- 12 -
Ciliary Beat Frequency in the Airways of Humans:
Influences of Lidocaine, Age, Sex and Smoking *
Seung Sin Lee, M.D.
1, In-Ho Jung, M.D.
2, Ji-Hun Mo, M.D.
2, Chul-Gyu Yoo, M.D.
3, Chul Hee Lee, M.D.
2,
Won-Jin Yi, Ph.D.
4and Chae-Seo Rhee, M.D.
2ABSTRACT
We measured the ciliary beat frequencies (CBFs) in respiratory ciliated epithelia obtained from the nasal cavity, trachea, and bronchus of 40 subjects during fiberoptic bronchoscopy, using a video-computerized analysis technique. The subjects were classified into various groups based on a range of parameters, including sex, age, history of smoking and whether or not a local anesthetic has been used and mean values of CBFs were analyzed between these groups. The ciliary beat of nasal epithelial cells was significantly faster than that of the trachea or bronchus (p=0.008). There were significant positive correlations between the CBFs at the nasal cavity and trachea (R
2=0.467, p<0.001), nasal cavity and bronchus (R
2=0.566, p<0.001), and trachea and bronchus (R
2=0.541, p<0.001). Subjects older than 60 years of age had significantly slower CBFs at all three sites and than their younger counterparts (p<0.001). Neither sex nor smoking affected the ciliary motility at any site of the respiratory tract.
There was no significant difference in the nasal CBFs between the anesthetized and non-anesthetized sides. In conclusion, this study can provide important clinical data on the CBFs of respiratory tracts in humans.
KEY WORDS
:Frequency・Cilia・Ciliary motility・Respiratory tract.
INTRODUCTION
The mucociliary system, which is composed of cilia, mucus, and periciliary fluid, is an integral part of air- way defense. Many chemical, biological, and physical agents and diseases can alter the mucociliary function.
The main function of the mucociliary system is to eliminate inhaled particles. The overall propulsive effect
depends on the arrangement of the cilia and ciliary beat frequency (CBF).
1)Because of its invasiveness, obtaining samples of the respiratory epithelium from the trachea or bronchus for the purpose of measuring CBF is a difficult procedure to perform. On the other hand, obtaining samples of the nasal mucosa is simpler, safer, and easier. Therefore, if it can be shown that there is a correlation between CBFs of the nasal mucosa, trachea, and bronchus, it would be possible to predict CBF of the trachea or bronchus from that of the nasal cavity. There have been several reports giving the values of CBF at different sites of human or animal airway
2-6)and the effects of anes- thesia on CBF.
7-9)To date, however, there have been few studies comparing CBFs of these three different sites (nasal cavity, trachea, and bronchus) of the human airway. Furthermore, most of the previous studies were performed using a photoelectric method, in which the number of cilia, which was analyzed for each measure- ment, is quite limited, resulting in possible experimental error.
2)We developed a video-computerized analysis tech-
*
This study was supported by grants of Ministry of Health &
Welfare (02-PJ3-PG10-31401-0010) and Korea Research Foun- dation (KRF-2002-015-EP 0102), Republic of Korea.
1
Departments of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, Ewha Womans University, Seoul,
2Depar- tments of Otorhinolaryngology-Head and Neck Surgery,
3Internal Medicine, College of Medicine and
4Oral and Maxillofacial Ra- diology, College of Dentistry, Seoul National University, Seoul, Korea
Address correspondences and reprint requests to Chae-Seo Rhee, M.D., Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University College of Medicine, 28 Yongon-dong, Chongno-gu, Seoul 110-744, Korea
Tel:82-2-760-3991, Fax:82-2-745-2387 E-mail:[email protected]
Accepted for publication on August 18, 2004
nique, which made it possible to measure CBF in either a single cell or multiple ciliated cells.
10)The purpose of this study was to compare CBFs of the human upper and lower airway, according to various parameters, in- cluding whether or not anesthesia has been or not, age, sex, and smoking, using this video-computerized an- alysis technique.
METHODS Subjects
Respiratory ciliated epithelial cells of the turbinate, trachea, and main bronchus were obtained from 40 subjects (30 males and 10 females) during fiberoptic bronchoscopy with informed written consent. All of the subjects underwent fiberoptic bronchoscopy for respiratory symptoms such as chronic cough, sputum, and chest pain but none of them had any visible lesions in the respiratory tract from the nasal cavity to the main bronchus. They had no history of chronic nasal disease, previous nasal surgery or prolonged use of to- pical medication. They denied swimming, taking any airplane flights or having any upper respiratory in- fections for at least 1 month prior to bronchoscopy.
Their mean age was 56.2 years (range, 32 to 75 years).
Twenty-six of 40 patients (65%) were smokers.
Preparation of respiratory ciliated epithelial cells
Nasal ciliated epithelial cells were taken from the lateral portion, 15 mm behind the anterior end of the inferior turbinates of both nasal cavities, with topical anesthesia of 4% lidocaine being administered on one side using a 2-mm diameter cytology brush (BC-15 AE;Olympus, Tokyo, Japan) and no anesthesia on the other side. Following premedication with pethidine HCl and atropine sulfate and the intraoral spraying of 4% lidocaine, ciliated epithelia were harvested at 5 cm above and 3 cm distal to the carina, respectively. The harvested epithelial cells were incubated in Dulbecco’s Modified Eagle Medium-Ham’s nutrient F12 (DMEM- F12;Gibco BRL, Grand Island, NY) at 37℃ under 5% CO
2in an incubator for 1 hour. A cluster of epi- thelial cells was placed in a specially designed sterile culture dish, which was maintained at 37℃ throughout
the experiment.
Measurement of ciliary beat frequency
Ciliary beat observed at x 1000 magnification was recorded using a charged coupled device (CCD) ca- mera (Digistar;Xomed, Jacksonville, FL). The analog signal on the video monitor was sent to a personal com- puter, which digitized and analyzed the signal by means of a program we developed based on the fast-Fourier transform (FFT).
10)The measured brightness intensi- ties from the selected region of ciliated mucosa yielded a dominant peak in power spectrum, which was es- timated using FTT. We measured CBFs in the most active cells of 5 consecutive fields and took the mean value as the CBF of the sampled tissue.
Statistical analysis
CBFs were compared between different sites of the respiratory tract and between groups of subjects con- stituted as a function of sex, smoking, and age using Mann-Whitney U test. The differences in the CBFs at each site of the respiratory tract between subgroups divided according to decade-intervals of age were an- alyzed using the Kruskall-Wallis test. Student t-test was used to compare CBFs of the nasal mucosa bet- ween the anesthetized and non-anesthetized sides. Corr- elations among CBFs at three sites of the respiratory tract were analyzed using linear regression analysis.
For all statistical procedures, SPSS for windows version 10.0 (SPSS Inc., Chicago, IL) was used. Differences with p values of less than 0.05 were considered as being statistically significant.
RESULTS
The mean values of the CBFs of the nasal cavity, trachea, and bronchus were 8.53±1.40 Hz, 7.67±
1.51 Hz, and 7.65±1.30 Hz, respectively. The ciliary beat of nasal cavity was significantly faster than that of the trachea or bronchus ( p=0.008), while there were no significant differences in the CBFs between the trachea and bronchus.
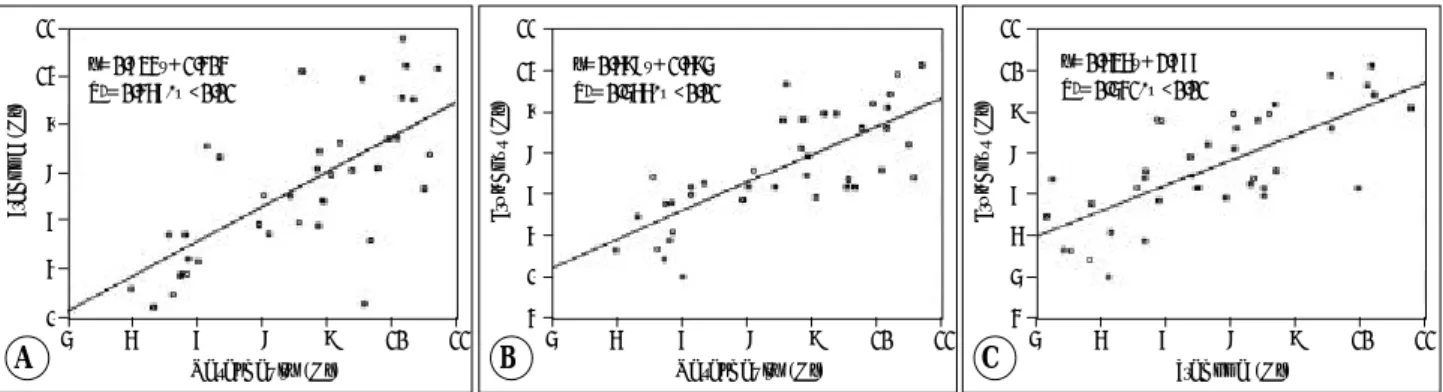
There were significant positive correlations between
the CBFs of the nasal cavity and trachea (y=0.734x+
1.404, R
2=0.467, p<0.001), nasal cavity and bronchus (y=0.698x+1.695, R
2=0.566, p<0.001), and trachea and bronchus (y=0.636x+2.777, R
2=0.541, p<0.001) (Fig. 1).
The mean values of the CBFs of nasal epithelial cells of the anesthetized and non-anesthetized sides were 8.29±1.33 Hz and 8.53±1.40 Hz, respectively. This difference in values was not statistically significant.
Table 1 shows the CBFs of the nasal cavity, trachea, and bronchus according to sex, age, and smoking, res- pectively. The CBFs at all three different sites of the respiratory tract in subjects under the age of 60 years were faster than those of their older counterparts. Fig. 2 shows the CBFs of the nasal cavity, trachea, and bro- nchus of subgroups divided according to decade-inter- vals of age. The CBFs of all three sites decreased sig- nificantly with age. However, no statistically significant differences were observed in the CBFs of the nasal cavity, trachea, or bronchus in terms of sex or smoking.
DISCUSSION
In the present study, the mean CBFs of all the sam-
ples taken from the nasal cavity, trachea, and bronchus were slower than those of other studies, in which the reported values ranged from 10 to 16 Hz.
4)11-14)This difference might be a result of the effect of the preme- dication with the intramuscular administration of pe- thidine HCl (25 to 50 mg) and atropine sulfate (0.5 mg). Acetylcholine is believed to accelerate CBF, and this effect can be blocked by atropine.
15)Atropine, a nonselective muscarinic receptor antagonist, signifi- cantly blocks methacholine-induced ciliostimulation in vitro
16)and also decreases mucociliary clearance in vivo.
17)The ciliary beat of the nasal cavity in this study was significantly faster than those of the trachea and bron- chus. This is in contrast to the results of a previous study,
4)which reported that there was no significant difference between the nasal and tracheal CBFs. The reason for this discrepancy is not clear, but is probably
Table 1. Ciliary beat frequency (Hz) at three different sites of re- spiratory epithelium
Nasal cavity Trachea Bronchus Sex Male (n=30) 8.67±1.41 7.57±1.44 7.67±1.24 Female (n=10) 8.12±1.35 7.96±1.75 7.59±1.53 Age, yr 30-59 (n=24) 9.43±0.86* 8.38±1.34* 8.35±1.02*
60-79 (n=16) 7.18±0.85 6.60±1.06 6.61±0.94 Smoking Smoker (n=26) 8.56±1.38 7.64±1.43 7.71±1.33
Non-smoker (n=14)
8.48±1.50 7.71±1.70 7.54±1.29 Values are mean±SD., *:p<0.001 vs. their older counterparts
Fig. 1. Correlation analyses of the relationship between CBFs of the nasal cavity, trachea, and bronchus. A:CBFs at nasal cavity vs trachea (n=40, y=0.734x+1.404, R2=0.467, p<0.001). B:CBFs at nasal cavity vs bronchus (n=40, y=0.698x+1.695, R2=0.566, p<0.001). C:
CBFs at trachea vs bronchus (n=40, y=0.636x+2.777, R2=0.541, p<0.001).
11 10 9 8 7 6
55 6 7 8 9 10 11 Nasal cavity (Hz)
y=0.734x+1.404 R2=0.467, p<0.01
Trachea (Hz)
A
11 10 9 8 7 6 5
45 6 7 8 9 10 11 Nasal cavity (Hz)
Bronchus (Hz)
y=0.698x+1.695 R2=0.566, p<0.01
B
11 10 9 8 7 6 5
45 6 7 8 9 10 11 Trachea (Hz)
Bronchus (Hz)
y=0.636x+2.777 R2=0.541, p<0.01
C
30-39 40-49 50-59 60-69 70-79 Age (year)
CBF (Hz)
12 10 8 6 4 2 0
N T B
Fig. 2. Ciliary beat frequency (Hz) at three different sites of res- piratory epithelium analyzed by age. Data shown represents the mean and standard deviation. CBFs of the nasal cavity (N), trachea (T) and bronchus (B) show significant differences bet - ween age groups (in all groups, p<0.05).
related to the use of a different experimental specimen and methodology. However, we previously obtained similar results from animal studies involving mouse, rat, and guinea pig (data not shown). Furthermore, this result is reasonable considering that the nasal cavity is the port of entry for many noxious particles present in the environment.
In this study, there was no difference between the CBFs of trachea and bronchus. Many studies
18-21)in animals or humans reported that as the mucus passes from the peripheral to the central airways, its transport velocity increases. Why, in spite of this increased tran- sport velocity, is there no difference between the CBFs of trachea and bronchus? This can be attributed to the following facts. Many factors, other than CBF, inclu- ding ciliary metachronicity and the properties of the mucus, affect mucociliary clearance. Furthermore, in contrast to in vitro ciliary activity, many chemical and mechanical environments, including nerve impulses,
22)hormones,
23-25)cytokines
26)27)and the viscoelasticity and amount of mucus,
28)can exert an influence on in vivo ciliary motility.
This study showed that there were strong positive correlations between the CBFs of all three sites of the respiratory tract. Based on these positive correlations, we can predict the CBFs of trachea and bronchus, without measuring them directly, from the CBF of the nasal cavity, whose measurement is less invasive. Ele- vated intracellular Ca
2+is a fundamental requirement for CBF to be increased. Chemical or mechanical stre- sses induce the release of 5’ nucleotides (ATP and UTP) into the extracellular compartment from airway epithelial cells. The interaction of these extracellular nucleotides with purinoceptors at the apical membrane of epithelial cells coordinates, by triggering intracellular Ca
2+mobilization, airway mucociliary clearance res- ponse, including an increase in CBF.
29)Another po- ssible explanation for the strong positive correlation between the CBFs of airway epithelia observed in this study is that there may be an intrinsic pacemaker within the ciliated cells, which controls the rhythmicity of ciliary activity in a subject-specific manner.
Gender did not affect the CBFs of the nasal cavity, trachea, or bronchus. This result is consistent with the results of previous studies conducted in vivo or in vitro.
4)30)Interestingly, there was no significant difference in
nasal, tracheal, and bronchial CBFs between the smo- kers and non-smokers in this study. There is some con- troversy surrounding the effect of smoking on ciliary movement.
2)13)31)Stanley and coworkers reported that there was no significant difference between the nasal CBFs of smokers and non-smokers, in spite of there being a significant decrease in nasal mucociliary clear- ance in smokers compared with that in non-smokers.
31)On the other hand, acute cigarette smoke exposure re- sulted in a marked loss of ciliated cells from the bron- chial luminal surface and a significant increase in bron- chial fluid dynein concentrations.
32)Taken together, these reports and our results suggest that cigarette smoke may cause the structural deformity of certain cilia, without decreasing the motility of the remaining cilia. Another possible explanation for this insignificant difference in the CBFs between smokers and non-smo- kers is the reversibility of ciliary activity, following structural and functional injury. If cilia have such reversibility, then this result is possible, because all of the subjects tested in this study quit smoking tem- porarily at least one month before the examination. Ci- garette smoke can also change the viscoelastic property of respiratory mucus. Smokers have an increased num- ber of goblet cell hyperplasia and epithelial inflamm- ation in the peripheral airway,
33)resulting in increased watery mucus secretion and decreased viscoelasticity of the mucus.
34)Because coordination of many com- ponents, including ciliary motility and the amount and rheologic property of the mucus and periciliary fluid, is essential for proper functioning of mucociliary clea- rance system, the influence of smoking should be dealt with after taking these factors into account.
The results concerning the influence of age differ between the various published reports.
2)4)14)35)In this study, nasal, tracheal and bronchial CBFs showed a tendency to decrease as patients aged over their seventh decade. In other reports, it was postulated that subjects older than 40 years of age had significantly slower CBFs and a higher percentage of ultrastructural abnor- malities of cilia.
14)These findings, together with a de- crease in immunity, may help to explain the frequent respiratory tract infections, which are observed in the elderly.
We did not observe any significant influence of the topical application of lidocaine on ciliary activity.
Although the results of this study differ from those of
previous studies,
4)8)it is generally accepted that the topical application of lidocaine does not significantly decrease either ciliary activity or mucociliary clear- ance.
13)36)This result should provide clinicians with the necessary reassurance to confidently use intranasal anesthetics for endoscopic treatment or diagnosis.
In summary, this study demonstrated that the ciliary activity of the nasal mucosa was significantly faster than that of the trachea or bronchus, and that ciliary activity shows a tendency to decrease with age, whereas neither gender, smoking nor topical lidocaine signifi- cantly affect ciliary activity. It is hoped that this study will provide important clinical data for the study of the pathophysiology of the human mucociliary system.
REFERENCES
1) Satir P, Sleigh MA. The physiology of cilia and mucociliary intera- ctions. Annu Rev Physiol 1990;52:137-55.
2) Yager JA, Ellman H, Dulfano MJ. Human ciliary beat frequency at three levels of the tracheobronchial tree. Am Rev Respir Dis 1980;
121:661-5.
3) Rutland J, Griffin W, Cole P. Nasal brushing and measurement of ciliary beat frequency. An in vitro method for evaluating pharma- cologic effects on human cilia. Chest 1981;80:865-7.
4) Roth Y, Aharonson EF, Teichtahl H, Baum GL, Priel Z, Modan M.
Human in vitro nasal and tracheal ciliary beat frequencies: com- parison of sampling sites, combined effect of medication, and de- mographic relationships. Ann Otol Rhinol Laryngol 1991;100:
378-84.
5) Joki S, Saano V. Ciliary beat frequency at six levels of the respi- ratory tract in cow, dog, guinea-pig, pig, rabbit and rat. Clin Exp Pharmacol Physiol 1994;21:427-34.
6) Clary-Meinesz C, Mouroux J, Huitorel P, Cosson J, Schoevaert D, Blaive B. Ciliary beat frequency in human bronchi and bronchioles.
Chest 1997;111:692-7.
7) Mostow SR, Dreisin RB, Manawadu BR, LaForce FM. Adverse effects of lidocaine and methylparaben on tracheal ciliary activity.
Laryngoscope 1979;89:1697-701.
8) Ingels KJ, Nijziel MR, Graamans K, Huizing EH. Influence of cocaine and lidocaine on human nasal cilia. Beat frequency and harmony in vitro. Arch Otolaryngol Head Neck Surg 1994;120:
197-201.
9) Rutland J, Griffin W, Cole PJ. An in vitro model for studying the effects of pharmacological agents on human ciliary beat frequency:
effects of lignocaine. Br J Clin Pharmacol 1982;13:679-83.
10) Min YG, Yun YS, Rhee CS, Sung MW, Lee KS, Ju MS, et al.
Effects of phenylephrine on ciliary beat in human nasal respiratory epithelium: quantitative measurement by video-computerized an- alysis. Laryngoscope 1998;108:418-21.
11) Moriarty BG, Robson AM, Smallman LA, Drake-Lee AB. Nasal mucociliary function: comparison of saccharin clearance with ciliary beat frequency. Rhinology 1991;29:173-9.
12) Joki S, Toskala E, Saano V, Nuutinen J. Correlation between ciliary beat frequency and the structure of ciliated epithelia in pathologic human nasal mucosa. Laryngoscope 1998;108:426-30.
13) Agius AM, Smallman LA, Pahor AL. Age, smoking and nasal ciliary
beat frequency. Clin Otolaryngol 1998;23:227-30.
14) Ho JC, Chan KN, Hu WH, Lam WK, Zheng L, Tipoe GL, et al.
The effect of aging on nasal mucociliary clearance, beat frequency, and ultrastructure of respiratory cilia. Am J Respir Crit Care Med 2001;163:983-8.
15) Hybbinette JC, Mercke U. Effects of the parasympathomimetic drug methacholine and its antagonist atropine on mucociliary activity.
Acta Otolaryngol 1982;93:465-73.
16) Yang B, Schlosser RJ, McCaffrey TV. Signal transduction pathways in modulation of ciliary beat frequency by methacholine. Ann Otol Rhinol Laryngol 1997;106:230-6.
17) Ruhle KH, Kohler D, Matthys H. Mucociliary clearance 24 hours following fiber optic bronchoscopy under local anesthesia and atro- pine premedication. Prax Klin Pneumol 1985;39:99-101.
18) Morrow PE, Gibb FR, Gazioglu KM. A study of particulate clear- ance from the human lungs. Am Rev Respir Dis 1967;96:1209-21.
19) Asmundsson T, Kilburn KH. Mucociliary clearance rates at various levels in dog lungs. Am Rev Respir Dis 1970;102:388-97.
20) Lourenco RV, Klimek MF, Borowski CJ. Deposition and clearance of 2 micron particles in the tracheobronchial tree of normal subjects- smokers and nonsmokers. J Clin Invest 1971;50:1411-20.
21) Serafini SM, Wanner A, Michaelson ED. Mucociliary transport in central and intermediate size airways: effect of aminophyllin. Bull Eur Physiopathol Respir 1976;12:415-22.
22) Chu S, Kennedy JR. Intra-epithelial palatine nerve endings and their regulation of ciliary activity of frog palate epithelium. J Comp Phy- siol 1994;175:505-18.
23) Kobayashi K, Tamaoki J, Sakai N, Kanemura T, Chiyotani A, Shi- basaki T, et al. Corticotropin-releasing factor and adrenocortico- tropin stimulate ciliary motility in rabbit tracheal epithelium. Life Sci 1989;45:2043-9.
24) Tamaoki J, Kobayashi K, Sakai N, Kanemura T, Horii S, Isono K, et al. Atrial natriuretic factor inhibits ciliary motility in cultured ra- bbit tracheal epithelium. Am J Physiol 1991;260:C201-5.
25) Tamaoki J, Kondo M, Takeuchi S, Takemura H, Nagai A. Vaso- pressin stimulates ciliary motility of rabbit tracheal epithelium:
role of V1b receptor-mediated Ca2+ mobilization. Am J Respir Cell Mol Biol 1998;19:293-9.
26) Rhee CS, Hong SK, Min YG, Lee CH, Lee KS, Ahn SH, et al.
Effects of IL-1 beta, TNF-alpha, and TGF-beta on ciliary beat fre- quency of human nasal ciliated epithelial cells in vitro. Am J Rhinol 1999;13:27-30.
27) Laoukili J, Perret E, Willems T, Minty A, Parthoens E, Houcine O, et al. IL-13 alters mucociliary differentiation and ciliary beating of human respiratory epithelial cells. J Clin Invest 2001;108:1817-24.
28) Seybold ZV, Mariassy AT, Stroh D, Kim CS, Gazeroglu H, Wanner A. Mucociliary interaction in vitro: effects of physiological and in- flammatory stimuli. J Appl Physiol 1990;68:1421-6.
29) Homolya L, Steinberg TH, Boucher RC. Cell to cell communication in response to mechanical stress via bilateral release of ATP and UTP in polarized epithelia. J Cell Biol 200018;150:1349-60.
30) Passali D, Bianchini Ciampoli M. Normal values of mucociliary transport time in young subjects. Int J Pediatr Otorhinolaryngol 1985;9:151-6.
31) Stanley PJ, Wilson R, Greenstone MA, MacWilliam L, Cole PJ.
Effect of cigarette smoking on nasal mucociliary clearance and ciliary beat frequency. Thorax 1986;41:519-23.
32) Sisson JH, Papi A, Beckmann JD, Leise KL, Wisecarver J, Bro- dersen BW, et al. Smoke and viral infection cause cilia loss de- tectable by bronchoalveolar lavage cytology and dynein ELISA.
Am J Respir Crit Care Med 1994;149:205-13.
33) Saetta M, Turato G, Baraldo S, Zanin A, Braccioni F, Mapp CE, et
al. Goblet cell hyperplasia and epithelial inflammation in peripheral airways of smokers with both symptoms of chronic bronchitis and chronic airflow limitation. Am J Respir Crit Care Med 2000;161:
1016-21.
34) Rubin BK, Ramirez O, Zayas JG, Finegan B, King M. Respiratory mucus from asymptomatic smokers is better hydrated and more
easily cleared by mucociliary action. Am Rev Respir Dis 1992;145:
545-7.
35) Jorissen M, Willems T, Van der Schueren B. Nasal ciliary beat fre- quency is age independent. Laryngoscope 1998;108:1042-7.
36) Wanner A. Clinical aspects of mucociliary transport. Am Rev Respir Dis 1977;116:73-125.