학술강좌
BIOTERRORISM
김명은
인제대학교 부산백병원 약제부
Introduction
생물테러(Bioterrorism)란 바이러스, 세균, 곰팡 이, 독소 등을 사용하여 사람, 동물 혹은 식물을 살상 하거나 질병을 일으키는 것을 목적으로 하고 궁극적 으로는 사회 붕괴를 의도하는 행위를 말한다.
생물테러는 기원전부터 전쟁이나 살상을 위하여 개 발, 사용되어 왔다. 현재까지도 10여 개국에서 생물 무기를 보유하고 있는 것으로 추정되며, 2001년 미 국에서 우편물을 이용한 탄저균 사건 이후로 생물 테 러에 대한 관심이 높아졌다.
미국 질병관리본부(CDC)에서는 생물테러의 발견 과 대응 능력향상을 위하여 일반인뿐만 아니라 의료 인을 대상으로 생물테러 관련정보 제공, 교육자료 개 발, 생물테러 발생 시 필요한 약물과 백신 비축, 효율 적인 communication 프로그램과 진단법 개발을 위한 연구 활동 등을 하고 있다. 우리나라에서도 2004년 질병관리본부에서 생물테러 대응 종합정보 망을 새로이 구축하여 생물테러와 관련된 각종 정보 를 제공하고 발생 상황과 위험 평가에 따라 "주의", "
경보", "위험"단계로 구분, 각 단계별 대응 전략을 수 립하고 있다.
Bioterrorism Agents
CDC에서는 생물 무기를 그 위험도와 국가사회에 대한 영향력에 따라 categoryA, B, C로 분류하여 각각에 대한 정보를 제공하고 있다.
Category A:쉽게 전파되거나 사람간의 전염력이
크고 사망률이 높아 사회를 공포에 빠뜨리기 쉬우 며 공중 보건 차원에서 특수한 비상 대비책이 필요 한 것; Anthrax, Smallpox, Plague, Botulism, Viral Hemorrhagic Fever, Tularemia.
Category B:중등도의 전염력과 유병률을 가지고 사망률이 낮으며 진단능과 질병감시의 강화가 필요 한 것; Brucellosis (Brucella species), Food safety threats (Salmonella species, Escherichia coli O157:H7, Shigella), Q fever (Coxiella burnetii), Ricin toxin from Ricinus communis (castor beans)
Category C:유병율과 사망률이 높고 생산, 전파가 용이하여 집단 전파를 위해 개발될 가능성이 있는 병원체; Nipah virus, hanta virus
이 중에서 category A에 속하는 병원체와 질병을 살펴보면 다음과 같다.
▶ Anthrax(탄저병)
병원체 : Bacillus anthracis(포자 형성)
전파 : 포자나 균의 접촉·섭취·흡입으로 감염되 며 사람-사람의 전염은 없다.
진단 : 배양, Immunohistochemical staining, PCR 등
임상양상 : 잠복기는 1~7일(~60일)이다.
Inhalational anthrax의 초기에는 fever, cough, second stage에서는 fever, dyspnea, shock, chest x-ray상 massive lym- phadenopathy, stridor, hemorrhagic menin- gitis, hypotension과 cyanosis가 급속도로 진행
되어 수시간 내에 사망할 수도 있다. Cutaneous anthrax는 local edema, round ulcer, gastroin- testinal anthrax의 oral-pharyngeal form은 oral & esophageal ulcer, edema, sepsis, abdominal form은 nausea, vomiting,bloody
diarrhea 등의 증상을 나타낸다.
치료 & 노출 후 예방 : 표1~표3
백신 : 미국 국방성이 보유하고 있는 탄저균 백신은 BioThrax로서 노출 후 예방에 단독으로는 효과가 없고 항생제 치료와 병행하여 사용할 수 있다.
표 1. Recommendations for Treating Cutaneous anthrax
Patient Group Initial Oral therapy Duration
성인 Ciprofloxacin 500 ㎎ q 12hrs 임산부 OR Doxycycline 100 ㎎ q 12hrs
소아
Ciprofloxacin 10~15 ㎎/㎏ q 12hrs (Max. 1 g/일) OR Doxycycline > 8세(> 45 ㎏): 100 ㎎ q 12hrs, 60일
> 8세(≤ 45 ㎏): 2.2 ㎎/㎏ q 12hrs,
≤ 8세: 2.2 ㎎/㎏ q 12hrs
면역저하환자 정상 환자와 동일
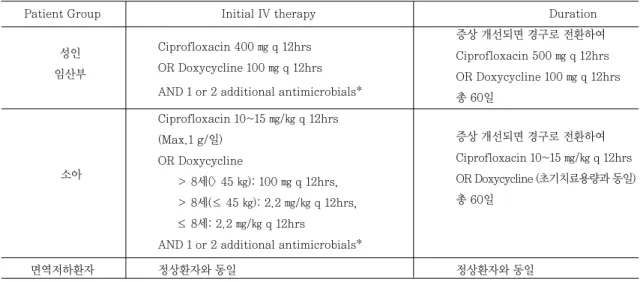
표 2. Recommendations for Treating Inhalational, Gastrointestinal Anthrax in the Contained Casualty Setting
Patient Group Initial IV therapy Duration
Ciprofloxacin 400 ㎎ q 12hrs 증상 개선되면 경구로 전환하여
OR Doxycycline 100 ㎎ q 12hrs Ciprofloxacin 500 ㎎ q 12hrs AND 1 or 2 additional antimicrobials*
OR Doxycycline 100 ㎎ q 12hrs 총 60일
Ciprofloxacin 10~15 ㎎/㎏ q 12hrs
증상 개선되면 경구로 전환하여 (Max.1 g/일)
Ciprofloxacin 10~15 ㎎/㎏ q 12hrs OR Doxycycline
OR Doxycycline (초기치료용량과 동일)
> 8세(> 45 ㎏): 100 ㎎ q 12hrs,
총 60일
> 8세(≤ 45 ㎏): 2.2 ㎎/㎏ q 12hrs,
≤ 8세: 2.2 ㎎/㎏ q 12hrs
AND 1 or 2 additional antimicrobials*
면역저하환자 정상환자와 동일 정상환자와 동일
* Rifampin, vancomycin, amoxicillin, quinupristin-dalfopristin, clindamycin, clarithromycin, telithromycin 등이 B.Anthracis에 in vitro에서 활성이 있는 것으로 알려져 있다. Combination therapy에 대한 근거는 적지만 2001년 탄저균 테 러 이후에 보고된 data로는 multiple antibiotics로 치료받은 환자의 생존율이 더 높았고 테러에서는 내성을 가진 균주를 생산하 여 이용할 수도 있으므로 항생제 병합 요법이 추천된다.
# Penicillin이 FDA로부터 anthrax에 적응증이 있지만 포자가 발아하는 곳인 macrophage로의 침투력이 떨어지고 penicillinase 를 생산할 가능성이 있기 때문에 추천되지 않는다.
# Anthrax meningitis에 이상적인 항생제 병합요법은 없지만 ciprofloxacin에 chloramphenicol, rifampin, penicillin을 추가 하는 것이 추천되며 doxycycline은 ciprofloxacin에 비해 CNS로의 침투력이 떨어지므로 추천되지 않는다.
소아 성인 임산부
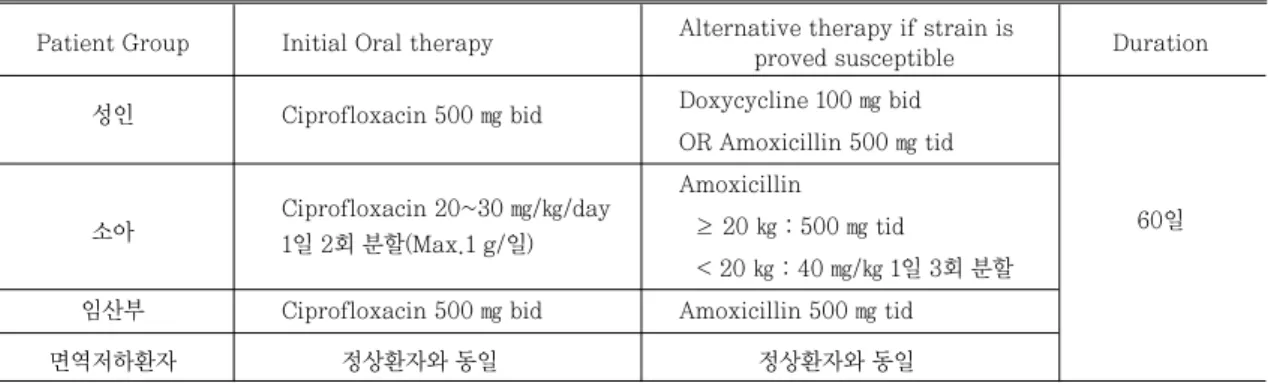
표 3. Recommendations for Treating Inhalational, Gastrointestinal Anthrax in the Mass casual- ty/Postexposure Prophylaxis Setting
Patient Group Initial Oral therapy Alternative therapy if strain is
Duration proved susceptible
성인 Ciprofloxacin 500 ㎎ bid Doxycycline 100 ㎎ bid OR Amoxicillin 500 ㎎ tid
소아 Ciprofloxacin 20~30 ㎎/㎏/day Amoxicillin
1일 2회 분할(Max.1 g/일) ≥ 20 ㎏ : 500 ㎎ tid 60일
< 20 ㎏ : 40 ㎎/㎏ 1일 3회 분할 임산부 Ciprofloxacin 500 ㎎ bid Amoxicillin 500 ㎎ tid
면역저하환자 정상환자와 동일 정상환자와 동일
▶ Smallpox(천연두, 두창) 병원체 : variola virus
전파 : 공기 전파(face to face contact), 오염된 침구나 옷에 접촉해도 감염된다.
진단 : electron microscopy, fluoroscent anti- body staining 등
임상양상 : 잠복기는 7~17일이다. 전구기(headache, high fever)를 지나 4~7일에 걸쳐 rash→macule→
papule→vesicle→pustule로 진행된 다음 딱딱해진 다. 감염 후에 65~80%의 환자가 심각한 얽은 자국 (pockmark)을 나타낸다.
치료 : smallpox의 치료제로 허가된 항바이러스제 는 없는데 Cidofovir IV가 동물과 in vitro model 에서 variola에 활성이 있는 것으로 알려져 있다.
노출 후 예방 : 노출 후 4일 내에 smallpox vac- cine을 투여해야 한다.
백신 : 미국 CDC가 보유하고 있는 Dryvax는 live vaccinia virus vaccine이다. 접종 후 vaccinia virus 감염 증상이 나타나면 vaccinia immune globulin을 투여한다. 백신 접종 후에 myoperi- carditis, angina 등이 보고되어 CDC에서는 coronary artery disease, congestive heart failure, cardiomyopathy, stroke, transient ischemic attack, angina 등 심장질환이 있는 경 우는 백신을 금하고 있고 또한 hypertension, hyperlipidemia, 흡연 등 심혈관질환의 위험인자 3가지 이상인 경우에도 백신 접종을 금하고 있다.
▶ Plague(페스트) 병원체 : Yersinia pestis
전파 : 감염된 벼룩에 물리거나 흡입으로 감염되 고, pneumonic plague는 비말감염으로 사람-사 람 전염 가능하다.
진단 : 배양, antigen detection, PCR
임상양상 : 잠복기는2~8일이다. Bubonic plaque 에서는 sudden fever, chills, weakness, bubo(사타구니, 겨드랑이, 목주위 림프절 부위에 inflamed swelling or abscess),ulcer 등을 보이 며, primary septicemic plague는 DIC (dis- seminated intravascular coagulation), 손가 락·발가락·코의 괴사를 나타낸다. Pneumonic plague (primary, secondary)는 broncho pneumonia, chest pain, dyspnea, hemopty- sis의 증상을 나타낸다.
치료 & 노출 후 예방 : 표4~표5
▶ Botulism(보툴리눔독소증)
병원체 : Clostridium botulinum이 생산하는 독 소인 botulinum(주로 Type A, B, E)
전파 : 소장이나 상처를 통한 흡수, 흡입으로 감염 되고 사람-사람의 전파는 없다.
진단:배양, mouse bioassay 등
임상양상 : 잠복기는 12~72시간(2~8일), acetyl- choline의 유리를 차단함으로써 "symmetric, descending flaccid paralysis with bulbar palsies, absence of fever, clear
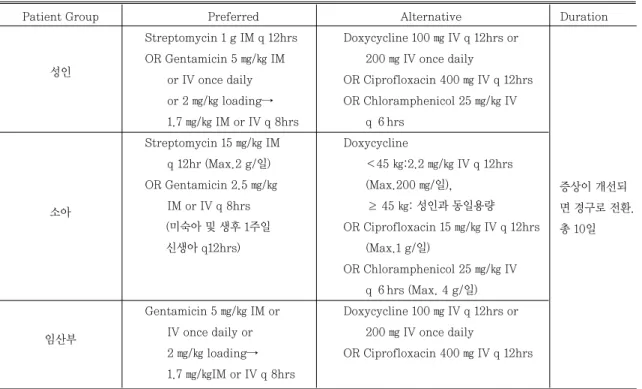
표 4. Treatment Recommendations for Pneumonic plague in a Contained Casualty Setting
Patient Group Preferred Alternative Duration
성인
Streptomycin 1 g IM q 12hrs Doxycycline 100 ㎎ IV q 12hrs or OR Gentamicin 5 ㎎/㎏ IM 200 ㎎ IV once daily
or IV once daily OR Ciprofloxacin 400 ㎎ IV q 12hrs or 2 ㎎/㎏ loading→ OR Chloramphenicol 25 ㎎/㎏ IV 1.7 ㎎/㎏ IM or IV q 8hrs q 6hrs
Streptomycin 15 ㎎/㎏ IM Doxycycline
q 12hr (Max.2 g/일) <45 ㎏:2.2 ㎎/㎏ IV q 12hrs OR Gentamicin 2.5 ㎎/㎏ (Max.200 ㎎/일),
IM or IV q 8hrs ≥ 45 ㎏: 성인과 동일용량
(미숙아 및 생후 1주일 OR Ciprofloxacin 15 ㎎/㎏ IV q 12hrs
신생아 q12hrs) (Max.1 g/일)
OR Chloramphenicol 25 ㎎/㎏ IV q 6hrs (Max. 4 g/일)
임산부
Gentamicin 5 ㎎/㎏ IM or Doxycycline 100 ㎎ IV q 12hrs or IV once daily or 200 ㎎ IV once daily
2 ㎎/㎏ loading→ OR Ciprofloxacin 400 ㎎ IV q 12hrs 1.7 ㎎/㎏IM or IV q 8hrs
소아
증상이 개선되 면 경구로 전환.
총 10일 sensorium(nosensory nerve damage)"의 특징
을 가진 마비 증상을 일으킨다.
치료 : Trivalent equine antitoxin (against toxin type A, B, E)1 vial (5500~8500 IU)을 1:10의 비율로 N/S로 희석해서 slow intra- venous infusion으로 투여하는데 이미 마비가 일 어난 곳에는 효과가 없다.
노출 후 예방 : 관찰
▶ Viral Hemorrhagic fever (바이러스성 출혈열) 병원체 : Filoviridae (Ebola virus, Marburg virus), Arenaviridae (Lassa virus,New World virus), Bunyaviridae (Rift Valley fever virus) Flaviviridae (Yellow fever virus,
표 5. Treatment Recommendations for Pneumonic plague in Mass casualty/
Postexposure Prophylaxis Setting
Patient Group Preferred Alternative Duration
성인 Doxycycline 100 ㎎ po q 12hrs Chloramphenicol
임산부 OR Ciprofloxacin 500 ㎎ po q 12hrs 25 ㎎/㎏ po q 6hrs mass casualty setting : 10일 postexposure
소아 Chloramphenicol prophylaxis : 7일
25 ㎎/㎏ po q 6hrs (Max. 6 g/day) Doxycycline
<45 ㎏ : 2.2 ㎎/㎏ po q 12hrs (Max. 200 ㎎/일),
≥ 45 ㎏: 성인과 동일용량 OR Ciprofloxacin 500 ㎎ po q 12hrs
(Max. 1 g/일)
Omsk hemorrhagic fever virus, Kyasanur Forest disease virus)
전파 : 감염된 동물 접촉,흡입, Rift Valley fever 와 flaviridae를 제외하고는 체액 속의 virus에 직 접 접촉하여 사람-사람으로 전염된다. 증상이 나 타나기 전에는 전염력이 없으나 병이 진행될수록 전염력이 커진다.
진단 : ELISA, RT-PCR 등
임상양상 : 잠복기는 2~21일이나 virus 종류에 따 라 다양하다. Fever, myalgia, hypotension, bradycardia, tachypnea 등의 증상으로 시작하 여 병이 진행됨에 따라 출혈의 합병증이 나타난다.
말기에는 shock/circulatory collapse, DIC, coma를 보여 치명적이다.
치료 : Ribavirin은 arena virus와 bunya virus 에만 활성을 가진다. Contained casualty set- ting에서는 Ribavirin을 IV로 30 ㎎/㎏ (~2 g) loading, 16 ㎎/㎏(~1 g) q6h for 4일→8 ㎎/㎏
(~500 ㎎) for 6일간 투여를 권장하며, Mass casualty setting에서는 Ribavirin을 po로 2 g
loading→ 600 ㎎ bid (≤75 ㎏: 2 g loading → 아침 400 ㎎-저녁 600 ㎎)로 10일간 투여를 추천 하고 있다. Ribavirin의 IV제제는 현재 시판되고 있지 않고 연구용 약물로서만 제조되고 있다.
노출 후 예방 : 관찰
▶ Tularemia(야토병)
병원체 : Francisella tularensis
전파 : 진드기, 파리, 모기 등에 의해 감염된 동물 접촉, 오염된 물·토양·식물, 흡입에 의해 감염되 며 사람-사람 감염은 되지 않는다.
진단 : 배양, direct fluorescent antibody, immunohistochemical stain
임상양상 : 잠복기는 3~5일(1~14일)이다. 급작스 러운 fever, chills, sore throat, substernal pain이 나타나나 pneumonia의 전형적인 증상인 pleuritic pain, purulent sputum, tachypnea, dyspnea, hemoptysis 등은 나타나지 않는다.
치료 & 노출 후 예방 : 표6~표7
표 6. Treatment Recommendations for Tularemia In a Contained Casualty Setting
Patient Group Preferred Alternative Duration
성인
Streptomycin 1 g IM q 12h Doxycycline 100 ㎎ IV q 12hrs OR Gentamicin 5 ㎎/㎏ IM OR Ciprofloxacin 400 ㎎ IV q 12hrs
or IV once daily OR Chloramphenicol 15 ㎎/㎏ IV q 6hrs
Streptomycin 15 ㎎/㎏ IM
Doxycycline
q 12hrs (Max. 2 g/일)
<45 ㎏: 2.2 ㎎/㎏ po q 12hrs
OR Gentamicin 2.5 ㎎/㎏
(Max. 200 ㎎/일),
IM or IV q 8hrs ≥ 45 ㎏: 성인과 동일용량
OR Ciprofloxacin 15 ㎎/㎏ IV q 12hrs (Max. 1 g/일)
OR Chloramphenicol 15 ㎎/㎏ IV q 6hrs (Max . 4 g/일)
임산부
Gentamicin 5 ㎎/㎏ IM or
Doxycycline 100 ㎎ IV q 12hrs IV once daily
OR Ciprofloxacin 400 ㎎ IV q 12hrs OR Streptomycin 1 g IM
q 12hrs
Streptomycin, Gentamicin, Ciprofloxacin : 10일
Doxycycline, Chloramphenicol : 14~21일 소아
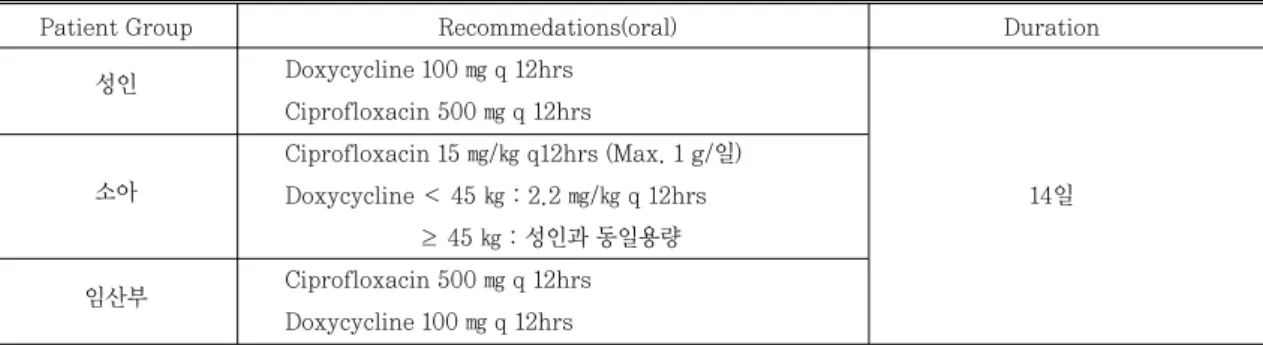
표 7. Treatment Recommendations for Tularemia In the Mass Casualty/Postexposure Prophylaxis Setting
Patient Group Recommedations(oral) Duration
성인 Doxycycline 100 ㎎ q 12hrs Ciprofloxacin 500 ㎎ q 12hrs
소아
Ciprofloxacin 15 ㎎/㎏ q12hrs (Max. 1 g/일)
Doxycycline < 45 ㎏ : 2.2 ㎎/㎏ q 12hrs 14일
≥ 45 ㎏ : 성인과 동일용량 임산부 Ciprofloxacin 500 ㎎ q 12hrs
Doxycycline 100 ㎎ q 12hrs
Conclusion - Role of the Pharmacists
지역별 기관에서의 적절한 대응이 생물무기 공격 후 유병율과 사망률에 큰 영향을 준다. 그러므로 vaccination, 약물 요법과 특정 환자군에 대한 용량 추천, 부작용 모니터링, 환자 교육, 조제 등의 부문 에서 병원 약사의 역할은 중요하다. 미국의 경우 약 사는 "National Pharmacist Response Team"을 통해 국가의 비상사태 시 연방 정부의 일원으로서 다른 직종의 팀과 함께 활동한다.
생물테러 등 비상사태가 발생하면 약사는 타기관 과의 협조 체계를 통해 합리적인 비축약품 결정과 재고관리를 해야 하고 진료부서와 협의하여 생물테 러시 사용되는 항생제의 처방을 제한하는 등 약품
품귀현상에 대비하여야 한다. 이를 위해 약사는 review article, 인터넷 등을 활용해서 생물 테러에 대한 기초 지식뿐만 아니라 최신 치료 경향 등을 파 악하고 정부의 테러 대응 전략에 대한 정보를 갖추 어야 한다.
출처
Bioterrorism, Pharmacotherapy Self- Assessment Program, 5th Edition
참고문헌
1. http://www.bt.cdc.gov
2. http://www.bioterrorism.kcdc.go.kr
시험문제
1. 다음 중 사람에서 사람으로 전염되지 않는 것 은?
ⓐ 페스트
ⓑ 천연두
ⓒ 바이러스성출혈열
ⓓ 보툴리눔독소증
2. CDC 생물무기 분류 중 category A에 속하지 않는 것은?
ⓐ 탄저병
ⓑ 한타바이러스
ⓒ 야토병
ⓓ 천연두
3. 다음 중 잘못 연결된 것은?
ⓐ 보툴리즘-연수 마비(bulbar palsy) 증상이 나타난다.
ⓑ 천연두-천연두 환자가 사용하던 이불에 접 촉해도 전염된다.
ⓒ 바이러스성 출혈열-증상이 나타나기 전에도 전염성이 있다.
ⓓ 탄저병-치료 및 노출 후 예방을 위한 투약기 간은 총 60일이다.
4. 보건 복지부에서 탄저병 테러 위험 경보를 발령 했다. 다음 중 이에 대한 대비로 병원에서 비축 해야 하는 약품이 아닌 것은?
ⓐ Ciprofloxacin
ⓑ Doxycycline
ⓒ Cefmetazole
ⓓ Amoxicillin
5. 병원체와 질병이 잘못 연결된 것은?
ⓐ Ebola virus-천연두
ⓑ Francisella tularensis-야토병
ⓒ Bacillus anthracis-탄저병
ⓓ Yersinia pestis-페스트
1 2 3 4 5 6 7
④ ① ③ ① ② ① ④
지난호 정답(비만)