Original Article Korean J Urogenit Tract Infect Inflamm 2014;9(1):39-43
3차 의료기관의 최근 10년간 성인 부고환염의 원인균주의 항생제 저항성의 변화
박종진, 김종욱, 배재현, 문두건, 오미미
고려대학교 구로병원 비뇨기과
전체 글
고려대학교 구로병원 비뇨기과
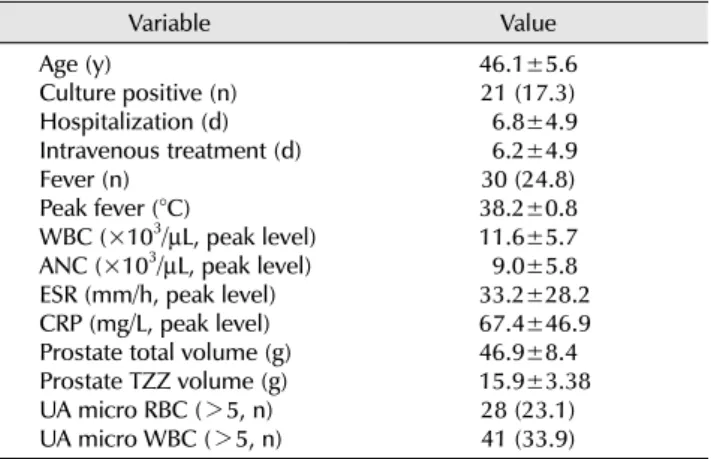
수치

관련 문서
Methods: I conducted a retrospective analysis of clinical records of children aged between 4 and 19 years who were treated with flunarizine for headache at
Keywords □ acute coronary syndrome, discharge medication patterns, Korea, tertiary hospital, follow-up evaluation, troponin-T,
Long-term outcomes of short dental implants supporting single crowns in posterior region: a clinical retrospective study of 5-10 years.. Osteotome sinus
This study is an analysis of distribution of patient who installed Endopore Ⓡ at maxilla in Chosun University Dental hospital and types of implant for about 4
Objective: The purpose of this study was to analyze recent trend in incidence of basal cell carcinoma and squamous cell carcinoma in patients from the Gwangju City
In this thesis, we introduce a Hurwitz polynomial ring and study the irreduciblity of Hurwitz polynomials over We also investigate the irreduciblilty of
The purpose of this study is to investigate how participation in 8-week swimming and resistance exercise programs affects changes in health fitness and
In this study, 12 weeks of aerobic exercise was conducted in middle-aged women aged 45 to 55 years with a body fat rate of 30% or more to determine the effects of blood
