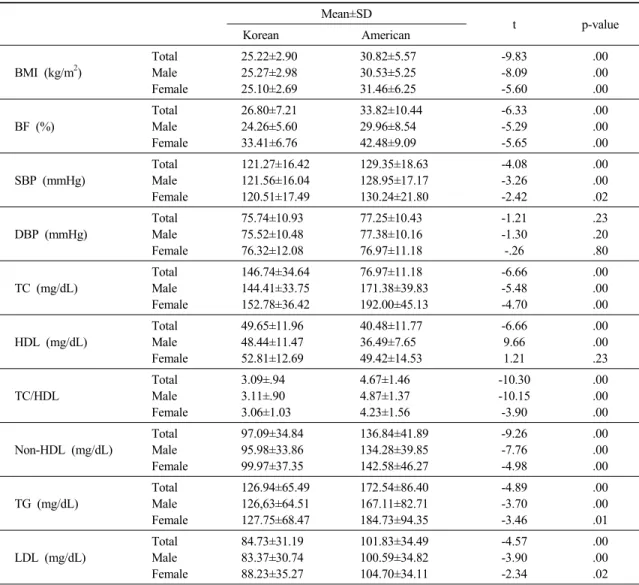
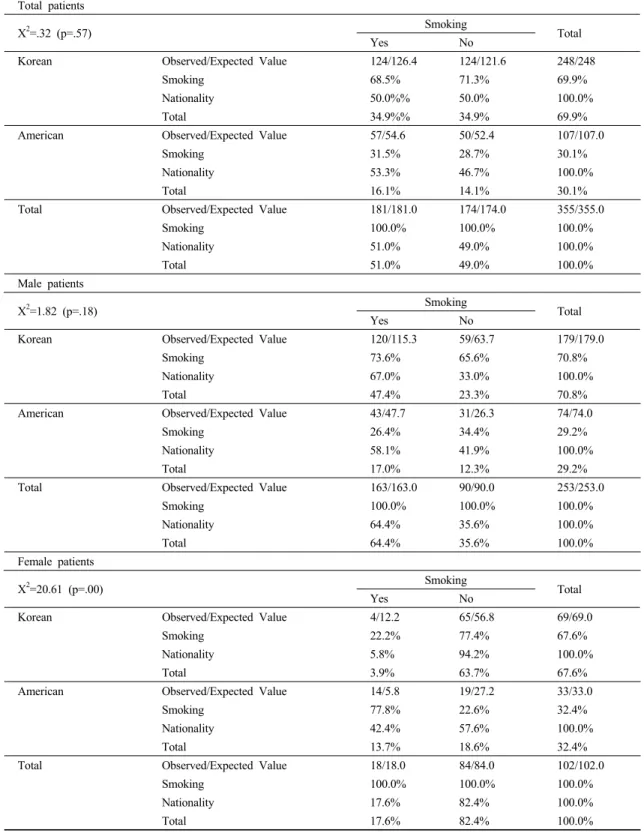
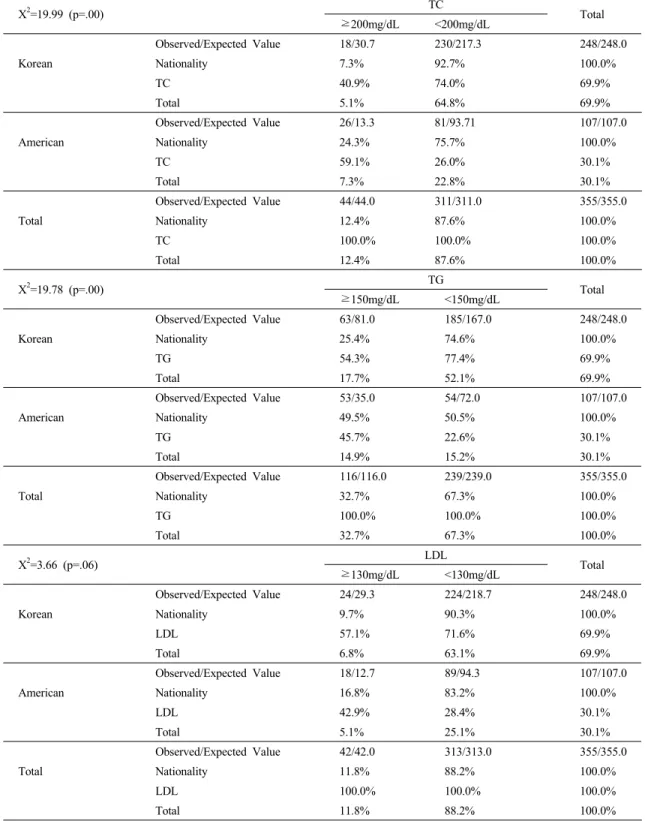
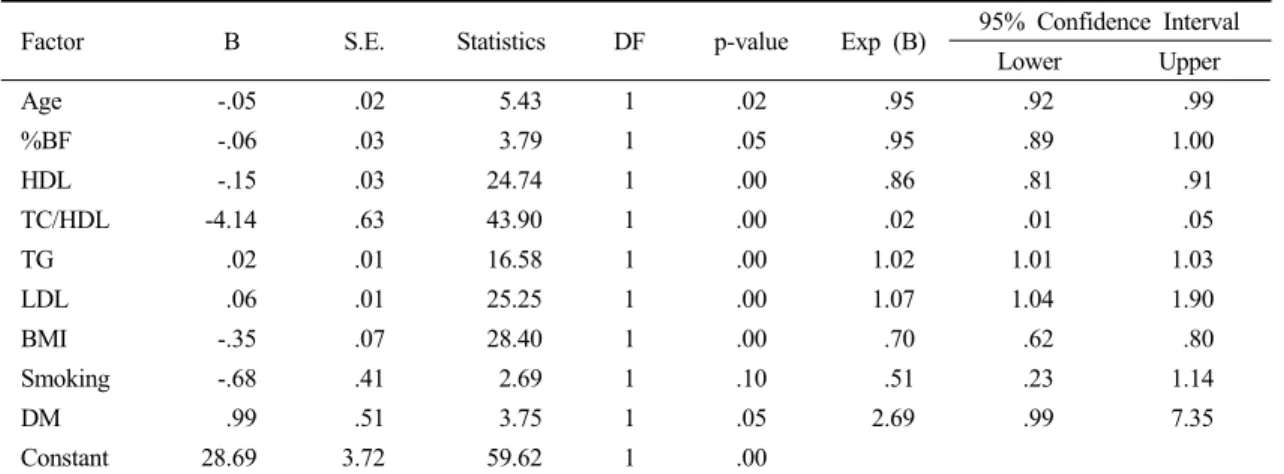
The Characteristics of Risk Factors in Korean CAD Patients Comparing to American Counterpart and Its Implications to Prevention of CAD
12
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
(12)
수치
관련 문서
3) ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
Method : : : : We evaluate clinical features of 714 Korean vitiligo patients who lived in the Gwangju chonnam province(315 males and 399 females).. Results
Drug-intoxicated patients were predominantly male, with the highest incidence of intoxication among patients above the seventh decade of age(21.5%) and the
The Effects of Culture Learning Through American TV Dramas on English Listening, Vocabulary Skills and Interest of Korean Elementary
Records of the Korean American Foundation Hawaii 호놀룰루 한인기독교회 관련 자료.. Korean Christian Church (Honolulu) Collection 사진
Third, the analysis of the body-centered vertical speed between male.. and female students showed that male students appeared faster than female students at
Prevalence of Undiagnosed Diabetes and Related Factors in Korean Postmenopausal Women:.. The 2011-2012 Korean National Health and
