hours after the start of gemcitabine were administered every 3 weeks. Results:Results:Results:Results: From December 2001 to January 2004, twenty patients were enrolled in this study. Among 17 of these patients assessable, 3 patients had a partial remission with the response rate of 17.7% (95% confidence interval, 6.2-41.0%). The median time to disease progression was 230 days and median duration of survival was 322 days. Among total of 91 cycles, leukopenia, neutropenia, and thrombocytopenia of grade 3 or 4 occurred in 12 cycles (13.2%), 12 cycles (13.2%), and 23 cycles (24.4%), re- spectively. Grade 3 or 4 mucositis developed at 2 cycles (2.2%), and nausea and vomiting were encountered in 3 cycles (3.3%). Conclusions:Conclusions:Conclusions: Combination chemotherapy with gemcitabine, 5-FU, and cisplatin for advancedConclusions:
pancreatic cancer is active and well-tolerated, warranting a phase III study. (Korean J Gastroenterol 2005;45:(Korean J Gastroenterol 2005;45:(Korean J Gastroenterol 2005;45:(Korean J Gastroenterol 2005;45:
348-353) 348-353) 348-353) 348-353) Key Words:
Key Words:
Key Words:
Key Words: Pancreatic cancer; Gemcitabine; 5-fluorouracil; Cisplatin
최상봉 외 인 진행 췌장암의 젬시타빈3 . , 5-FU,시스플라틴 복합화학요법에 관한 상 연구2 349
가한 것이다.
췌장암은 완치를 위한 치료로 근치 절제술이 유일하나, 불행히도 진단 당시부터 진행된 경우가 많아 근치 절제술이 가능한 경우는 전체 환자의10-15%에 불과하다 또 근치 절. 제술을 받은 후에도 86%의 환자들은 재발한다.1 처음부터 근치 절제술이 불가능하거나 또는 근치 절제술 이후 재발한 환자들의 예후는 매우 불량하여 평균 생존기간이, 3-5개월 정도에 불과하다.1 이런 환자들을 위한 치료로는 항암화학 요법이 유일하다 진행 또는 재발 췌장암의 항암화학요법으. 로는5-fluorouracil (5-FU)이 주로 이용되어 왔으나5-FU의 반응률은 약0-19%정도에 불과하며 생존기간의 연장도 명, 확하지 않아 항암화학요법을 시행 받은 환자의 평균 생존기 간은 5.5개월에 지나지 않는다.2-4
최근에gemcitabine이 개발되어 기존의5-FU를 대체하는 표준화학요법제로 자리 잡고 있다. Gemcitabine은 년 생존1 율이5-FU의2%에 비하여18%로 우수하며 생존기간도, 4.4 개월에서5.7개월로 증가하였다 또 삶의 질도 우수하여 현. 재 표준요법으로 사용되고 있다.5그러나gemcitabine도 단 독으로 사용할 경우 반응률은6.3-12%에 불과하다.3,4Gemci- 이외의 최근에 개발된 다른 약제 중 과
tabine irinotecan
은 각각 의 반응률을 보이나 연구결과가 oxaliplatin 15-20% ,
많지 않고gemcitabine보다 반응률이 더 우수하지 않다.2현 재 표준요법으로 사용되고 있는gemcitabine만으로는 치료 결과가 만족스럽지 않아 다른 효과적인 약제를 병합하여 반 응률을 더 높이고자 하는 시도들이 이루어지고 있다.
은 단일제제로 췌장암에서 약 정도의 반응
Cisplatin 20%
률을 나타내어 췌장암에도 일부 효과가 있다.2 Cisplatin과 의 복합요법이 췌장암의 치료에 상승작용을 하 gemcitabine
며,6-95-FU와gemcitabine,10-145-FU와cisplatin의 복합요법도 췌장암의 치료에 상승작용을 한다.15또 이들 약제의 용량제 한 독성도 서로 달라5-FU는 점막염, gemcitabine은 골수 독 성, cisplatin은 오심과 신독성이 있으므로 그 독성이 중복되 지 않는 장점이 있다.
이에 저자들은gemcitabine과cisplatin, 5-FU은 서로 상승 작용이 있을 것이라 가정하고 복합화학요법의 효과 및 안전 성을 알아보고자 연구를 시행하였다.
대상 및 방법
대상 환자 1.
이번 연구는 인제대학교 상계백병원 내과에 입원한 환자 중 암이 진행되어 근치 절제술이 불가능하거나 수술 후 재, 발한 췌장암 환자를 대상으로 하였다 대상 환자는 이전에. 방사선치료를 받지 않았고 측정 가능한 병변이 있으며, 18
세에서 70세까지의 환자들로 하였고 말초혈액 호중구가, 1,800/mm3이상 혈소판, 100,000/mm3이상이며 혈색소, 9.0 이상 간기능검사에서 가 정상의 배 이하이
g/dL , AST/ALT 3
고 다른 장기의 위중한 기능부전이 없는 경우로 하였다, .
치료방법 2.
Gemcitabine (Gemzar®, Lilly France S.A., Fegersheim, 은
France) 800 mg/m2를 제 일과 일에 각각 정맥 주사하였1 8 으며, 5-flourouracil (5-FU®,중외제약 한국 은, ) 1,000 mg/m2/
를 제 일부터 일까지 지속해서 정맥 주사하였다
day 1 3 .16Cis-
platin (Cisplan®, 동아제약 한국 은, ) 60 mg/m2를 제 일에2 gemcitabine투여하고24시간 이후에 정맥 주사하였다 구토. 를 예방하기 위해 ondansetron, dexamethasone, metoclopra- mide, lorazepam을 함께 투여하였다 이 치료를 주 간격으. 3 로 반복하였고 병변이 진행되는 증거가 발견되면 연구를, 종료하였다.
투여량 조정 3.
치료 당일 측정한 말초혈액 호중구와 혈소판이 각각 1,800/mm3과 100,000/mm3이상인 경우만 화학요법을 시행했 고 치료가 주 이상 연기된 경우 연구대상에서 제외하였다, 3 . 제 일째에 혈중 호중구가8 500-999/mm3이거나 혈소판 수가 50,000-99,000/mm3이면gemcitabine을50%감량하였고 호중, 구가 500/mm3미만이거나 혈소판 수가 50,000/mm3미만이 면 투여하지 않았다.
매회 치료 시 문진을 통하여 비혈액학 독성을 판단하였 다 세계보건기구. (WHO) 기준으로 3도 이상의 신경독성이 나타나면 cisplatin을 중단하고 연구대상에서 제외하였다. 기준으로 도 이상의 구내염이나 설사가 발생하면
WHO 3
를 감량하였고 감량했는데도 다음 치료 때 도
5-FU 25% , 3
이상의 구내염이나 설사가 발생하면 연구대상에서 제외하 였다 신기능에 따라. cisplatin의 용량을 조절하였으며 신 청, 소율이30-49 mL/min이면cisplatin을50%감량하였고, 30
미만이면 투여하지 않았다
mL/min .
치료 효과 분석 4.
매회 치료 전에 병력 청취 신체검사 말초혈액검사 간기능, , , 검사 신기능검사 단순흉부 촬영을 시행하고 치료의 독성을, , 평가하였다 치료 후 진행 증거가 없으면 다시 회의 치료를. , 2 더 시행한 후 복부 전산화단층촬영으로 효과를 분석하였다.
치료 효과는 WHO의 기준에 따라 완전관해는 모든 측정 가능한 병변이 최소 주 이상 완전히 없어진 경우 부분관4 , 해는 모든 측정 가능한 병변의 지름의 합이 50%이상 주4 이상 감소한 경우 불변은 병변이, 50% 미만 감소하였거나 미만 증가한 경우 진행은 병변이 이상 진행하였
25% , 25%
350 The Korean Journal of Gastroenterology: Vol. 45, No. 5, 2005
거나 새로운 병변이 발생한 경우로 정의하였다.
진행 기간은 치료 시작일에서 병변의 진행이 확인된 날까 지로 생존기간은 치료 시작일에서 사망일로 정의하였다, . 생존기간은SPSS (version 10.0)를 이용하여Kaplan-Meier방 법으로 분석하였다.
결 과
대상 환자의 특성 1.
년 월부터 년 월까지 모두 예가 연구에 포 2001 12 2004 1 20
함되었다 대상 환자의 연령은. 40-69 (세 평균60.3 )세 였고 남, 성이14 ,예 여성이 예였다 활동도는6 . Eastern Cooperative 기준으로 도 또는 도가 예였 Oncology Group (ECOG) 0 1 16 고, 2도가 예2 , 3도가 예였다2 . 15예는 기존 항암요법의 병 력이 없었으나, 5예는 이전에 다른 항암요법을 받았으며 치 료 중단 후 평균44일 뒤 이번 연구에 포함되었다 이전 치. 료경력이 있는 예 중 예는 이전 치료의 독성 때문에 치료5 4 를 중단하였고, 1예는 연고지 관계로 중단하였다 치료 전. 혈장CA 19-9수치는 정상수치인37 U/mL미만인 경우가5 예 이상인 경우가, 15예였다(Table 1).치료를 받은 횟수는
총91 (1-9 )회 회 로 평균4.6회였다. 5예에서 약제의 용량을 감 량해야 했으며 이유는 혈액 독성에 의한 경우가 예 구내, 3 , 염에 의한 경우가 예 오심 및 구토에 의한 경우가 예였1 , 1 다.
반응률 진행 기간 생존기간
2. , ,
전체20예 중 치료의 반응을 평가할 수 있었던 경우는 모 두 17예였다 평가가 불가능하였던 예 중 예는 회의 치. 3 2 1 료, 1예는 회 치료 후 더 이상 병원을 방문하지 않았다2 .
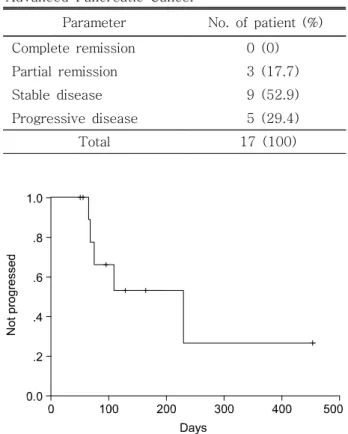
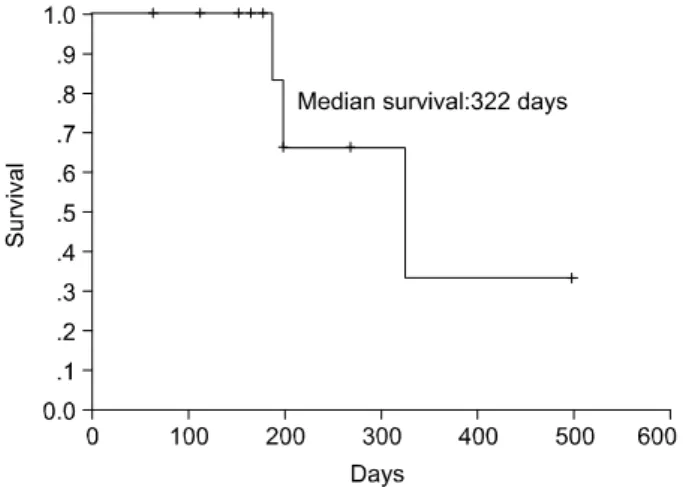
평가 가능한 17예 중 완전관해는 없었으며 부분관해는3 예 불변이 예 진행이 예로 반응률은, 9 , 5 17.7% (95%신뢰구 간, 6.2-41.0%)였다(Table 2).진행 기간은53-478 (일 평균230 일 이었고) (Fig. 1),생존기간은110-757 (일 평균322 )일 이었다 (Fig. 2).
치료의 독성 3.
총 91회의 항암화학요법 중 WHO 기준으로 도 이상의3 혈액 부작용은 백혈구감소증이12 (13.2%),회 과립구감소증 이12 (13.2%)회 였고 혈소판감소증은, 23 (24.4%) 다(Table회 였
Table 1.
Table 1.
Table 1.
Table 1. Characteristics of the 20 Patients with Advanced Pancreatic Cancer
Characteristics Age, years
Median 60.3 (40-69)
Sex, male/female 14/6 ECOG performance status
0 and 1 16
2 and 3 4
Previous chemotherapy
No 15
Yes 5
Serum CA 19-9 37 U/mL
< 5
37 U/mL
≥ 15
Number of cycles
Range 1-9
Median 4.6
Stage
IV 20
Site of metastatic disease
Liver 9
Lung 2
Peritoneum 2
ECOG, Eastern cooperative oncology group.
Table 2.
Table 2.
Table 2.
Table 2. Response to Treatment in the 17 Patients with Advanced Pancreatic Cancer
Parameter No. of patient (%) Complete remission 0 (0) Partial remission 3 (17.7) Stable disease 9 (52.9) Progressive disease 5 (29.4)
Total 17 (100)
Fig. 1.
Fig. 1.Fig. 1.
Fig. 1. Progression-free survival of 17 patients with locally ad- vanced or metastatic pancreatic carcinoma who were treated with gemcitabine, 5-FU, and cisplatin. The time to progression was 53- 478 days (median: 230 days).
Choi SB, et al. A Phase II Study of Combination Chemotherapy with Gemcitabine, 5-fluorouracil, and Cisplatin for Advanced Pancreatic Cancer 351
3). 백혈구 감소로 인한 감염과 치료의 독성에 의한 사망은 발생하지 않았다.
기준으로 도 이상의 비혈액 부작용으로는 점막염
WHO 3
이 회2 (2.2%),오심 및 구토가 회3 (3.3%)가 있었으나, 3도 이 상의 설사는 없었다(Table 4).
고 찰
전이 췌장암의 항암화학요법에 여러 임상연구가 시도되 었지만 아직 효과적인 치료방법이 없으므로 더 많은 연구가 필요하다 과거에는. 5-FU가 췌장암의 치료에 가장 많이 이 용되었고 5-FU를 기본으로 한 연구가 주를 이루었으나, 의 개발 이후 현재는 이 표준요법으로 gemcitabine gemcitabine
받아들여지고 있다. Investigational New Drug Treatment Pro- 의 보고에 의하면 명의 췌장암 환자를
gram 982 gemcitabine
단독요법으로 치료하였을 경우 14명의 완전관해를 포함하 여 반응률이12%였고, 2,380명의 환자를 대상으로 한 연구 에서 평균 생존기간이4.8개월, 1년 생존율이15%였다.17하 지만 아직 성적이 만족스럽지 못하고 더 효과적인 치료 약 제가 없으므로 췌장암의 치료에 효과가 있고gemcitabine과 상승작용이 있는 약제들로 효과적인 복합요법을 알아보기 위한 연구가 필요하다.
은 에 의해 손상된 의 복원을
Gemcitabine cisplatin DNA
억제하며 이 두 제제의 복합요법은 상승작용이 있어 췌, 장암의 치료에서 반응률이 9-36.4%이고 평균 생존기간, 이 5.6-7.4개월이었다.6,7,18 이 둘의 복합요법과 gemci- 단독요법을 비교한 연구에서 반응률은 와
tabine , 31.3%
평균 생존기간은
27.8%, 9. 개월과1 7.2개월이었지만 한, 3 상의 연구에서는 반응률이26.4%와9.2%,평균 생존기간
이 개월과7 4.7개월로 복합요법이 단독요법에 비해 반응 률과 진행까지의 시간은 증가시켰지만 평균 생존기간과, 증상의 완화에는 효과가 없었다.8,9 또 5-FU의 대사산물 이 gemcitabine monophosphate의 불활성화에 작용하는 를 억제하기 때문 deoxycytidine monophosphate deaminase
에 5-FU와gemcitabine은 상승작용이 있다.19,20이 두 제제 의 복합요법은 반응률이 5-19.2%였고 평균 생존기간은,
개월이었으며
6-10.3 ,10-13gemcitabine단독요법과 효과를 비교한 상의 연구에서도 반응률은3 6.9%와 5.6%였고 평, 균 생존기간은 6.7개월과 5.4개월로 평균 생존기간과 반 응률은 차이가 없었고5-FU에 의한 독성은 더 증가하였 다.145-FU와cisplatin도 서로 상승작용이 있어5-FU단독 요법과 cisplatin과의 복합요법은 반응률이0%와 12%, 6 개월 생존율은28%와 38%, 12개월 생존율은 9%와 17%
로 복합요법이 우수하였다.15 하지만 위의 2제 복합요법 들과gemcitabine단독요법의 치료효과를 비교할 경우 복 합요법이 더 효과적이라는 결과는 없다.
저자들이gemcitabine, 5-FU, cisplatin복합요법을 이용한 연구에서는 반응률이 17.7%, 평균 생존기간이 10.7개월로 단독요법의 반응률 평균 생존기간 개월
gemcitabine 12%, 4.8
과 비교하여 우수하였다. Gemcitabine단독요법에서는 오심 과 구토가 3.9%, 패혈증과 위장관 출혈이 각각 2.4%였고, 독성에 의해 치료를 중단한 경우가4.6%였지만,17이번 연구 에서는 제의 복합요법에도 불구하고 위중한 독성이 더 증3 가하지는 않았다 저자들과 용법은 다르지만. gemcitabine, 5- 의 복합요법 연구에서 반응률이 평균 생존
FU, cisplatin 23%,
기간이8.6개월이었고,21다른 연구에서는 반응률이19%,평 Fig. 2.
Fig. 2.
Fig. 2.
Fig. 2. Overall survival of 17 patients with locally advanced or metastatic pancreatic carcinoma who were treated with gemci- tabine, 5-FU, and cisplatin. The survival duration was 110-757 days (median survival: 322 days).
Table 3.
Table 3.
Table 3.
Table 3. Occurrence of Hematologic Toxicities in 91 Cycles of Combined Chemotherapy
Toxicity WHO grade, n (%)
Grade 1 Grade 2 Grade 3 Grade 4 Leukopenia 14 (15.4) 15 (16.5) 7 (7.7) 5 (5.5) Neutropenia 11 (12.1) 8 (8.8) 3 (3.3) 9 (9.9) Thrombocytopenia 11 (12.1) 14 (15.4) 13 (14.3) 10 (10.1)
Table 4.
Table 4.
Table 4.
Table 4. Occurrence of Non-hematologic Toxicities in 91 Cycles of Combined Chemotherapy
Toxicity WHO grade, n (%)
Grade 1 Grade 2 Grade 3 Grade 4 Mucositis 9 (9.9) 1 (1.1) 2 (2.2) 0 (0.0) Diarrhea 0 (0.0) 1 (1.1) 0 (0.0) 0 (0.0) Nausea/vomiting 14 (15.4) 5 (5.5) 2 (2.2) 1 (1.1)
352 대한소화기학회지 제: 45권 제 호5 , 2005
균 생존기간이 9.0개월이었다.22
이 연구의 제한점은 다음과 같다 첫째 연구대상이. , 20명 으로 다른 연구에 비해 수가 적었고 이 중, 17명만 반응률 을 측정할 수 있었다 둘째 연구대상 중 명은 조직검사로. , 5 췌장암이 진단되지 않았다 조직 진단을 하지 못한 경우는. 환자가 거부하였거나 종양의 크기가 약, 2 cm로 작고 혈관, 을 침범한 경우였다.
향후 더 많은 환자를 대상으로 제 복합요법의 효과에 대3 한 평가가 이루어져야 한다 또. gemcitabine과 여러 다른 제 제의 복합요법에도 아직 췌장암의 예후가 크게 개선되지 않 고 있기 때문에gemcitabine보다 더 효과적인 치료제의 개발 이 필요하다.
요 약
목적 진행 췌장암의 치료에: gemcitabine, cisplatin, 5-FU 복합화학요법의 효과와 안전성을 알아보기 위하여 연구를 시작하였다. 대상 및 방법 진행 췌장암 환자를 대상으로 하: 였다. Gemcitabine은 제 일과 제 일에1 8 800 mg/m2을 각각 정 맥 주사하였고, 5-FU은 제 일부터1 3일까지 72시간 동안 1,000 mg/m2/day을 지속해서 정맥 주사하였고, cisplatin은 gemcitabine투여24시간 후인 제 일에2 60 mg/m2을 정맥 주 사하였다 이 용법을 주 간격으로 반복 투여하였다. 3 . 결과:
년 월부터 년 월까지 명의 환자가 연구에 포 2001 11 2004 1 20
함되었다. 20명 중17명에서 치료의 효과를 측정할 수 있었 는데, 17명 중 명이 부분관해를 보여3 17.7%의 반응률을 나 타냈다 진행까지의 시간은. 7.7개월이었고 평균 생존기간은 개월이었다 혈액 독성은 총 회의 치료에서 도 이상
10.7 . 91 3
의 백혈구감소증 과립구감소증 혈소판감소증이 각각, , 12회
회 회 였다 비혈액 독성은 도
(13.2%), 12 (13.2%), 23 (24.4%) . 3 이상의 점막염과 오심 구토가 각각 회, 2 (2.2%), 3 (3.3%)회 였 다. 결론: Gemcitabine, 5-FU, cisplatin복합화학요법은 진행 췌장암의 치료에 효과적이며 위중한 독성은 발생하지 않았, 다.
색인단어: 췌장암, Gemcitabine, 5-fluorouracil, Cisplatin
참고문헌
1. Evans DB, Abbruzzese JL, Willett CG. Cancer of the pancreas. In: DeVita VT, Hellman S, Rosenberg SA, eds.
Cancer. Principles and practice of oncology. Volume 1. 6th ed. Philadelphia: Lippincott, Williams & Wilkins, 1997:
1126-1161.
2. Heinemann V. Gemcitabine: progress in the treatment of pan-
creatic cancer. Oncology 2001;60:8-18.
3. Carmichael J, Fink U, Russell RC, et al. Phase II study of gemcitabine in patients with advanced pancreatic cancer. Br J Cancer 1996;73:101-105.
4. Crino L, Mosconi AM, Calandri C, et al. Gemcitabine in advanced pancreatic cancer: a phase II trial. Am J Clin Oncol 2001;24:296-298.
5. Burris HA 3rd, Moore MJ, Andersen J, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreatic cancer: a randomized trial. J Clin Oncol 1997;15:2403-2413.
6. Philip PA, Zalupski MM, Vaitkevicius VK, et al. Phase II study of gemcitabine and cisplatin in the treatment of patients with advanced pancreatic carcinoma. Cancer 2001;92:569-577.
7. Cascinu S, Labianca R, Catalano V, et al. Weekly gemci- tabine and cisplatin chemotherapy: a well-tolerated but in- effective chemotherapeutic regimen in advanced pancreatic cancer patients. A report from the Italian Group for the Study of Digestive Tract Cancer (GISCAD). Ann Oncol 2003;14:
205-208.
8. Colucci G, Giuliani F, Gebbia V, et al. Gemcitabine alone or with cisplatin for the treatment of patients with locally advanced and/or metastatic pancreatic carcinoma: a prospec- tive, randomized phase III study of the Gruppo Oncologia dell'Italia Meridionale. Cancer 2002;94:902-910.
9. Wang X, Ni Q, Jin M, et al. Gemcitabine or gemcitabine plus cisplatin for in 42 patients with locally advanced or meta- static pancreatic cancer. Zhonhua Zhong Liu Za Zhi 2002;
24:404-407.
10. Oettle H, Arning M, Pelzer U, et al. A phase II trial of gemcitabine in combination with 5-fluorouracil (24-hour) and folinic acid in patients with chemonaive advanced pancreatic cancer. Ann Oncol 2000;11:1267-1272.
11. Hidalgo M, Castellano D, Paz-Ares L, et al. Phase I-II study of gemcitabine and fluorouracil as a continuous infusion in patients with pancreatic cancer. J Clin Oncol 1999;17:585- 592.
12. Berlin JD, Adak S, Vaughn DJ, et al. A phase II study of gemcitabine and 5-fluorouracil in metastatic pancreatic cancer:
an Eastern Cooperative Oncology Group Study (E3296).
Oncology 2000;58:215-218.
13. Kanat O, Evrensel T, Kurt E, et al. Treatment of metastatic pancreatic cancer with a combination of gemcitabine and 5-fluorouracil: a single center phase II study. Tumor 2004;
90:192-195.
14. Berlin JD, Catalano P, Thomas JP, et al. Phase III study of gemcitabine in combination with fluorouracil versus gemci-
최상봉 외 인 진행성 췌장암의 젬시타빈3 . , 5-FU,시스플라틴 복합화학요법에 관한 상 연구2 353
tabine alone in patients with advanced pancreatic carcinoma:
Eastern Cooperative Oncology Group Trial E2297. J Clin Oncol 2002;20:3270-3275.
15. Ducreux M, Rougier P, Pignon JP, et al. A randomized trial comparing 5-FU with 5-FU plus cisplatin in advanced pan- creatic carcinoma. Ann Oncol 2002;13:1185-1191.
16. Moon Y, Todoroki T, Ohno T, Fukao K, Little JB. Killing effects of 5-fluorouracil on biliary tract cancer cell lines. Int J Oncol 1999;14:253-257.
17. Storniolo AM, Enas NH, Brown CA, Voi M, Rothenberg ML, Schilsky R. An investigational new drug treatment program for patients with gemcitabine: results for over 3000 patients with pancreatic carcinoma. Cancer 1999;85:1261-1268.
18. Bergman AM, Ruiz van Haperen VW, Veerman G, Kuiper CM, Peters GJ. Synergistic interaction between cisplatin and
gemcitabine in ovarian and colon cancer cell lines. Adv Exp Med Biol 1994;370:139-143.
19. Ren Q, Kao V, Grem JL. Cytotoxicity and DNA fragmen- tation associated with sequential gemcitabine and 5-fluoro- 2'-deoxyuridine in HT-29 colon cancer cells. Clin Cancer Res 1998;4:2811-2818.
20. Schulz L, Schalhorn A, Wilmanns W, et al. Synergistic in- teraction of gemcitabine and 5-fluorouracil in colon cancer cells. Proc Am Soc Clin Oncol 1998;17(abstr):251A.
21. El-Rayes BF, Zalupski MM, Shields AF, et al. Phase II study of gemcitabine, cisplatin, and infusional fluorouracil in ad- vanced pancreatic cancer. J Clin Oncol 2003;21:2920-2925.
22. Novarino A, Chiappino I, Bertelli GF, et al. Phase II study of cisplatin, gemcitabine and 5-fluorouracil in advanced pan- creatic cancer. Ann Oncol 2004;15:474-477.