Abstract : Backgrounds : Warfarin, an oral anticoagulant, has narrow therapeutic range. Bleeding risk can rise dramatically in patients with supratherapeutic international normalized ratio (INR).
There are various guidelines for correcting excessive anticoagulation. One of these is the 9th ACCP guideline. It suggests simply holding warfarin in non-bleeding patients with INR value of 4.5 to 10.0.
Therefore, we evaluated the treatment methods for INR control at Seoul National University Hospital (SNUH).
Methods : Patients with INR value of 4.5 to 10.0 without evidence of bleeding who were followed at an anticoagulation clinic in SNUH from September 2012 to August 2014 were included in this study.
They were observed retrospectively based on medical records and anticoagulation clinic sheets.
Patients were divided into two groups: 1) short-term warfarin withdrawal group, and 2) vitamin K1
group. We evaluated the incidence of INR over-correction, bleeding, and thromboembolic events in each group.
Results : Most patients with 4.5 ≤ INR 6.0 were treated by temporarily holding warfarin. Finally,
와파린 복용 중 과도한 INR 상승 시 비출혈 환자에서 비타민 K1 사용의 후향적 평가
서비취, 문정연,�조은정, 조윤숙, 한현주 서울대학교병원 약제부
A Retrospective Evaluation of Vitamin K
1Therapy for Managing Supratherapeutic International Normalized Ratio in Non-Bleeding
Patients Treated with Warfarin
Bi Chwi Seo, Jung Yeon Moon,�Eun Jeong Jo, Yoon Sook Cho and Hyeon Joo Hahn
Department of Pharmacy, Seoul National University Hospital, 101 Daehak-ro, Jongno-gu, Seoul, 110-744, Korea
투고일자 2016.5.12; 심사완료일자 2016.6.23; 게재확정일자 2016.9.22
�교신저자 문정연 Tel:02-2072-2594 E-mail:[email protected]
Original Article
a total of 30 cases with INR value of 6.0 to 10.0 were analyzed, including 13 cases treated by tem- porarily holding warfarin and 17 cases treated by vitamin K1. INR over-correction was more frequent in the vitamin K1group (11 cases (64.7%) in the vitamin K1group vs. 1 case (7.7%) in the temporary warfarin withdrawal group, p=0.002). We found no significant difference in bleeding rate between the two treatment groups (minor bleeding in 1 case (7.7%) in the temporary warfarin withdrawal group and 1 case (5.9%) in the vitamin K1group, p=0.687). There was no thromboembolic event or major bleeding in either group.
Conclusion : Considering the risk of thromboembolism by INR over-correction, temporary warfarin withdrawal may be more appropriate than using vitamin K1for non-bleeding patients with supratherapeutic INR without indications of acute reversal of excessive anticoagulation.
[Key words] Warfarin, Supratherapeutic INR, Vitamin K1
경구용 항응고제인 warfarin은 vitamin K epoxide reductase (VKOR)를 억제하여 vitamin K depend- ent coagulation factors Ⅱ, Ⅶ, Ⅸ, Ⅹ의 활성화를 감소시켜 항응고 효과가 나타나는 약물로 심부정맥혈 전증, 심방세동, 급성심근경색, 판막질환 환자 및 인공 심장판막치환술을 받은 환자의 전신적인 색전증을 예 방하기 위해 사용되고 있다.1)Warfarin의 항응고 효과 는 약물상호작용, 식이, 질병상태 등 다양한 요인에 의 하여 변할 수 있으므로 warfarin의 치료 효과를 유지 하면서 주요 합병증인 출혈을 예방하기 위하여 정기적 으로 INR (International normalized ratio)을 모니 터링하고 이에 따른 warfarin의 용량 조절이 이루어 져야 한다.
국내에서는 항응고 요법의 구체적인 치료지침이 확 립되어 있지 않아 대부분의 의료기관에서 ACCP (American College of Chest Physicians) 치료지침 을 기준으로 하고 있으며 해당 지침에서는 warfarin을 복용하는 대부분 환자들의 적정치료 범위로 INR 2.0~3.0을 권고하고 있다.1),2)
Palareti G. 등의 연구3)에 따르면 warfarin을 복용 하는 환자의 출혈빈도는 fatal bleeding 0.25%, major bleeding 1.1%, minor bleeding 7.6%로 보고
되었고 INR 4.5 이상일 때 bleeding risk가 더 높았 다. Warfarin 복용 중 과도한 항응고 효과가 발생했을 때는 warfarin을 감량 또는 단기간 복용 중단하고 추 가적으로 vitamin K1과 혈액제제인 fresh frozen plasma (FFP), prothrombin complex concentra- tion (PCC)을 사용하는 적극적인 치료 방법도 있어 환 자의 출혈 여부와 그 유형, INR 상승치를 고려하여 적 절한 치료 방법을 선택해야 한다.4)2012년도 ACCP 치 료지침에 따르면 INR 4.5-10.0이고 출혈이 없는 환자 는 Warfarin의 복용을 단기적으로 중단하도록 하고 INR 10.0 초과 시 vitamin K1경구제제를 투여하도록 권고하고 있다.5)
서울대학교병원에 critical-value reporting sys- tem이 도입된 후 치료범위 이상으로 INR이 상승된 항 응고상담실(AntiCoagulation Service, ACS) 환자를 진료과에 연결하는 INR 상승 기준이 기존 INR 10.0에 서 일반외과 INR 5.0, 그 외 진료과는 INR 6.0으로 낮 추어 변경되었다. 이 후 INR이 치료범위 이상으로 과 도하게 상승되었어도 출혈 증상이 없어 INR의 즉각적 인 교정이 요구되지 않는 환자에서 vitamin K1의 처방 빈도가 증가하는 경향을 보이고 있다. 따라서 본 연구 에서는 서울대학교병원 ACS상담실에서 관리하는 환
자 중 과도한 INR 상승 시 출혈이 없는 환자들을 대상 으로 vitamin K1 투여 후 INR over-correction 발생 률을 조사하고 warfarin 단기 복용 중단과 vitamin K1투여 후 출혈 예방 효과의 차이를 비교하여 안전하 고 효과적인 치료법을 확인하고자 하였다.
연구방법 1. 연구대상
2012년 9월부터 2014년 8월까지 총 24개월 동안 서 울대학교병원 ACS에 등록된 환자 중에서 INR 4.5- 10.0이고 출혈이 없는 환자를 대상으로 후향적 연구를 진행하였다. Warfarin 복용기간이 3개월 미만인 환 자, 18세 미만 환자, warfarin 복약순응도가 떨어지는 환자, 심각한 간질환, 신기능, 갑상선 기능 이상 환자,6) 관찰 기간 중 warfarin과 약물 상호작용을 일으킬 수 있는 약제의 변화, 식이의 변화, 과다한 음주, 한약이 나 건강보조식품의 복용 등 INR 유지와 출혈 발생에 영향을 주는 요인이 있는 환자는 연구 대상에서 제외 하였다.
2. 연구방법
대상 환자의 항응고 상담기록 및 전자의무기록지 (electronic medical record)를 통해 환자의 연령, 성 별, warfarin 적응증, 과도한 INR 상승 시 수치, 치료 후 INR 및 clinical event 발생 여부를 조사하였다. 수 집한 자료들은 warfarin을 단기간 복용 중단하는 환자 군과 vitamin K1을 투여한 환자군으로 나누어 평가하 였다.
본 연구에서는 치료 후 1차 PT (prothrombin time) 검사 결과가 INR 1.5 미만인 경우를 INR over-cor- rection으로 정의하였고7),8)두 군간 INR over-cor- rection 발생률의 차이를 비교하였다. 또한 각 치료의 출혈 예방 효과 차이를 평가하기 위하여 치료 후 30일 이내에 발생한 출혈 증상과 혈전색전증 발생 여부를 조 사하였고9) 출혈의 유형은 major bleeding과 minor bleeding으로 분류하였다. Major bleeding은 두개내 출혈, 척수내 출혈, 안구 출혈, 후복막 출혈, 관절강내
출혈, 심막 출혈 및 헤모글로빈 20 g/L 이상 감소되는 출혈, 2 unit 이상의 수혈이 필요한 출혈 등 생명을 위 협하는 출혈이 나타난 경우이며 minor bleeding은 major bleeding에 해당하지 않는 출혈로 멍이 증가한 경우, 잇몸 출혈, 코피, 미세혈뇨 등을 포함하여 의학적 인 개입이 필요한 경우로 정의하였다.10) 각 치료 후 warfarin 용량조절에 대한 영향을 평가하기 위하여 측 정오차를 고려한 target INR (INR range: 1.8-3.2)이 연속 2회 이상 유지된 시점까지 시행한 ACS follow up 횟수와 치료 후 INR over-correction이 나타난 환 자를 대상으로 INR 1.5 이상으로 회복될 때까지 시행 한 ACS follow up 횟수를 조사하였다.
본 연구의 통계분석은 SPSS (Statistical Package for the Social Sciences) version 22.0을 사용하였고 모든 통계분석의 결과는 5% 미만(p<0.05)일 때 통계적 으로 유의하다고 정의하였다. 두 군간 INR over-cor- rection 발생률, clinical event 발생률의 차이는 Chi- square test (Fisher’s exact test)를 이용하여 분석하 였고 치료 후 target INR 도달 시점과 INR over- correction을 벗어나는 시점까지의 ACS follow up 횟 수는 Mann-Whitney test로 분석하였다.
3. 피험자 보호
본 연구는 서울대학교병원 의학연구윤리심의위원회 (Institutional Review Board, IRB)로부터 승인(IRB No. H-1409-062-609)받았으며, 후향적 연구이므로 피험자의 동의는 생략하였다.
연구 결과
연구기간 내 INR 4.5 이상 5.0 미만 236건 전체 (100%)와 INR 5.0 이상 6.0 미만 242건 중 232건 (95.9%)은 과도한 항응고 효과에 대한 치료로 단기적 으로 warfarin의 복용을 중단하였다. 그러나 INR 6.0-10.0에 해당하는 113건 중 46건(40.7%)에서 vitamin K1이 투여되어 과잉 치료되는 경향을 보였고 critical-value reporting system 시행 후 해당 INR 수치의 환자에서 vitamin K1의 사용이 증가함을 확인 하였다(Table 1). 따라서 본 연구는 ACS 등록환자 중
치료범위 이상으로 INR 상승 시 의료진에 연결하는 ACS 상담실 기준과 2012 ACCP 치료지침을 고려하여 초기 연구대상 중 과잉치료가 우려되는 INR 6.0-10.0 인 환자를 대상으로 치료 후 INR over-correction 발 생률과 clinical event 발생률과 유형을 조사하였다.
이와는 별도로 각 치료 후 ACS follow up 횟수는 INR 5.0-10.0인 환자를 대상으로 검토하였다.
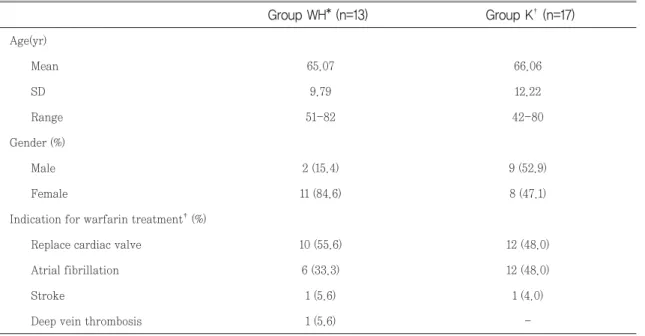
1. 대상환자의 특성
본 연구는 INR 6.0-10.0에 해당하는 113건 중 83건 을 제외한 30건을 연구대상으로 하였다. 이 중 war- farin을 단기 복용 중단한 치료는 13건, vitamin K1을 투여한 치료는 17건으로 두 군간 연령, 성별은 유의한 차이가 없었다(P=0.057, P=0.706). Warfarin의 적응 증은 두 군 모두 인공심장 판막치환술과 심방세동이 가
*Temporary warfarin withdrawal group; �Vitamin K1group
4.5~4.99 118 0
5.0~ 5.99 120 2
6.0~10.0 45 4
4.5~4.99 118 0
5.0~ 5.99 112 8
6.0~10.0 22 42
Group K�
INR Group WH*
Table 1. The number of cases in two treatment groups
Before starting critical-value reporting system (from September, 2012 to August, 2013;12monthes)
After starting critical-value reporting system (from September, 2013 to August, 2014;12monthes)
*Temporary warfarin withdrawal group; �Vitamin K1group
�There are patients that have more than two warfarin indications
Age(yr)
Mean 65.07 66.06
SD 9.79 12.22
Range 51-82 42-80
Gender (%)
Male 2 (15.4) 9 (52.9)
Female 11 (84.6) 8 (47.1)
Indication for warfarin treatment�(%)
Replace cardiac valve 10 (55.6) 12 (48.0)
Atrial fibrillation 6 (33.3) 12 (48.0)
Stroke 1 (5.6) 1 (4.0)
Deep vein thrombosis 1 (5.6) -
Group K�(n=17) Group WH* (n=13)
Table 2. Characteristics of study patients
장 많았다(Table 2).
2. INR over-correction 발생률
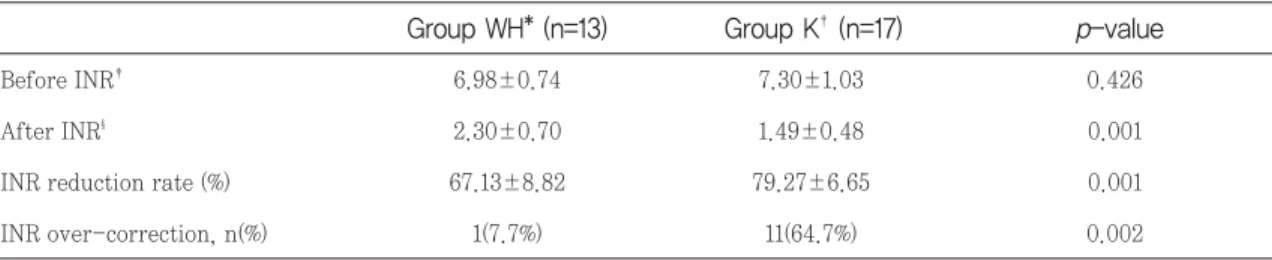
INR 6.0-10.0에 해당하는 환자의 치료 전후 INR 수 치 변화를 확인하기 위해 INR 감소율을 비교하였다.
치료 전 INR은 두 군에서 차이가 없었으나(6.98±
0.74 vs 7.30±1.03, P=0.426), 치료 후 INR은 war- farin 단기 중단군보다 vitamin K1투여군에서 유의하 게 낮게 나타나 높은 INR 감소율을 보였다(67.13±
8.82 vs 79.27±6.65, P=0.001)(Table 3).
또한 INR over-correction은 warfarin 단기 중단 군 13건 중 1건, vitamin K1투여군 17건 중 11건에서 발생하여 warfarin 단기 중단군보다 vitamin K1투여 군에서 INR over-correction 발생률이 유의하게 높 았다(7.7% vs 64.7%, P=0.002)(Table 3).
3. Clinical event 발생 여부 및 유형
INR 6.0-10.0에 해당하는 환자의 각 치료 후 발생한
출혈 합병증을 조사하였을 때 warfarin 단기 중단군 13건 중 1건, vitamin K1투여군 17건 중 1건에서 출혈 이 발생하였다. 출혈의 유형은 잇몸출혈과 멍으로 모두 minor bleeding에 해당하고 두 군간 출혈 발생률은 통계학적으로 유의한 차이가 없었다(7.7% vs 5.9%, P=0.687). 관찰기간 내 major bleeding과 혈전색전증 은 두 군 모두 발생하지 않았다(Table 4).
4. ACS follow up 횟수
INR 6.0-10.0에 해당하는 환자 중 warfarin 단기 중단군의 INR over-correction은 1건이 관찰되어 본 연구의 ACS follow up 횟수는 INR 5.0-10.0인 환자 를 대상으로 조사하였다. INR 5.0-10.0에 해당하는 355건 중 259건을 제외한 96건을 대상으로 하였을 때 warfarin 단기 중단 76건 중 9건(11.8%), vitamin K1
투여 20건 중 14건(70%)에서 INR over-correction이 발생하였다.
따라서 각 군에서 INR over-correction 발생 후 INR이 1.5 이상 회복될 때까지 시행한 ACS follow up
*Temporary warfarin withdrawal group; �Vitamin K1group
�Before INR: INR values before management of excessive warfarin anticoagulation
§After INR: INR values after management of excessive warfarin anticoagulation
Before INR� 6.98±0.74 7.30±1.03 0.426
After INR§ 2.30±0.70 1.49±0.48 0.001
INR reduction rate (%) 67.13±8.82 79.27±6.65 0.001
INR over-correction, n(%) 1(7.7%) 11(64.7%) 0.002
p-value Group K�(n=17)
Group WH* (n=13)
Table 3. Comparison of INR reduction rate, INR over-correction incidence between group WH and group K
*Temporary warfarin withdrawal group; �Vitamin K1group
Bleeding event, n(%) 1 (7.7%) 1 (5.9%) 0.687
Type Gingival bleeding Bruise, gingival bleeding
Thromboembolic event, n(%) - - -
p-value Group K�(n=17)
Group WH* (n=13) Table 4. Types and frequencies of clinical event
횟수를 조사한 결과, warfarin 단기 중단군은 9건 모 두 1회차 ACS상담 시 INR이 회복되었지만 vitamin K1투여군은 1회차 9건(64.29%), 2회차 3건(21.43%), 3회차 2건(14.28%) 순으로 조사되었다(Fig. 1).
또한 치료 후 target INR (INR range: 1.8-3.2)이 연속 2회 이상 유지된 시점까지 시행된 ACS follow up 횟수는 warfarin 단기 중단군과 vitamin K1투여 군 각 중위수 값이 3.21회, 4.41회로 vitamin K1투여 군이 더 높았으며, 각 군의 범위는 3~5회, 3~9회 이었 다(Fig. 2).
결론 및 고찰
경구용 항응고제인 warfarin은 치료 범위가 좁은 약 물로 과용량 복용, 음주, 약물상호작용, vitamin K1의
식이량 감소, 급성 질환의 동반 등 다양한 요인으로 인 해 과도한 항응고 효과가 나타날 수 있다.11)본 연구는 2012 ACCP guideline에 근거하여 2012년 9월부터 2014년 8월까지 서울대학교병원 ACS 등록환자 중 INR 4.5-10.0이고 출혈이 없는 환자를 대상으로 INR 을 치료범위로 낮추기 위하여 warfarin 복용을 단기 중단한 환자와 vitamin K1을 투여한 환자로 나누어 안 전하고 효과적인 치료법을 확인하고자 하였다.
현재 국내에서 시판되는 vitamin K1 주사제제는 S.C. (subcutaneous), I.M. (intramuscular), I.V.
(intravenous)로 투여될 수 있다. Vitamin K1의 S.C.
투여는 warfarin 단기 중단 치료와 비교 시 24시간 내 INR 감소율이 유사하고7)I.M. 투여는 혈종이 발생할 가능성이 있다.12)Watson HG. 등의 연구13)에서 vita- min K1을 I.V.로 투여했을 때 P.O. (per oral) 투여보 Fig. 1 The number of ACS follow-up until reaching INR above 1.5 after INR over-correction
*Temporary warfarin withdrawal group; �Vitamin K1group
Fig. 2 The number of ACS follow-up to target INR
*Temporary warfarin withdrawal group; �Vitamin K1group
다 INR 감소 속도가 더 빨랐지만 투여 24시간 후 INR 감소율은 투여방법에 따른 차이가 없어 anaphylaxis 가 발생할 수 있는 I.V. 보다 P.O.로 vitamin K1을 투 여할 것을 권장하고 있다.14) 그러나 현재 국내에서는 vitamin K1경구제제가 생산되지 않기 때문에 INR의 빠른 교정이 요구되는 응급상황 시 vitamin K1주사제 제를 사용하고 있으며 본 연구에서는 모두 I.V. 경로로 투여되었다.
본 연구에서 INR over-correction 발생률은 war- farin 단기 중단군보다 vitamin K1투여군에서 더 높 게 나타났고 통계적으로 유의적인 차이를 보였다(7.7%
vs 64.7%, P=0.002). Patel RJ. 등의 연구15)에서도 vitamin K12.5 mg와 placebo를 경구투여 후 INR을 측정하였을 때 vitamin K1경구투여군에서 INR<1.5인 patient-days가 유의하게 많았다(0(0%) vs 10(5%), P=0.009). Rose AJ. 등의 연구8)에서는 INR 수치가 1.5 미만일 경우 혈전색전증의 위험이 INR 2.0 이상인 경우보다 약 16배 높다고 보고하고 있고 과잉치료 후 다시 항응고 치료를 할 때 warfarin resistance가 발 생하여 치료 실패를 야기할 수 있으므로 warfarin을 복용하는 환자에서 vitamin K1의 투여는 주의가 필요 하다.
치료 후 출혈발생률은 warfarin 단기 중단군이 7.7%, vitamin K1투여군이 5.9% 로 통계적으로 두 군 사이의 유의적인 차이가 없었으며 출혈발생 건은 두 군 모두 1건으로 낮은 발생빈도를 보였다. 따라서 두 치료법은 모두 INR을 낮추어 출혈을 예방하는데 효과 가 있는 것으로 사료된다. INR 4.5-10.0이고 출혈이 없는 환자를 대상으로 진행한 Crowther M.A. 등의 연 구16)에서도 vitamin K11.25 mg를 경구 투여 했을 때 placebo와 비교 시 출혈 예방 효과는 차이가 없었다 (15.8% vs 16.3%, P= 0.86).
이번 연구에서 vitamin K1 투여 후 혈전색전증과 warfarin resistance는 관찰되지 않았다. 그러나 INR 5.0-10.0이면서 출혈이 없는 환자를 대상으로 각 치료 법에 따라 target INR 도달 할 때까지 수행된 ACS follow up 횟수와 INR over-correction 후 INR 수치 가 1.5 이상 회복될 때까지 수행된 ACS follow up 횟 수를 조사한 결과, 두 경우 모두 vitamin K1투여군의 ACS follow up 횟수가 더 많은 경향을 보였다. 이를
통해 vitamin K1투여 후 다시 치료범위의 INR 수치 에 도달하기 위하여 warfarin의 용량을 조절하는데 어 려움이 있음을 알 수 있었다.
본 연구는 대상환자의 수가 제한적이고 항응고 상담 기록 및 전자의무기록지를 통해 후향적(retrospective) 조사 방법으로 진행되어 INR의 재측정 시기가 다양해 일정한 시간 후의 치료효과를 비교할 수 없었고 치료 후 시간 경과에 따른 INR 감소 추이를 확인할 수 없었 다는 점 등에서 한계를 보인다. 이를 보완하기 위하여 일정한 조건 하에서 전향적인 방법으로 연구를 진행한 다면 보다 적절한 치료지침을 확립할 수 있을 것이다.
그러나 이번 연구는 해당 환자에서 과도한 항응고 효 과에 대한 치료로 warfarin 단기 중단과 vitamin K1
투여 시 INR over-correction 발생률, 출혈여부, ACS follow up 횟수를 비교, 평가하여 안전하고 효과 적인 치료법을 확인하였다는데 의의가 있다.
위 연구의 결과들을 종합하였을 때, 과도한 항응고 효 과의 치료로 vitamin K1의 투여는 INR over-cor- rection이 나타나 혈전색전증이 발생할 위험이 있고 warfarin resistance로 인한 항응고 치료 실패를 야기 할 수 있으므로 INR 4.5-10.0이면서 출혈이 없는 환 자의 치료로 vitamin K1을 투여하는 것보다 warfarin 을 단기 중단하는 것이 더 적절할 것으로 사료된다.
참고문헌
1) Hirsh J., James E., Anderson D. R. et al.
Oral anticoagulants: mechanism of action, clinical effectiveness, and optimal therapeu- tic range. Chest 2001; 119: 8S-21S.
2) Dentali F., Ageno W., Crowther M. et al.
Treatment of coumarin-associated coagu- lopathy: a systematic review and proposed treatment algorithms. J Thromb Haemost.
2006; 4: 1853-63.
3) Palareti G., Leali N., Coccheri S. et al.
Bleeding complications of oral anticoagulant treatment: an inception-cohort, prospective collaborative study (ISCOAT). Lancet. 1996;
348:423-28.
4) Ansell J., Hirsh J., Hylek E., Jacobson A., Crowther M., Palareti G. Pharmacology and Management of the vitamin K antagonist, American College of Chest Practice Guidelines (9th Edition). Chest 2008;
133:160-198.
5) Holbrook A., Schulman S., Daniel M. et al.
Antithrombotic therapy and prevention of thrombosis, American College of Chest, Physicians Evidence-Based Clinical Practice Guidelines (9th Edition). Chest 2012;
141(2_suppl): e152s-e184s.
6) Demirkan K., Stephens M.A., Newman K.P., Self T.H. Response to warfarin and other oral anticoagulants: effects of disease states.
South Med J. 2000; 93(5):448-54.
7) DeZee K.D., Shimeall W.T., Douglas K.M., Shumway N.M., O’Malley P.G. Treatment of excessive anticoagulation with phytonadione (vitamin K). Arch Intern Med. 2006; 166:391- 397.
8) Rose A.J., Ozonoff A., Grant R.W., Henault L.E., Hyleck E.M. Epidemiology of subthera- peutic anticoagulation in the United States.
Circ Cardiovasc Qual Outcomes. 2009;
2:591-597.
9) Denas G., Marzot F., Offelli P. et al.
Effectiveness and safety of a management protocol to correct over-anticoagulation with oral vitamin K: a retrospective study of 1043 cases. J Thromb Trombolysis. 2009;
27:340-347.
10) International Society on Thrombosis and Haemostasis, Inc., Available from: http://
www. isth.org (Accessed on August 2014).
11) Jeon H.Y., Shin K.Y., Kim E.Y., An H.Y., Chang H.I., Sohn K.H. Evaluationn of the management of excessive warfarin antico- agulation. J. Kor. Soc. Health-Syst. Pharm.
2009; 26:66-77.
12) American Hospital Formulary Service (AHFS).2008; 3658-3660.
13) Watson H.G., Baglin T., Laidlaw S.L., Makris M., Preston F.E. A comparison of the efficacy and rate of response to oral and intravenous vitamin K in reversal of over- anticoagulation with warfarin. Br J Haematol. 2001;115: 145-149.
14) Fiore LD, Scola MA, Cantillon CE, Brophy MT. Anaphylactoid reactions to vitamin. J Thromb Trombolysis. 2001;11:175-183.
15) Patel R.J., Witt D.M., Saseen J.J., Tillman DJ, Wilkinson D.S. Randomized, placebo- controlled trial of oral phytonadione for excessive anticoagulation. Pharmacotherapy.
2000; 20(10):1159-1166.
16) Crowther M.A., Ageno W., Garcia D. et al.
Oral vitamin K Versus Placebo to Correct Excessive Anticoagulation In Patients Receiving Warfarin, Ann Intern Med, 150, 293-300 (200:9).