J Korean Neurosurg Soc/Volume 30/January, 2001 81 KISEP Case Reports J Korean Neurosurg Soc 30::::81-84, 2001
단락술후 발생한 긴장성 기뇌증
- 증 례 보 고 -
순천향대학교 의과대학 신경외과학교실
이재학·김범태·조성진·신원한·최순관·변박장
= Abstract =
Tension Pneumocephalus after Shunting for Hydrocephalus
--
-- Case Report ----
Jae-Hack Lee, M.D., Bum-Tae Kim, M.D., Sung-Jin Cho, M.D., Won-Han Shin, M.D., Soon-Kwan Choi, M.D., Bark-Jang Byun, M.D.
Department of Neurosurgery, Soonchunhyang University Hospital, Seoul, Korea
neumocephalus is exceedingly rare in the absence of trauma or recent surgery. It is most commonly seen after severe head injury, with disruption of the dura and subsequent cerebrospinal fluid leakage. Intracranial air has also been reported as a complication of shunting. This may be secondary to intermittent shunt failure or a persistent communication between the extracranial and intracranial space that permits the entrance of air.
In the present case, air appeared to enter the ventricular system through the fistula that connected the frontal sinus.
This air replaced the CSF being drained into the peritoneal cavity by the shunt. The decrease of intracranial pressure after a shunt might play a role in causing pneumocephalus. We report a case of tension pneumocephalus after shunting for hydrocephalus as a life-threatning complication.
KEY WORDS:Tension pneumocephalus・Shunting・Hydrocephalus・Head trauma.
서 론
대부분의 기뇌증은 부비동이나 유양돌기동에 발생된 기 저골절과 연관되어 발생된다. 그 밖의 경우로는 선천적인 기저골의 결손, 부비동이나 기저골에 발생한 종양이나 골 수염, 또는 수술 등에 의해 발생하는 것으로 알려져 있다.
단락술후 기뇌증이 발생하는 경우는 매우 드문 것으로 현 재까지 문헌고찰상 12례가 보고되고 있다. 이에 저자들은 단락술후 긴장성 기뇌증이 발생하여 사망한 사례를 치험하 였기에 문헌고찰과 함께 보고하는 바이다.
증 례
54세 남자로 내원 1개월전 작업중 발생된 우측 외상성
뇌실질내출혈로 타병원에서 개두술 및 혈종제거술을 시행 받은 후 전원 되었다. 동반손상으로 왼쪽 전두골의 함몰성 분쇄골절이 있었으나 기뇌증은 보이지 않았다(Fig. 1). 의 식은 반혼수 상태였으며 흡입성 페렴의 소견이 있어 보존 적 치료를 시행 후 의식은 호전되고 보행이 가능한 상태로 회복되었다. 환자는 3개월후 보행장애와 뇨실금이 있어 뇌전 산화단층촬영을 시행한 결과 정상압수두증으로 진단하고 요 추복강간 단락술을 시행하였다(Fig. 2). 술후 환자의 상태가 호전되었다가 약 1개월 후 다시 뇨실금이 발생되고 점차 의 식이 기면 상태로 되었다. 단순 방사선 촬영과 뇌전산화단 층촬영상 전두부 및 뇌실내에 광범위한 긴장성 기뇌증을 보였다(Fig. 3).
수술 소견 및 술 후 경과:양쪽 전두부 개두술을 시행하 자 골편이 안으로 들어가면서 경막과 붙어 있고 경막의 결손이 관찰되었으며 주위에 육아조직이 있었다(Fig. 4).
PPPP
단락술후 발생한 긴장성 기뇌증
J Korean Neurosurg Soc/Volume 30/January, 2001 82
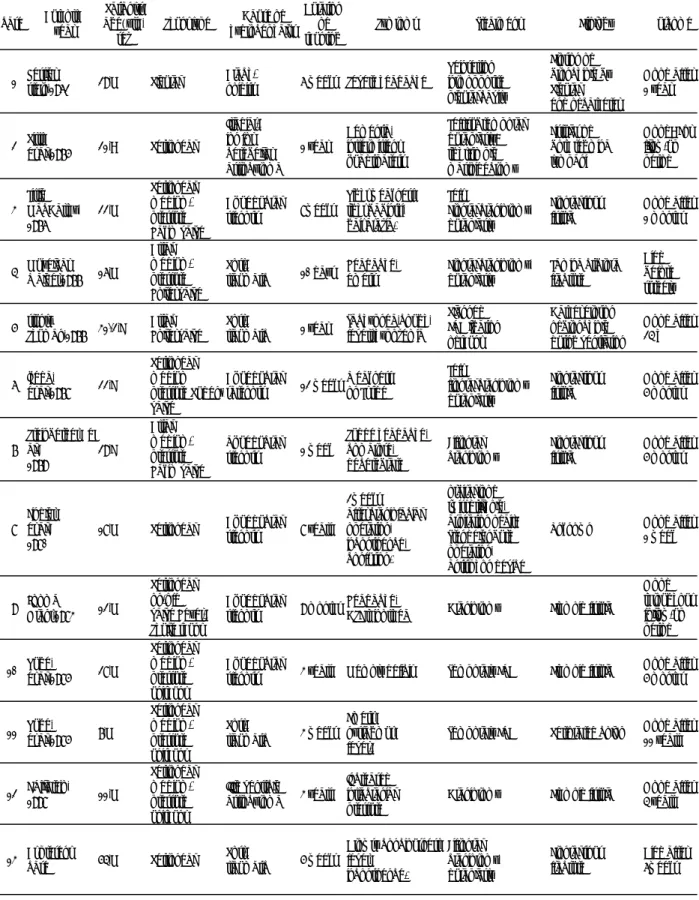
Table 1. Reported cases of shunt associated pneumocephalus case Authors,
year
Patiant’s age(yrs), sex
Shunt type Cause of hydrocephalus
Duration of shunting
Symtoms Treatment Etiology Outcome
1 Kessler &
stern,1962 29,M Pleural Arach-
noiditis 6 weeks Severe headache
Reinsertion into opposite pleural cavity
Erosion of bronchiole by Pleural end of catheter
Good after 1 year
2 Pitts,
et al.,1975 21,? Peritoneal Irradiat- ion for cerebellar astrocytoma
1 year
Dementia, inttermittent quadriparesis
Left:subtemporal duraplasty:
right:simple mastoidectomy
Fistulas of both tegmina tympani
Good? For fllow-up period
3 Little &
MacCarthy, 1976
22,M
Peritoneal, medium- pressure Hakim valve
Aqueductal
stenosis 8weeks
Right weakness, right babinski, gait ataxia.
Left
Frontal craniotomy, duraplasty
Frontal sinus fistula
Good after 1 months
4 Muizelaar &
Walder,1977 16,M
Atrial, medium- pressure Holter valve
Post-
traumatic 10 days Headache, emesis
Frontal craniotomy, duraplasty
Lamina cribrosa fracture
Died before surgery 5 stuntz &
Shuman,1977 31/2,F Atrial, Holter valve
Post-
traumatic 1 year Tachypnea,cough, fevers,hypoxemia
Planned EVD ligation of shunt
Cather erosion of bronchiole during ventilation
Good after 24 h
6 Ikeda,
et al.,1978 22,F
Peritoneal medium pressure Pudenz valve
Aqueductal
satenosis 12 weeks Weakness on Lt side
Left
frontal craniotomy duraplasty
Frontal sinus fistula
Good after 5 months
7
Steinberger, et al.,
1979
29,F
Atrial, medium- pressure Hakim valve
aqueductal
stenosis 1 week
Sudde headache, comatose, decerebrate
Bifrontal craniotomy
Frontal sinus fistula
Good after 5 months
8 Findler, et al.,
1980 18,M Peritoneal Aqueductal
stenosis 8 years 2weeks after craniofacial operation, incontinence, confusion.
orbital roof twist drill,hole, aspiration of air;
Trendelenburg operation, antisiphon device
Unknown Good after 1 week
9 Jooma &
Grant,1983 12,M
Peritoneal on-off valve Heyer- Shulte shunt
Aqueductal
stenosis 9 months Headache,
CSF rhinorrhea Craniotomy Ethmoid fistula Good throughout follow-up period 10 Ruge,
et al.,1985 28,M
Peritoneal medium- pressure unishunt
Aqueductal
stenosis 3 years Memory deficit Temporary EVD Ethmoid fistula Good after 5 months
11 Ruge,
et al.,1985 7,M
Peritoneal medium- pressure unishunt
Post-
traumatic 3 weeks Emesis, nystagmus, fever.
Temporary EVD Perforated colon Good after 11 years
12 F.Villarejo,
1998 11,M
Peritoneal medium- pressure unishunt
IIIrd ventricle
astrocytoma 3 years
Increased intracranial pressure
Craniotomy Ethmoid fistula Good after 4 years
13 At present
case 54,M Peritoneal Post-
traumatic 5 weeks Drowsy conciousness, fever,
incontinence.
Bifrontal craniotomy, duraplasty
Frontal sinus fracture
Died after 6weeks
이재학·김범태·조성진·신원한·최순관·변박장
J Korean Neurosurg Soc/Volume 30/January, 2001 83
경막의 결손부위를 골막을 이용하여 봉합하고 전두동을 막 았다. 전두엽의 공기가 있는 부분에 공기배액을 위한 배액 관을 삽입하고 수술을 마쳤다. 술 후 환자는 뇌실염과 동반 된 패혈증으로 사망하였다.
고 찰
대부분의 기뇌증은 부비동이나 유양돌기동을 경유하는 뇌기저부 골절에 의해 발생한다. 그 밖의 다른 원인으로는 뇌기저골이나 부비동의 종양, 뇌기저골의 골수염, 그리고 선천적인 뇌기저골의 결손이다. 또한 기뇌증으로 인한 종 괴효과와 감염등으로 인한 중증의 정도가 이환율, 사망률 과 관계가있다. 단락술후 기뇌증이 발생하는 경우는 매우 드문 것으로 현재까지 문헌고찰상 12례가 보고되고 있으 며 그 중 1례가 사망하였다1)2). 단락술후 발생한 기뇌증은 단락관을 통하거나, 외상, 수술후 발생한 결손, 선천적으로 존재했던 단락부위, 그리고 뇌기저골의 얇은 부위를 통하 여 발생한다. 원위부 단락관을 통해 공기가 두개강내로 들 어가는 경우는 단락관이 피부를 뚫거나 세기관지나 대장을 뚫고 들어가는 경우이다4)7).
단락술후 두개강내압의 변화는 단락관의 사이폰 작용(si- phon effect)에 의해 발생 되며 기립위에서 정상 뇌척수액
Fig. 1. Brain CT scan taken at admission. Computed tomogra- phy revealing the fractured left frontal sinus and hyper- density on the right temporal lobe.
Fig. 3. CT scan shows the air in a porecephalic cavity of the right frontal lobe, which commiunicated with frontal si- nus, and left temporal lobe and basal cisterns.
Fig. 4. Intraoperative photography indicating the dura defect (arrow).
Fig. 2. Brain CT scan showing the ventricular enlargement and periventricular low-density and porencephalic cavity of the right temporal lobe.
434343 43
46 46 46 46
44 4444 44
4545 4545
단락술후 발생한 긴장성 기뇌증
J Korean Neurosurg Soc/Volume 30/January, 2001 84
압은 -30~155mmH2O이며, 단락술을 시행한 환자에서 몬 로공(foramen of Monro) 부위에서 압력은 -440mmH2O 가 된다9). 또한 뇌척수액은 단락이나 대뇌바닥(cranial fl- oor)을 통해 배액되게 된다. 이렇게 생긴 음압과 뇌척수액 의 배액은 공기가 두개강내를 채우게 하며, 뇌조직이나 경 막에 의한 ball-valve 현상에 의해 뇌척수액 유출없이 두 개강내에 고립되게 된다1)2). 본 증례의 환자는 수상당시 전 두동을 포함한 전두골의 함몰성 분쇄골절이 있었으나 염증 과 육아조직으로 자연치유 되었다가, 수두증의 치료로 실 시한 단락술로 인해 두개강내 음압이 발생되면서, 전두동 골절부위의 자연치유 되었던 경막 결손 부위로 공기가 유 입된 것으로 사료되었다. 이런 두부외상 환자의 단락술을 시행할 때 기뇌증의 발생과 함께 이는 치명적일 수 있음을 충분히 염두에 두어야 할 것이다.
또한, 중뇌수도협착(aqueductal stenosis) 환자에서 단 락술후 기뇌증이 발생할 수 있는 것으로 알려져 있는데 이 는 만성적인 두개강내압항진으로 두개기저골에 골미란이 일어나기 때문이다. 제치기나 운동등의 적은사고에도 악화된 뇌척수액 경계(thinned cerebrospinal fluid barrier)가 쉽 게 파괴된다1)8).
선천적으로 두개저의 결손이 있던 경우에도 만성적으로 상승된 뇌압에 의해 이 결손부위를 통해 기뇌증이 발생할 수 있다. 뇌허니아(encephaloceles)의 약 5%가 뇌기저골 에 발생하고 이 결손부위를 통해 기뇌증이 발생할 수 있으 며2), 대부분이 중두개와(middle cranial fossa)에 발생한다.
중이(middle ear cavity)의 고실개(tegmen tympani)6)나 접형동의 외측 확장부위10) 등도 원인이 될 수 있다. Åhren and Thulin3)의 조사에 의한면 고실개의 약 21%에서 결손 이 관찰되었고, Elwany5)의 조사에서 접형동의 외측 확장부 위는 16%에서 관찰되었다. 단락술에 의해 변화된 뇌척수 액의 역동학과 압력의 변화는 이런 선천적인 결손부위를 통해 기뇌증이 발생할 수 있다.
중수도협착 등 만성적으로 상승된 두개강내압 환자나 부 비동이나 유양돌기를 포함하는 두개골절이 있던 환자에서 선천적으로 존재한 두개골 결손부위나 육아조직에 의해 자 연치유되었던 부위에서 단락술에 의해 변화된 두개강내압 의 변화는 얘기치 못한 합병증을 유발할 수 있음을 충분히 고려하여야 하겠다.
결 론
저자들은 외상 후 단락이 형성되었다가 자연 치유된 후
단락술후 발생한 긴장성 기뇌증으로 사망한 사례를 치험하 였으며 이런 두부외상 환자의 단락술을 시행할때는 기뇌증 의 발생과 함께 치명적일 수 있음을 충분히 염두에 두어야 할 것이다.
•논문접수일:2000년 4월 10일
•심사완료일:2000년 7월 18일
•책임저자:김 범 태
420-853 경기도 부천시 원미구 중동 1174 순천향대학교 의과대학 부천병원 신경외과학교실 전화:032) 621-5289, 전송:032) 621-5018 E-mail:[email protected]
References
1) Ruge JR, Cerullo LJ, McLone DG:Pneumocephalus in pa- tients with CSF shunts. J Neurosurg 63:532-536, 1985 2) Villarejo F, Cerceller F, Alvarez C, et al:Pneumocephalus
after shunting for hydrocephalus. Child’s Nerv Syst 14:
333-337, 1998
3) Åhren C, Thulin CA:Lethal intracranial complications foll- owing inflation in the external auditory canal in treatment of serous otitis media and due to defects in the petrous bone. Acta Otolaryng 60:407-421, 1965
4) Arico M, beluffi G, Fiori P, et al:Rectal extrusion of the catheter and air ventriculography following bowel perfora- tion in ventriculo-peritoneal shunt. Pediatr Radiol 15:53- 55, 1985
5) Elwany S. Yacout YM, Talaat ME, et al:Surgical anatomy of the sphenoid sinus. J Laryngol Otol 97:227-241, 1983 6) Goffin J, Plets C:Tension pneumocephalus in association
with ventriculoperitoneal shunt. Acta Neurochirurgica 76: 121-124, 1985
7) Karibe H, Ishibashi Y:A case of sigmoid colon perforation by a V-P shunt tube resulting in pneumocephalus. No Shinkei Geka 26:79-82, 1998
8) Little JR, MacCarty CS:Tension pneumocephalus after ins- ertion of ventriculoperitoneal shunt for aqueductal stenosis: case report. J Neurosurg 44:383-385, 1976
9) McCullough DC, Fox JL:Negative intracranial pressure hy- drocephalus in adults with shunts and its relationship to the production of subdural hematoma. J Neurosurg 40:372-375, 1974
10) Morley TP, Wortzman G:The importance of the lateral ex- tensions of the sphenoid sinus in post-traumatic cerebrospinal rhinorrhea and meningitis. J Neurosurg 22:326-332, 1965