ABSTRACT
Background : Generally speaking, the condition of dyslipidemia is a major risk factor for the devel- opment of an ischemic stroke. The domestic and international stroke guidelines recommend that physicians follow the 2004 NCEP-ATP III and 2013 ACC/AHA dyslipidemia treatment guidelines when using statins for the prevention of an ischemic stroke. However, the role of statin therapy in the patients with acute cerebral infarction has not been established, and is generally prescribed under clinical judgment. The purpose of this study was to evaluate the status and appropriateness of the statin treatment for patients with an acute cerebral infarction in the emergency department.
Methods : In this study, we analyzed 430 patients who were diagnosed with an ischemic stroke at
급성기 뇌경색 환자에서 Staitn 처방과 임상결과 지표 분석
구희원
a, 서성연
a, 김귀숙
a, 조윤숙
a, 정근화
b,�, 이주연
c,�서울대학교병원 약제부
a, 서울대학교병원 신경과
b, 서울대학교 약학대학
cPatterns of Statin Treatments During Acute Stroke Period and Clinical Outcomes in Patients with Ischemic Stroke
Heewon Ku
a, Sungyun Suh
a, Kwi suk Kim
a, Yoonsook Cho
a, Keunhwa Jung
b,�and Ju-Yeun Lee
c,�Department of Pharmacy, Seoul National University Hospital 101 Daehak-ro, Jongno-gu, Seoul 03080, Republic of Korea
aDepartment of Neurology, Seoul National University Hospital 101 Daehak-ro, Jongno-gu, Seoul 03080, Republic of Korea
bCollege of Pharmacy, Seoul National University 103 Daehak-ro, Jongno-gu, Seoul 03080, Republic of Korea
c투고일자 2017.7.31; 심사완료일자 2017.9.20; 게재확정일자 2018.3.8
�교신저자 정근화 Tel:02-2072-4901 E-mail:[email protected] 공동교신 이주연 Tel:02-3668-7472 E-mail:[email protected]
Original Article
연구배경 및 목적
뇌졸중은 우리나라뿐 아니라 전세계적으로 가장 중 요한 사망원인이며, 성인에서 장애의 가장 중요한 원인 질환이다. 국내의 뇌졸중 발생은 노령층 인구의 증가와 더불어 2030년에는 현재 보다 3배 가까이 증가한 연간 35만 건에 이를 것으로 예측된다.
1)뇌졸중 급성기 치료 및 뇌졸중 위험인자 조절 향상으로 국내에서 뇌졸중으 로 인한 연간 사망이 21세기 첫 10년동안 약 28.3% 감 소하였다. 그러나 아직도 뇌졸중은 주요 사망원인이며, 2010년 통계청 사망통계에 의하면 약 26,500명이 뇌 졸중으로 사망하였으며(인구 10만명 당 53.2명) 20분 마다 1명이 뇌졸중으로 사망하고 있다.
2)허혈성 뇌졸중, 특히 죽상경화성 뇌졸중은 고지질혈
증이 중요한 위험 요인으로 작용하며, 이는 여러 statin 관련 임상연구를 통해 밝혀졌다.
3),4)Statin은 콜 레스테롤 저하 작용 뿐 아니라 다양한 세포보호 기전을 갖는다는 연구 결과가 있다.
5)최근 결과가 발표된 SPARCL(Stroke Prevention by Aggressive Reduction in Cholesterol Levels Study) 연구는
3)저 밀도 콜레스테롤(LDL cholesterol)이 100-190 mg/dL인 뇌졸중 혹은 일과성허혈발작(transient ischemic attack) 환자 4,731명을 대상으로 atorvas- tatin을 하루 80 mg 투여한 무작위 대조군 연구로서, 대조군에 비해 치료군에서 5년 뇌졸중의 발생률이 16%(위험비, 0.84) 감소되는 효과를 확인하였다. 국내 권고사항에는 허혈성 뇌졸중의 경우, 고지질혈증은 반 드시 교정되어야 하며, 죽상경화성 동맥질환에 의한 허 the Seoul National University Hospital from July 2013 to May 2015. We retrospectively analyzed the prescription pattern of statin therapy for the first 72 hours and 3 months, after the admission due to an ischemic stroke with a review of the patient electronic medical records. We also evaluated the effects of statin use during an acute phase of ischemic stroke on the patient clinical outcomes.
Results : Among the 430 patients who participated in the study, there were 314 patients (73.0%) who received a statin within 72 hours after admission, and 246 patients (78.3%) who were prescribed with moderate intensity statins. The predictors of statin therapy within 72 hours after hospital admission were patients who had received previous statin use (aOR 7.38, 95% CI 3.77-14.44), LDL 100 mg/dL on admission (aOR 8.98, 95% CI 4.99-16.19), and who had experienced large artery atherosclerosis (aOR 2.92, 95% CI 1.64-5.22) type by TOAST classification. In addition, the high-intensity statin was less prescribed in a stroke of cardioembolism (aOR 0.33, 95% CI 0.12-0.90), and a small vessel occlu- sion (aOR 0.28, 95% CI 0.11-0.70), as compared with a large artery atherosclerosis. The compliance with the 2013 ACC/AHA guideline on the treatment of hyperlipidemia was 34.1% in this case. The use of statin within 72 hours after admission did not affect each clinical outcome, which included early neurological deterioration for 7 days, mRS 2 at 3 months and a recurrent ischemic stroke within 3 months after admission.
Conclusion : The main factors influencing the prescription status and clinical outcome were a pre- vious medication, LDL level, and the pathogenesis of a stroke. The effect of the statin on the clinical outcome in an acute cerebral infarction should be confirmed by a prospective study of stroke patients with the same pathogenesis.
[Key words] Statin, Acute stroke period, Ischemic stroke, Intensity of statin, TOAST classification
혈성 뇌졸중이나 관상동맥질환을 동반한 허혈성 뇌졸 중 환자의 고지질혈증 치료기준은 National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Cholesterol in Adults (Adult Treatment Panel III, 이하 NCEP-ATP III)의 기준을 따르도록 되어 있다.
6)또한 관상동맥질환을 동반하거나 증후성 죽상경화성 허혈성 뇌졸중 환자의 콜레스테롤 교정 목표는 저밀도 콜레스테롤을 기준으로 하여 100 mg/dL 이하이다.
6), 7)이러한 뇌졸중의 일차 및 이차 예방에 대한 statin의 국내 권고사항은 나와있지만, 급성기 뇌경색에서의 statin 사용에 관한 권고사항은 없다. 하지만 statin이 저밀도 지질 단백질 수치를 낮출 뿐만 아니라, 혈관내 막 기능, 뇌혈관 혈류, 염증 등을 포함한 급성기 신경보 호 효과가 밝혀지면서, 2013년 AHA/ASA Guideline for the Early Management of Patients With Acute Ischemic Stroke에서는 허혈성 뇌졸중 발생 이전부터 statin을 복용하고 있었다면, 급성기 동안 계 속 statin을 사용하는 것이 합리적이라고 권고한다.
8)또한, 코호트 연구로 Dublin의 북쪽지방 주민을 대상 으로 한 statin의 급성기 뇌경색 예후 효과에 관한 연구
9)
에서 뇌경색 발생 전 및 발생 후 72시간 이내에 statin 복용과 modified Rankin Score (mRS) 및 생존율을 분석하였다. 결과적으로 뇌경색 발생 후 72시간 이내의 statin 복용이 statin을 투여하지 않은 환자군과 비교 시 생존율을 높이는 것으로 분석 되었으며 뇌경색 발생 전 복용도 유사한 결과를 보였다.
하지만 급성기 뇌졸중에서 statin의 종류 및 용량에 대한 근거는 확립되지 않은 상태이며, 급성기에서 statin을 사용해야 하는지에 대한 권고사항 조차 국내 에는 마련되어 있지 않다. 따라서, 국내 급성기 뇌경색 치료에서 statin 사용 현황을 평가하고, statin의 예후 효과를 확인하는 추가적 연구가 필요하다. 본 연구에서 는 증상 발생 7일 이내 서울대학교병원을 방문한 19세 이상의 급성기 뇌경색 환자를 대상으로 statin 처방현 황을 파악하고 뇌졸중 후 예후와의 상관성을 평가하고 자 하였다.
연구방법
1. 연구대상 및 연구기간
2013년 7월부터 2015년 5월까지 서울대학교병원 신 경과에서 허혈성 뇌졸중을 진단 받은 환자 중 만 19세 이상의 성인으로 증상 발생 7일 이내 입원한 환자를 대 상으로 후향적 연구를 진행하였다. 과거 허혈성 뇌졸중 의 병력 및 statin의 복용력이 불확실한 환자, 서울대 학교병원 신경과 입원일 이후 3개월 이내 외래기록이 미비한 환자는 연구 대상에서 제외하였다. 본 연구는 서울대학교병원 생명윤리심의위원회의 승인 하에 진행 되었다.(IRB 심의번호: 1605-022-760).
2. 연구 도구 및 자료 수집 방법
전자의무기록을 통해 환자의 인구정보학적 특징, 기
저질환, 10년 죽상경화질환 위험도(10-year ASCVD
risk), 허혈성 뇌졸중 발병기전, 뇌동맥의 협착정도
(stenosis of relevant artery), 입원 전과 후 statin
종류 및 용량, 약물 중단 시점 및 재개시점, 입원 후 3
개월 까지의 재발률, 약물 관련 부작용 발생, 신경과 전
문의가 평가한 입원 후 7일 동안의 신경학적 악화여부,
발병 3개월째의 mRS를 후향적으로 수집하였다. 대상
환자의 모든 statin 처방패턴을 분석하였으며, 입원 후
72시간 안에 statin을 처방 받은 군과 처방 받지 않은
군으로 분류하였다. 아형에 따른 허혈성 뇌졸중의 분류
로는 Trial of Org 10172 in Acute Stroke Treatment
(TOAST) 분류에 따라 Large artery atherosclero-
sis(LAA)군, Small vessel occlusion(SVO)군,
Cardioembolism(CE), Undetermined(UD) 및
Other determined(OD)로 구분하였다. 사용된 statin
의 강도는 2013 ACC/AHA Blood cholesterol
guideline
7)에 제시된 기준으로 평균 고강도, 중간강도,
저강도로 평가하였다. 임상현장에서의 급성기 뇌경색
환자에게의 statin 처방 현황 파악을 위하여 2013
ACC/AHA Blood cholesterol guideline과의 일치도
를 평가하였다. 임상결과 지표 분석에서 일차 지표는 7
일 동안의 신경학적 악화 여부(early neurological
deterioration, 입원 후 7일 이내 National Institute
of Health Stroke Scale (NIHSS) 점수 1점 이상 상
승)와 3개월째 mRS 점수 2점 초과 여부로 정의하였으
며, 이차 지표는 입원 후 3개월 이내 뇌졸중 재발 여부 로 정의하였다.
3. 통계분석 방법
환자의 특성이나 처방패턴은 기술적 통계를 이용하 여 비율로 표시하였으며, statin 처방 여부와 임상결과 지표에 영향을 미치는 요인 분석은 로지스틱 회귀분석 을 이용하였다. 모든 통계적 분석은 IBM SPSS stat- ics version 22.0을 이용하였다.
연구결과
1. 환자 특성
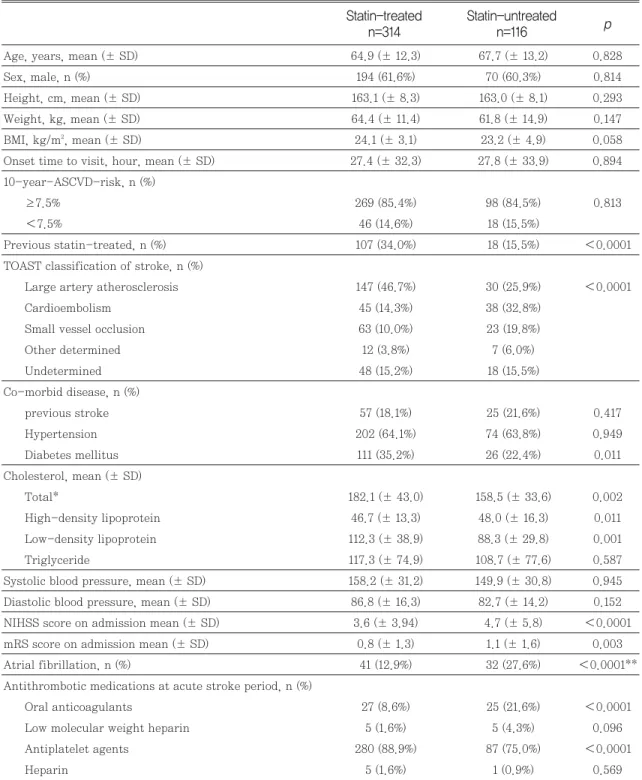
연구기간 동안 선정기준을 만족하는 환자는 430명이 었다. 입원 후 72시간 안에 statin을 처방 받은 군은 받 지 않은 군에 비해 총콜레스테롤(total cholesterol, TC)(p=0.002)과 저밀도지단백 콜레스테롤(LDL-C) 농도가 유의하게 높았다(p=0.001)(Table 1). 또한 statin을 처방 받은 군이 당뇨병을 기저질환으로 갖고 있는 비율이 더 높았다(p=0.011; Table 1). 반면, EKG 및 24시간 홀터검사에서 심방세동이 있는 환자의 비율 은 statin을 처방 받지 않은 군에서 더 높았다 p 0.0001; Table 1). 입원 시 NIHSS(p 0.0001) 및 mRS 점수(p=0.003)도 statin을 처방 받지 않은 군에 서 더 높았다(Table 1).
2. Statin 처방패턴 분석 및 처방에 영향을 주는 요인 분석
전체 환자 중 입원 후 72시간 안에 statin을 투여 받 은 환자는 314명(73.0%)이었다. 입원 후 가장 많이 처 방된 강도의 statin은 중간강도(78.3%; 246/314명)였 으며, 이 중 가장 많이 처방된 statin은 10 mg ator- vastatin(43.9%; 138/314명)과 20mg atorvas- tatin(23.9%; 75/314명)이었다. 입원 후 72시간 이내 statin 처방에 영향을 주는 로지스틱 회귀 분석 결과, 다변량 분석에서는 입원 전 statin 사용력(aOR 7.38, 95% CI 3.77-14.44)과 입원 시 LDL-C 수치가 100 초과(aOR 8.98, 95% CI 4.99-16.19)인 변수가 statin
처방 빈도를 높이는 것으로 나타났고 TOAST 분류에 서 다른 기전 모두와 비교하였을 때 LAA 기전으로 발 병 시 statin 처방 빈도가 높은 것으로 확인되었다 (Table 2).
입원 후 72시간 안에 고강도 statin 처방에 영향을 주 는 요인에 대한 로지스틱 회귀분석 결과, 단변량 분석 에서 유일하게 TOAST 분류에 따라 CE, SVO 기전 대 비 LAA 기전으로 발병했을 시에만 고강도 statin 처방 빈도를 높이는 것으로 나타났다(Table 2).
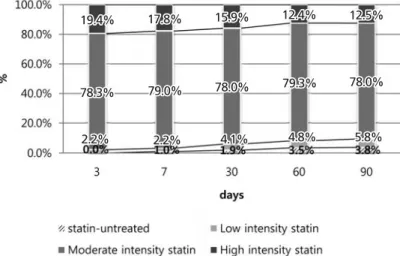
입원 후 72시간 이내 statin을 처방 받은 군에서는, 입원 후 7일, 30일, 60일, 90일이 지날 수록 고강도 statin 사용빈도는 감소하였고, 저강도 statin 및 statin 중단 빈도는 점점 증가하였다. 반면 가장 사용 량이 많았던 중간강도 statin의 사용 빈도는 비슷하게 유지되었다(Fig 1). 입원 후 72시간 이내 statin을 처방 받지 않은 군에서는, 입원 후 7일째 중간강도 statin의 처방 빈도가 크게 증가하였고 30일, 60일, 90일 지날 수록 더 상승하였다. 반면 고강도 statin의 처방빈도는 7일 이후 비슷하게 유지되었고 저강도 statin을 처방 받은 환자는 없었다(Fig 2).
3. 초기 statin 사용이 임상결과에 미치는 영향
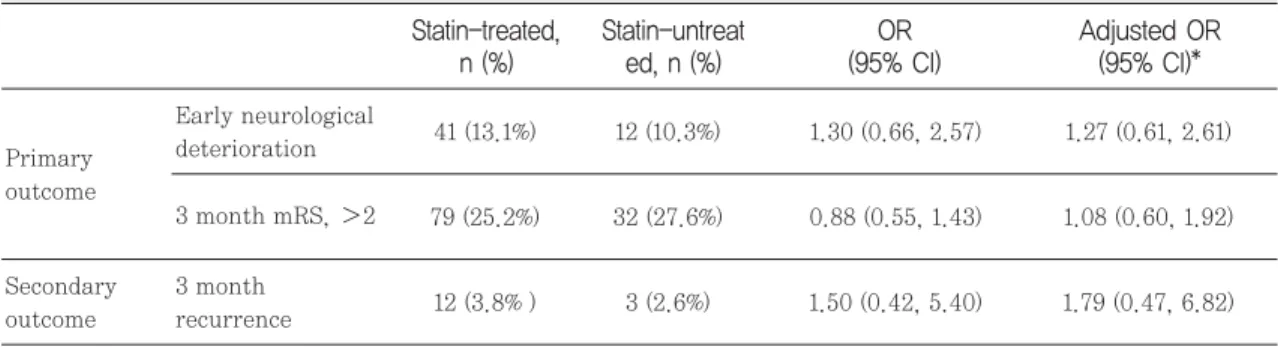
입원 후 72시간 안에 statin을 처방 받은 군과 받지 않은 군을 비교 했을 때, 나이, 입원 시 NIHSS, TOAST 분류 및 이전 뇌졸중 기왕력으로 보정한 다변 량 로지스틱 회귀분석 결과, 7일 동안의 신경학적 악화 (early neurological deterioration, END)여부와 3개 월째 mRS 점수가 2점 초과인 여부 그리고 입원 후 3 개월 이내 뇌졸중의 재발여부에 통계적으로 유의한 영 향을 미치지 않는 것으로 분석되었다(Table 3).
전체 환자 중 LAA 기전으로 발병한 환자는 176명
(40.9%)이었으며, 이들 중 입원 후 72시간 안에 statin
을 처방 받은 환자는 146명(82.9%), 처방 받지 않은 환
자는 30명(17.1%)이었다. 입원 후 72시간 안에 고강도
statin를 사용한 환자가 40명(22.7%), 중간강도
statin을 사용한 환자가 106명(60.2%)이었고 저강도
statin은 처방되지 않았다. 또한 LAA 기전으로 발병
한 군에서 입원 후 72시간 안에 statin의 처방 여부가
임상결과 지표에 미치는 영향은 통계적으로 유의하지
Statin-untreated p n=116 Statin-treated
n=314
Table 1 Baseline characteristics according to statin exposure within 72 hours after admission
Age, years, mean (± SD) 64.9 (± 12.3) 67.7 (± 13.2) 0.828
Sex, male, n (%) 194 (61.6%) 70 (60.3%) 0.814
Height, cm, mean (± SD) 163.1 (± 8.3) 163.0 (± 8.1) 0.293
Weight, kg, mean (± SD) 64.4 (± 11.4) 61.8 (± 14.9) 0.147
BMI, kg/m2, mean (± SD) 24.1 (± 3.1) 23.2 (± 4.9) 0.058
Onset time to visit, hour, mean (± SD) 27.4 (± 32.3) 27.8 (± 33.9) 0.894 10-year-ASCVD-risk, n (%)
≥7.5% 269 (85.4%) 98 (84.5%) 0.813
7.5% 46 (14.6%) 18 (15.5%)
Previous statin-treated, n (%) 107 (34.0%) 18 (15.5%) 0.0001
TOAST classification of stroke, n (%)
Large artery atherosclerosis 147 (46.7%) 30 (25.9%) 0.0001
Cardioembolism 45 (14.3%) 38 (32.8%)
Small vessel occlusion 63 (10.0%) 23 (19.8%)
Other determined 12 (3.8%) 7 (6.0%)
Undetermined 48 (15.2%) 18 (15.5%)
Co-morbid disease, n (%)
previous stroke 57 (18.1%) 25 (21.6%) 0.417
Hypertension 202 (64.1%) 74 (63.8%) 0.949
Diabetes mellitus 111 (35.2%) 26 (22.4%) 0.011
Cholesterol, mean (± SD)
Total* 182.1 (± 43.0) 158.5 (± 33.6) 0.002
High-density lipoprotein 46.7 (± 13.3) 48.0 (± 16.3) 0.011
Low-density lipoprotein 112.3 (± 38.9) 88.3 (± 29.8) 0.001
Triglyceride 117.3 (± 74.9) 108.7 (± 77.6) 0.587
Systolic blood pressure, mean (± SD) 158.2 (± 31.2) 149.9 (± 30.8) 0.945 Diastolic blood pressure, mean (± SD) 86.8 (± 16.3) 82.7 (± 14.2) 0.152
NIHSS score on admission mean (± SD) 3.6 (± 3.94) 4.7 (± 5.8) 0.0001
mRS score on admission mean (± SD) 0.8 (± 1.3) 1.1 (± 1.6) 0.003
Atrial fibrillation, n (%) 41 (12.9%) 32 (27.6%) 0.0001**
Antithrombotic medications at acute stroke period, n (%)
Oral anticoagulants 27 (8.6%) 25 (21.6%) 0.0001
Low molecular weight heparin 5 (1.6%) 5 (4.3%) 0.096
Antiplatelet agents 280 (88.9%) 87 (75.0%) 0.0001
Heparin 5 (1.6%) 1 (0.9%) 0.569
BMI Body Mass Index; TOAST Trial of Org 10172 in Acute Stroke Treatment; NIHSS National Institute of Health Stroke Scale; mRS modified Rankin score;
SD standard deviation
않은 것으로 분석되었다.
반면, 입원 후 72시간 안에 처방된 statin 강도에 따 른 임상결과 지표에 미치는 영향 분석에서는 중등강도 statin 사용군과 비교 시 고강도 statin을 사용하였을 때 END가 나타난 빈도가 더 높았던 것으로 분석되었 다(aOR 6.92, 95% CI 1.46-32.73, Table 4).
4. 임상결과에 영향을 주는 요인 분석
1) 7일동안의 신경학적 악화에 영향을 주는 인자
END는 입원 후 72시간 안에 statin을 처방 받은 군 에서 41명(13.1%)에서 나타났고, 처방 받지 않은 군에 서 12명(10.3%)에서 나타났다(p=0.523, Table 3).
Fig. 1 Changing pattern of statin intensity for 3months in patients who received statins within 72 hours after admission
Fig. 2 Changing pattern of statin intensity for 3 months in patients who didn’ t receive statins within 72
hours after admission
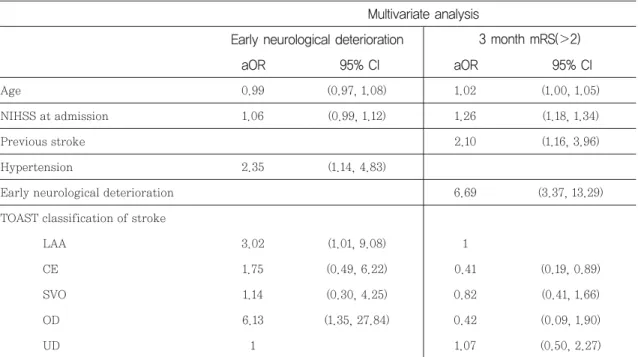
END에 영향을 주는 요인으로는, 로지스틱 회귀분석 결과 다변량 분석 시 TOAST 분류에서 UD 대비 LAA (aOR 3.02, 95% CI 1.01-9.08)및 OD 기전(aOR
6.13, 95% CI 1.35-27.84)에서 END의 빈도를 높이는 것으로 나타났다. 또한 TOAST 분류, 나이, 입원 시 NIHSS 로 보정한 다변량 분석 결과, 기저로 고혈압이
95% CI aOR
95% CI aOR
High intensity statins Univariate analysis statins
Multivariate analysis
Table 2 Predictors for prescribing statins and high intensity statins within 72 hours after admission
Age, 75yr 0.58 (0.27, 1.25)
Previous statin 7.38 (3.77, 14.44) 1.14 (0.63, 2.31)
Admission NIHSS 0.95 (0.90, 1.00) 0.95 (0.88, 1.03)
Previous stroke 0.99 (0.48, 2.05)
Diabetes mellitus 1.61 (0.91, 2.87) 1.24 (0.70, 2.20)
Heart disease 0.9 (0.43, 2.03) 0.78 (0.37, 1.64)
Baseline LDL, 100mg/dl 8.98 (4.99, 16.19) 1.29 (0.72, 2.34)
10-yr ASCVD risk, ≥7.5% 0.99 (0.45, 2.18)
TOAST classification of stroke
LAA 1 1
CE 0.35 (0.14, 0.86) 0.33 (0.122, 0.90)
SVO 0.33 (0.16, 0.67) 0.28 (0.112, 0.70)
OD 0.27 (0.08, 0.85) 0.88 (0.228, 3.43)
UD 0.39 (0.18, 0.85) 0.45 (0.188, 1.09)
OR Odds ratio; 95% CI 95% Confidence Interval; NIHSS National Institute of Health Stroke Scale ; LDL low density lipoprotein; ASCVD Atherosclerotic cardiovascular disease; LAA large artery atherosclerosis; CE cardioembolism; SVO small vessel occlusion; OD other determinded; UD undeterminded
* Asjusted by age, NIHSS at admission, TOAST classification and previous stroke.
Adjusted OR (95% CI)*
OR (95% CI) Statin-untreat
ed, n (%) Statin-treated,
n (%)
Table 3 Association between primary or secondary outcome and statin therapy within 72 hours after admis- sion with ischemic stroke
41 (13.1%) 12 (10.3%) 1.30 (0.66, 2.57) 1.27 (0.61, 2.61)
79 (25.2%) 32 (27.6%) 0.88 (0.55, 1.43) 1.08 (0.60, 1.92)
12 (3.8% ) 3 (2.6%) 1.50 (0.42, 5.40) 1.79 (0.47, 6.82) Primary
outcome
Secondary outcome
Early neurological deterioration 3 month mRS, 2
3 month recurrence
있을수록 END의 빈도를 높이는 것으로 나타났다(OR 2.35, 95% CI 1.14-4.83, Table 5).
2) 입원 후 3개월째 mRS 점수가 2점 초과여부에 영향 을 미치는 요인
3개월째 mRS 점수가 2점 초과인 환자는, 입원 후 72 시간 안에 statin을 처방 받은 군에서 79명(25.2%) 그 리고 처방 받지 않은 군에서 32명(27.6%) 이었다 (p=0.81, Table 3). 이 지표에 영향을 주는 로지스틱 회귀분석 결과 다변량 분석 시 TOAST 분류에서 LAA
*Adjusted by age, NIHSS at admission, previous hypertension, previous stroke and stenosis of the relevant artery.
Adjusted OR (95% CI)*
OR (95% CI) Moderate inten-
sity statin, n (%) High intensity
Statin, n (%)
Table 4 Association between primary or secondary outcome and statin therapy within 72 hours after admis- sion with large artery atherosclerotic stroke
12 (30.0%) 13 (12.3%) 3.07 (1.26, 7.47) 6.92 (1.46, 32.73)
15 (37.5%) 26 (36.7%) 1.85 (0.85, 4.02) 3.02 (0.85, 10.75)
2 (3.4%) 4 (3.3%) 1.81 (0.30, 11.24) 0.52 (0.03, 8.39) Primary
outcome
Secondary outcome
Early neurological deterioration 3 month mRS, 2
3 month reccurence
95% CI aOR
95% CI aOR
3 month mRS( 2) Multivariate analysis
Early neurological deterioration
Table 5 Multivariate logistic regression analyses for factors associated with the early neurological deteriora- tion and 3 month mRS( 2)
Age 0.99 (0.97, 1.08) 1.02 (1.00, 1.05)
NIHSS at admission 1.06 (0.99, 1.12) 1.26 (1.18, 1.34)
Previous stroke 2.10 (1.16, 3.96)
Hypertension 2.35 (1.14, 4.83)
Early neurological deterioration 6.69 (3.37, 13.29)
TOAST classification of stroke
LAA 3.02 (1.01, 9.08) 1
CE 1.75 (0.49, 6.22) 0.41 (0.19, 0.89)
SVO 1.14 (0.30, 4.25) 0.82 (0.41, 1.66)
OD 6.13 (1.35, 27.84) 0.42 (0.09, 1.90)
UD 1 1.07 (0.50, 2.27)
OR Odds ratio; 95% CI 95% Confidence Interval; NIHSS National Institute of Health Stroke Scale; LAA large artery atherosclerosis; CE cardioembolism;
SVO small vesslel occlusion; OD other determined; UD undetermined
로 발병 시 CE와 비교하였을 때, 3개월째 mRS 2점 초 과인 빈도를 높이는 것으로 나타났다(Table 5).
3) 2013 ACC/AHA cholesterol guideline 일치도 평가
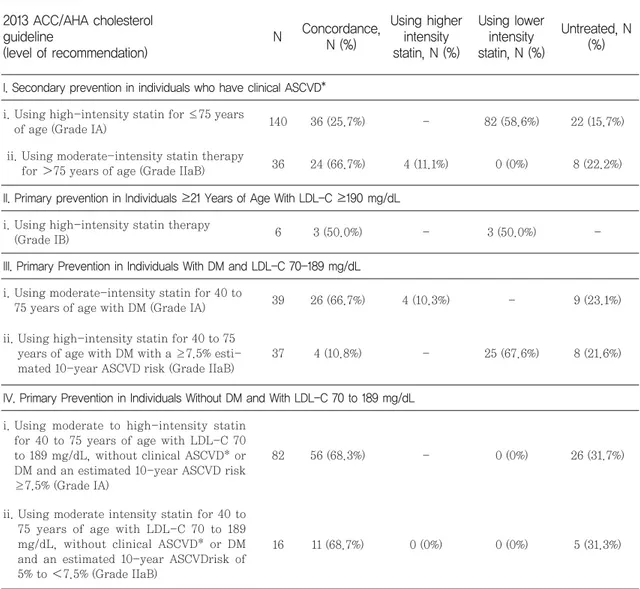
입원 후 72시간 이내 statin 처방 현황에서 2013 ACC/AHA cholesterol guideline을 어느 정도 순응 하고 있는지를 평가하였다. 이 때, 죽상경화로 인해 주 요 뇌동맥(major brain artery) 혹은 가지 대뇌 피질 동맥(branch cortical artery)에 폐색(혹은 중증 협착) 이 발생하는 대동맥죽상경화 기전의 뇌졸중만 임상적 인 ASCVD 군에 포함하여 2차 예방 기준으로 평가하 였다. 이러한 2차 예방 기준으로 75세 이하에서는 고 강도 statin이 grade IA로 권고되지만 실제로 대상 140명 중 36명(25.7%)만이 순응하였고 82명(58.6%) 이 중간강도 혹은 저강도 statin을 사용하였다(Table 6). 1차 예방 기준으로 평가하였을 때, 입원 시 LDL-C 가 190 mg/dL 이상이며 21세 이상인 대상 환자 6명 중 3명(50.0%)이 고강도 statin을 사용하라는 권고사 항(Grade IB)을 준수하였고, LDL-C 수치가 70-189 mg/dL 사이며 당뇨병을 함께 갖고 10년 죽상경화질환 위험도가 7.5% 이상인 45-75세 대상환자 37명 중 4 명(10.8%)만이 고강도 statin을 사용하라는 권고사항 (Grade IIaB)을 준수하였다(Table 6).
입원 후 72시간 안에 statin을 사용한 군에서 전체적 으로 2013 ACC/AHA guideline을 순응한 환자는 147 명(46.8%)이 고강도 권고사항 및 중간강도 권고사항보 다 낮은 강도의 statin을 사용한 환자는 156명(49.7%) 이였다. 또한 75세 초과인 노인에서 고강도 statin을 사용한 환자는 9명(2.9%)였고 나머지 2명(0.6%)은 위 험과 이익을 판단하여 statin을 처방할 것이 권고되고 있었다.
입원 후 72시간 안에 statin을 사용하지 않은 군에서 는 112명(96.5%)이 statin 사용 권고 대상 이었지만 순 응하지 않았다. 나머지 4명(3.4%)은 위험과 이익을 판 단하여 statin을 처방할 것이 권고되고 있었다.
고찰
Statin이 급성 심근경색과 심혈관계 질환의 위험성을
낮춘다는 것은 잘 알려져 있지만, 상대적으로 뇌 조직 과 뇌졸중 후 예후에서 statin의 잠재적 이점은 연구가 부족하다.
10)국내외 뇌졸중 진료지침에서 2차 예방목적 으로의 statin 사용은 높은 수준으로 권고되고 있지만, 급성기 뇌경색에서의 statin의 역할에 대해서는 언급이 제한적이다. 다만, 이전에 statin을 복용하고 있었다면 급성기에 복용을 중단할 시 기능적 결과(mRS 점수 2; 60.0% vs 39.0%; p=0.043), END(65.2% vs 20.9%; p 0.0001), 경색 부피(infarct volume)(74 [45, 126] vs 26 [12, 70] mL; p=0.002)가 나빠지므로 계속 유지할 것이 추천되고 있다.
11)본 연구는 허혈성 뇌졸중으로 신경과에 입원한 환자 중, 증상 발생 7일 이내 입원한 환자 430명을 대상으로 입원 후 statin 처방에 영향을 미치는 요인, 입원 후 72 시간 이내 statin 사용 여부에 따른 임상결과지표에 미 치는 영향 그리고 2013 ACC/AHA cholesterol guideline과의 일치도를 평가하였다. 본 연구 결과 입 원 후 72시간 내 statin 투여에 영향을 미치는 인자로 는 입원 전 statin 복용력, 입원시 LDL-C 100 mg/dL 초과, TOAST 분류상 LAA 기전 일 때 처방 빈도가 높 았음이 확인되었다(Table 2). 이는 허혈성 뇌졸중 발병 전 statin을 복용하고 있었다면 급성기 동안 복용을 지 속하라는 권고사항
8)과 증후성 죽상경화성 허혈성 뇌졸 중 환자에서 LDL 목표수치를 100mg/dL 이하로 하라 는 권고사항
12)을 잘 이행하고 있다고 평가할 수 있다.
임상적으로 뇌졸중 환자에서 예후에 가장 중요한 인자 는 발병 기전이며, 실제 항혈소판, 항응고요법 등의 약 물치료는 발병 기전에 따라 다르게 계획된다. 본 연구 결과, LAA 기전으로 발병 시 다른 기전에 비해 중상동 맥경화의 부담이 가장 크다고 판단되기 때문에 statin 처방과 고강도 statin 사용이 더 많다고 분석되었다.
실제로 최근 LAA 기전으로 발병한 급성기 뇌경색 환
자를 대상으로 한 연구에서 입원 전 statin 사용이 좋
은 기능적 결과(mRS 점수 0-1; OR 2.44; 95% CI
1.07-5.53), 낮은 1개월 사망률 (HR; 0.24; 95% CI
0.08-0.75), 낮은 뇌졸중 재발(HR 0.11; 95% CI
0.02-0.46)을 보인다고 밝혀졌다.
13)하지만 본 연구에
서 임상결과지표 분석 시 입원 후 72시간 안에 statin
사용 여부가 END, 3개월째 mRS 점수가 2 초과인 여
부, 3달 이내 뇌졸중 재발에 유의한 영향을 미치지 않
는 것으로 분석되었고(Table 3), LAA군만 세부분석 하였을 때는 고강도 statin 사용하였을 때 오히려 END의 비율이 높게 나타나는 것으로 분석되었다 (Table 4). 원인으로는 실제 임상에서 statin을 사용시 동맥경화 위험도가 심할수록 고강도 statin을 사용하 였기 때문에 진행이 관찰되었다고 해석할 수 있다. 통
계분석 시, 죽상동맥경화 부담을 평가할 수 있는 다양 한 지표인 죽상경화반 안정성, 측부 순환정도 등이 보 정되지 않은 혼동될 수 있는 인자로 남아있으므로 추후 이러한 인자들을 바탕으로 추가적인 연구가 필요할 것 으로 사료된다. 본 연구에서 END의 위험인자로 기저 로 고혈압을 갖는 경우, TOAST 기전상 UD와 비교 시
IV. Primary Prevention in Individuals Without DM and With LDL-C 70 to 189 mg/dL82 56 (68.3%) - 0 (0%) 26 (31.7%)
16 11 (68.7%) 0 (0%) 0 (0%) 5 (31.3%)
i. Using moderate to high-intensity statin for 40 to 75 years of age with LDL-C 70 to 189 mg/dL, without clinical ASCVD* or DM and an estimated 10-year ASCVD risk
≥7.5% (Grade IA)
ii. Using moderate intensity statin for 40 to 75 years of age with LDL-C 70 to 189 mg/dL, without clinical ASCVD* or DM and an estimated 10-year ASCVDrisk of 5% to 7.5% (Grade IIaB)
Untreated, N (%) Using lower
intensity statin, N (%) Using higher
intensity statin, N (%) Concordance,
N (%) N
2013 ACC/AHA cholesterol guideline
(level of recommendation)
I. Secondary prevention in individuals who have clinical ASCVD*
Table 6 Concordance rate of prescribing statin within 72hr after admission with 2013 ACC/AHA cholesterol guideline
140 36 (25.7%) - 82 (58.6%) 22 (15.7%)
36 24 (66.7%) 4 (11.1%) 0 (0%) 8 (22.2%)
i. Using high-intensity statin for ≤75 years of age (Grade IA)
ii. Using moderate-intensity statin therapy for 75 years of age (Grade IIaB)
III. Primary Prevention in Individuals With DM and LDL-C 70-189 mg/dL
39 26 (66.7%) 4 (10.3%) - 9 (23.1%)
37 4 (10.8%) - 25 (67.6%) 8 (21.6%)
i. Using moderate-intensity statin for 40 to 75 years of age with DM (Grade IA) ii. Using high-intensity statin for 40 to 75
years of age with DM with a ≥7.5% esti- mated 10-year ASCVD risk (Grade IIaB)
II. Primary prevention in Individuals ≥21 Years of Age With LDL-C ≥190 mg/dL
6 3 (50.0%) - 3 (50.0%) -
i. Using high-intensity statin therapy (Grade IB)
*Clinical ASCVD included only stroke with mechanism of large artery atherosclerosis. ACC/AHA American College of Cardiology/American hearth
Association; ASCVD Atherosclerotic cardiovascular disease; LDL-C low density lipoprotein cholesterol; DM Diabetes Mellitus
LAA, OD로 발병한 경우가 유의한 요인으로 분석되었 고, 3개월째 mRS 점수가 2점 초과인 여부의 위험인자 로는 나이, 입원시 NIHSS 점수, stroke 기왕력, END 여부, TOAST 기전상 CE와 비교시 LAA로 발병한 경 우가 유의한 요인으로 분석되었다(Table 5). 이는 기존 의 연구와 일치하는 결과로 END를 예측할 수 있는 인 자로는 입원 시 중증도, 당뇨병 기왕력, 입원 시 혈압, 대동맥 협착 등이 알려져 있다.
14)3개월째 mRS 점수가 2점 초과인 여부 또한 유사하게 입원 시 중증도, 나이, END 여부 등이 영향을 미치는 것으로 알려져 있다.
15)2013 ACC/AHA 고지질혈증 치료 가이드라인에서는 임상적 ASCVD 를 갖고 있을 시 이차 예방으로 나이 75세 이하에서 고강도 statin 사용이 권고되고 있다.
본 연구 결과 LAA 기전 발생군을 임상적 ASCVD 군 으로 놓고 평가하였을 때 25.7%만 이 권고사항을 순 응 하는 것으로 확인되었다. 58.6%는 중간강도 및 저 강도 statin을 사용하였고 15.7%는 statin을 사용하 지 않았다.
그 외에 기저질환으로 당뇨를 갖고 있으며 입원시 LDL 수치가 70-189 mg/dL인 환자에서 나이가 40- 75세이고 10년 죽상경화질환 위험도가 7.5% 이상일 시 고강도 statin을 사용하라 권고되지만, 10.8%만이 순 응하는 것으로 분석되었다. 고강도 statin 사용에 대한 가이드라인 일치율이 낮은 이유로는 뇌혈관 질환에서 고강도 statin의 명확한 이점이 잘 밝혀지지 않은 이유 가 있으며,
10)동양인은 서양인과 비교하여 적은 체중과 유전적 다양성 때문에 적은 용량으로도 동일한 지질저 하작용을 가지므로
16)임상의가 statin을 처방할 때 이러 한 점들을 고려하기 때문으로 보인다. 또한 가이드라인 상 2차, 1차 예방으로 statin 사용시 사용시작 시점 및 사용기간에 대한 언급이 없으므로 이에 대한 부분 또한 임상의의 판단에 따라 다르게 사용되고 있다. 최근 ASSORT 연구에서 급성기 뇌경색에서 초기 statin 치 료가 후기 치료에 비해 유의한 이점이 없다고 한 발표 가 있었으므로 치료 시작 시점에 대한 논의는 더 필요 할 것으로 보인다.
18)본 연구결과 대체로 급성기 뇌경색 으로 입원한 후 7일 이내 statin 투약을 시작하며, 대다 수가 중간 강도 statin을 사용하고 시간이 지날수록 강 도가 낮아지고 중단하는 흐름을 보이는 것을 확인할 수 있었다.
결론
본 연구 결과 statin 사용이 급성기 뇌경색 환자들의 임상경과지표에 유의한 영향을 미치지 않은 것으로 분 석이 되었다. 하지만 다른 논문들에서 적극적인 statin 의 사용이 급성기 뇌경색 환자의 예후에 좋은 결과를 보이고 있으며,
9)-11),17)고강도 statin의 사용이 동양인, 고령환자에서도 좋은 안전성 자료를 갖고 있으므로
16)향후 급성기 뇌경색 환자에서 statin 사용 가이드라인 확립을 위해서는 동일한 뇌졸중 발병기전을 갖는 국내 급성기 뇌경색 환자를 대상으로 statin 강도에 따른 임 상결과 차이를 보는 전향적인 대규모 연구가 필요할 것 으로 사료된다.
참고문헌
1) Park T, Kim M, Lee K et al. Population attributable risk of major risk factors for ischemic stroke in the Korean population.
Korean J Stroke 2008;10:125-33.
2) Hong K-S, Bang OY, Kang D-W et al.
Stroke statistics in Korea: part I.
Epidemiology and risk factors: a report from the korean stroke society and clinical research center for stroke. Journal of Stroke 2013;15(1):2-20.
3) Investigators SPbARiCL. High-dose ator- vastatin after stroke or transient ischemic attack. N engl J med 2006;2006(355):549-59.
4) Amarenco P, Lavallee P, Touboul P-J.
Statins and stroke prevention. Cerebrovas- cular Diseases 2003;17(Suppl. 1):81-8.
5) Vaughan CJ, Delanty N. Neuroprotective properties of statins in cerebral ischemia and stroke. Stroke 1999;30(9):1969-73.
6) Expert Panel on Detection E. Executive summary of the Third Report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults
′
(Adult Treatment Panel III). Jama 2001;
285(19):2486.
7) Stone NJ, Robinson JG, Lichtenstein AH et al. 2013 ACC/AHA Guideline on the treat- ment of blood cholesterol to reduce athero- sclerotic cardiovascular risk in adults: a report of the American college of cardiolo- gy/American heart association task force on practice guidelines. Journal of the American College of Cardiology 2014;63(25_PA):2889- 934.
8) Jauch EC, Saver JL, Adams HP et al.
Guidelines for the early management of patients with acute ischemic stroke a guide- line for healthcare professionals from the American Heart association/American stroke association. Stroke 2013;44(3):870-947.
9) Chroinin DN, Callaly EL, Duggan J et al.
Association between acute statin therapy, survival, and improved functional outcome after ischemic stroke the north dublin popu- lation stroke study. Stroke 2011;42(4):1021- 9.
10) Charidimou A, Merwick A. Statin therapy in acute ischemic stroke:Time for large ran- domized trials? Neurology 2016;86(12):1082- 3.
11) Blanco M, Nombela F, Castellanos M et al.
Statin treatment withdrawal in ischemic stroke a controlled randomized study.
Neurology 2007;69(9):904-10.
12) Furie KL, Kasner SE, Adams RJ et al.
Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack a guideline for healthcare profes- sionals from the American heart associa- tion/American stroke association. Stroke 2011;42(1):227-76.
13) Tsivgoulis G, Katsanos AH, Sharma VK et al. Statin pretreatment is associated with
better outcomes in large artery atheroscle- rotic stroke. Neurology 2016;86(12):1103-11.
14) Thanvi B, Treadwell S, Robinson T. Early neurological deterioration in acute ischae- mic stroke: predictors, mechanisms and management. Postgraduate Medical Journal 2008;84(994):412-7.
15) Roquer J, Rodriguez-Campello A, Gomis M et al. Acute stroke unit care and early neu- rological deterioration in ischemic stroke.
Journal of Neurology 2008;255(7):1012-7.
16) Liao JK. Safety and efficacy of statins in Asians. The American journal of cardiology 2007;99(3):410-4.
17) Chung J-W, Hwang J, Lee MJ et al.
Previous statin use and high-resolution magnetic resonance imaging characteristics of intracranial atherosclerotic plaque.
Stroke 2016;47(7):1789-96.
18) Yoshimura S, Uchida K, Daimon T et al.
Randomized controlled trial of early vs delayed statin therapy in patients with acute ischemic stroke. LB 17. Presented at:
the 2017 International Stroke Conference.
Feb. 22-24, 2017;Houston, TX.
′
′
′
′