Copyright 2016 The Korean Society of Neuro-Ophthalmology http://neuro-ophthalmology.co.kr 27
주시유발안진과 주기교대안진
박재한
대구가톨릭대학교병원 신경과
Gaze Evoked and Periodic Alternating Nystagmus
Jae Han Park, MD
Department of Neurology, School of Medicine, Catholic University of Daegu, Daegu, Korea
Gaze-evoked nystagmus (GEN) is a drift of the eye which is only present for certain directions of gaze away from straight ahead. It is the most common form of nystagmus encountered in clinical practice. End point nystagmus is a variant of GEN. It is basically GEN in persons who are otherwise normal. It is more frequently seen with prolonged gaze holding and also with large eccentrici- ties. It is often somewhat torsional. The judgement as to whether nystagmus is called GEN or end point, is presently one made by the experience of the examiner. We think it best to avoid the term end point nystagmus entirely. Other nystagmus related to GEN are centripetal and rebound nystagmus. If patients with GEN are encouraged to sustain their attempt to look eccentrically, their nystagmus may reverse direction (“centripetal nystagmus”) and the eyes are then returned to the central position, a short live re- verse directed nystagmus, which is called rebound nystagmus. Periodic alternating nystagmus (PAN) refers to horizontal or hori- zontal rotary nystagmus that reverses its direction with a periodicity of 1 to 6 minutes and is characterized by a quiescent interval of 4 to 20 seconds between reversals. However, periodicity and quiescence are not regular in all cases and can be as short as a few seconds. PAN is most commonly found either in its congenital form or after cerebellar or pontomedullary lesions. Rarely, PAN has been described in peripheral disorders.
Keywords: Gaze evoked nystagmus; End point nystagmus; Periodic alternating nystagmus
서 론
사물을 정확하게 보기 위해서 안구운동이 일어나게 되며, 안구운 동을 통해 사물의 상이 망막의 중심오목(fovea centralis)에 위치하게 되면 가장 명확한 상을 얻을 수 있다.1 따라서 인체의 발달과정에서 사 물의 상을 중심오목에 유지하여 정확한 시각을 유지하기 위하여 머 리운동과 안구운동이 발전되어 왔고, 전정안반사(vestibule-ocular re- flex), 부드런따라보기(smooth pursuit), 시운동계(optokinetic system), 이향안구운동계(vergence)뿐만 아니라 주시고정계(fixation) 가 그 역 할을 한다.2 이러한 정상적인 기능에 문제가 발생하면 다양한 형태의
안진이 발생하게 되는데 본문에서는 그 중에서도 신경적분체(neural integrator)의 장애로 인한 주시유발안진(gaze evoked nystagmus, GEN), 또한 주시유발안진과 관련있는 극위안진(endpoint nystagmus), 구심안진(Centripetal nystagmus) 및 반동안진(Rebound nystagmus), 그리고 추가적으로 교대안진의 일종인 주기교대안진(Periodic alter- nating nystagmus, PAN) 에 대해 자세히 살펴보도록 하겠다.
주시유발안진(GEN)
외측 주시를 할 때 안구를 그 위치에서 지속적으로 유지시키는 주
Correspondence to: Jae Han Park, MD
Department of Neurology, Catholic University of Daegu, School of Medicine, Daegu Catholic University Hospital, 33 Duryugongwon-ro 17-gil, Nam-gu, Daegu 42472, Korea Tel: +82-53-650-3626, Fax: +82-53-654-9786, E-mail: [email protected]
Received: Jul. 28, 2016 / Accepted: Sep. 26, 2016
REVIEW
ISSN: 2234-0971 대한안신경의학회지: 제6권 제2호
Clin Neuroophthalmol 6(2):27-30, December 2016
Park JH • Gaze Evoked and Periodic Alternating Nystagmus
Clin Neuroophthalmol 6(2):27-30, December 2016 28 http://neuro-ophthalmology.co.kr
시고정(gaze holding)은 사물이 보이지 않는 어두운 곳에서도 일어나 기 때문에, 일반적인 시고정(visual fixation)의 기전만으로는 설명 할 수 없다.3 안구가 원위치(primary position)를 벗어나 외측으로 지속적 으로 치우쳐있기 위해서는 안구를 원래의 위치로 되돌리려는 안구 주위 조직의 탄력에 대항할 수 있는 외안근의 긴장성 수축이 필요하 다. 이를 위해서는 신경조직의 지속적인 흥분이 필요하며, 이러한 역 할을 담당하는 구조물을 신경적분체(neural integrator)라 한다.4 신경 적분체는 전정안구반사(vestibular-ocular reflex), 신속보기(saccade)에 서 안구의 이동속도에 대한 명령(pulse)을 안구의 위치에 대한 정보 (step)로 전환하여 외안근의 수축을 유지한다(Fig. 1).5 따라서 신경적 분체의 기능이 정상이라면, 신속보기의 이동속도에 대한 명령은 완벽 하게 위치에 대한 정보로 변환되어 안구가 외측에서 고정되지만 기능 이 떨어진 경우에는 위치에 대한 정보가 감쇠되고 안구가 원위치로 돌아오게 되며, 이를 보상하기 위한 안진이 발생하게 되는데, 이를 주 시유발안진이라고 한다(Fig. 2).5 수평방향의 안구운동에서는 설하전 핵(nucleus prepositus hypoglossi, NPH), 내측 전정신경핵(medial ves- tibular nucleus, MVN)과 소뇌 타래엽(flocculus)이 신경적분체 역할을 하며, 수직 및 회선 안구운동에서는 Cajar사이핵(interstitial nucleus of Cajar, INC)이 관여한다.6 주시유발안진에서 발생하는 안구운동의 서 상(slow phase)은 주로 감속형을 보이며 일부 정상인에서도 지속적인 외측주시 동안에 작은 시계추진동(pendular oscillation) 이나 사각파
된떨림(square wave jerk)이 관찰되기도 한다. 가장 흔한 주시유발안진 의 원인은 진정제와 간질약을 포함한 약물이며, 특히 알코올 중독에 의해서도 발생할 수 있다. 약물에 의한 주시유발안진은 수평 또는 수 직방향에서 모두 나타날 수 있으며, 약물이 작용하는 정확한 위치는 알 수 없으나 소뇌나 전정신경핵에 영향을 주는 것으로 생각된다.5,7 주 시유발안진은 다양한 소뇌질환에서도 발생하는데 타래엽과 같은 전 정소뇌와 그와 관련된 신경로의 이상으로 발생하는 것으로 알려져 있으며, 부드런따라보기나 전정안반사 장애와 같은 다른 이상소견이 동반되는 경우가 많다.8 또한 주시유발안진은 가족성 간헐성 현훈(fa- milial episodic vertigo)과 제2형 실조증(ataxia type 2)에서도 관찰될 수 있고, 이 경우 acetazolamide와 4-aminopyridine에 의해 호전될 수 있 다.9,10 설하전핵과 내측전정신경핵에 직접 영향을 주는 뇌간질환은 주 시유발안진을 발생시킨다. 또한 뇌간의 병변은 전정불균형(vestibular imbalance)을 동반하기도 하는데, 이런 경우에는 전정불균형으로 인 한 안진으로 인해 주시유발안진을 구분하기 어려울 수도 있다. 주시 유발안진과 감별해야 될 안진으로 극위안진이 있는데, 특별한 이상소 Fig. 1. Simplified scheme of generation of a neural signal for a saccade that
takes the eye to an eccentric eye position (E) and subsequently holds it steadily there. A pulse of innervation (velocity command) is generated by burst neurons (B) that project to ocular motoneurons (OM), so causing a phasic contraction of the extraocular muscles to move the eye quickly through angle E. This same pulse signal is sent to neural integrator cells (NI), which generate a step of in- nervation. The step is a position command that causes a tonic contraction of the extraocular muscles to hold the eye steadily at its new position. OM carry the summed pulse-step neural signal. Vertical lines represent individual dis- charges of neurons. Underneath the schematized neural (spike) discharge is a plot of discharge rate versus time.
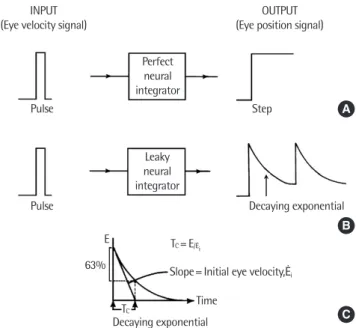
Fig. 2. Quantitative aspects of the neural integrator. (A) For saccades, the input to the neural integrator is a pulse, which may be thought of as an eye velocity signal. If neural integration is perfect, then the output will be a step, which may be thought of as an eye position signal. (B) If the integration of eye velocity sig- nals is imperfect (i.e., if the neural integrator is “leaky”), then the eye position signal will be a decaying exponential. Thus, the eye will drift back toward the midline until a corrective quick-phase puts the eye back on target. This causes gaze-evoked nystagmus. (C) The centripetal drift of the eyes that occurs with a leaky integrator can be described by its time constant (Tc), given by the time at which the eye has drifted 63% of the way back to the midline. Thus, the “leaki- er” the integrator, the shorter the time constant. A convenient way of calculat- ing the time constant is from the ratio of the initial displacement of the eye from midline (E) to the initial velocity of eye drift (Ėi).
INPUT
(Eye velocity signal) OUTPUT
(Eye position signal)
Perfect neural integrator
Leaky neural integrator Pulse
Pulse
Step
Decaying exponential
Decaying exponentialTC
TC= E/Ėi
Slope= Initial eye velocity,Ėi
Time E
63%
A
B
C
주시유발안진과 주기교대안진 • 박재한
Clin Neuroophthalmol 6(2):27-30, December 2016 http://neuro-ophthalmology.co.kr 29
견이나 병리기전 없이 외측주시를 하는 동안 정상인에서 나타나는 안 진을 말하며 생리적안진(physiologic nystagmus), 피로안진(fatigue nys- tagmus) 등과 같은 의미로도 사용되기도 한다.11 두 가지를 확실히 구 분할 수 있는 방법은 없지만 일반적으로 다음과 같은 특징이 있을 때 극위안진일 가능성이 높다. 첫째, 상대적으로 안진의 진폭이 작고 빈 도가 낮은 경우, 둘째, 양쪽 안구의 안진의 양상이 비슷한 경우. 셋째, 안진이 지속적이지 않고 일시적인 경우, 마지막으로 다른 안신경학적 이상소견이 없는 경우이다.11,12 또한 안진의 파형에 있어 주시유발안진 은 서상의 속도가 줄어드는 양상을 보이나 극위안진은 속도가 일정한 선상의 형태를 보이는 경우가 많다. 과거에는 안구가 원위치에서 40°
이하에서 나타나는 안진이 병적인 주시유발안진이라는 보고도 있었 고, 미국에서 알코올과 관련된 법적인 문제가 있을 때 주시유발안진 의 기준을 원위치에서 45° 이하에서 나타나는 경우로 하기도 했지만, 10°-20° 에서도 극위안진이 나타난다는 여러 보고들이 있어 그 기준과 극위안진이라는 이름에 대해서는 논란이 있다.11,12
구심안진(Centripetal nystagmus) 및 반동안진(Rebound nystagmus)
주시유발안진을 보이는 환자가 외측주시를 지속하는 경우 안진이 약간 아래로 치거나, 안진의 방향이 역전되는 경우를 구심안진이라 한다.13 만약 외측주시 후에 중심으로 돌아오면 일시적으로 외측으로 서상이 향하면서 주시했던 방향과 반대방향으로 안진이 발생하는 경 우를 반동안진(rebound nystagmus)이라고 한다.14 구심안진과 반동안 진은 주시유발안진의 구심전이(centripetal drift)를 교정하기 위한 뇌 간과 소뇌 기전을 반영한다고 할 수 있다. 반동안진을 일으키는 결정 적인 구조에 대해서는 잘 알려져 있지 않지만, 전정핵이나 연수 주위 구조물이 반동안진을 발생시키는데 중요할 것으로 생각된다.15,16
주기교대안진(PAN)
원위치에서 한 방향으로의 수평안진이 1-2분(90초)간 지속되다가 점차 약해지면서 사라지고, 0-10초 동안의 정지주기(null period)후에 반대방향으로의 안진이 생겨 같은 기간 동안 지속된다.2 선천적으로 발생하기도 하고, 후천적으로는 다음과 같은 질환들에서 보고되었다 (Table 1).17 많은 경우 안진의 기간이 약 4분 정도로 길어서 검사자가 수분이상 안진을 관찰하지 않으면 놓치기 쉬워 의심이 된다면 충분한 기간 관찰해야 한다. 안진의 방향이 바뀌는 사이에 짧은 전이기간 (transition period)이 존재하는데 이때 상향, 하방안진이나 사각파된 떨림이 관찰되기도 한다.17 선천적으로 발견되는 주기교대안진의 경우
안진의 방향역전이 덜 규칙적이며, 안진의 서상이 증가형이나 시계추 형으로 나타날 수 있다. 주기교대안진은 광범위한 대뇌병변을 보이는 환자에서 안구편위가 주기적으로 바뀌는 ping-pong주시와 감별이 필 요하다. 일부 환자에서는 약 20-40초의 짧은 주기로 안진의 역전이 관 찰되기도 한다. 후천성으로 주기교대안진이 발생하는 경우 주시 유무 에 따른 안진의 변화는 없는 것이 일반적이며, 일부 환자에서는 두위 회전이 같이 동반되기도 한다.18,19 부드런따라보기와 시운동성안진 (optokinetic nystagmus)의 이상이 잘 동반되나, 눈모음(convergence) 은 유지되는 경향을 보인다. 전정자극에 의해 안진이 영향을 받을 수 있는데, 일정한 회전자극을 주는 경우, 일시적으로 주기교대안진이 소실되기도 한다.17 후천성 주기교대안진은 다양한 질환에서 동반될 수 있는데, 주로 소뇌의 이상을 포함한다. 뇌간의 이상이 동반된 경우 주기교대주시편위(periodic alternating gaze deviation)의 양상으로 진 행할 수도 있다. 또한, 시력소실로 인하여 안진이 발생한 경우 시력이 호전되면서 안진이 호전되기도 한다. GABAB-ergic 약제인, baclofen이 대부분의 환자에서 후천성 주기교대안진을 경감시킬 수 있으며, 선천 성의 경우 그 효과는 미미하다.17 원숭이의 소뇌의 소절와 목젖을 제거 한 후 주기교대안진이 발생하였고, baclofen 투여 후 암실에서 관찰 시 주기교대안진은 소실되었다.20 Baclofen 효과를 고려할 때 소뇌 소절과 목젖이 GABA에 의해 전정회전반응을 억제한다고 볼 수 있다. 본래 소절과 목젖의 역할은 회전자극에 의하여 발생하는 안진의 시간경과 를 조절하는 기능을 한다(속도저장기능). 따라서, 소뇌와 목젖을 제거 하면, 회전자극에 의해 유발된 안진의 지속기간은 지나치게 길어진 다.20 이후 정상적인 전정기능에 의해 안진의 방향이 역전되는 주기교 대안진이 발생하는 것으로 생각 된다. 시각 안정화 (visual stabilization) 에 의해 일부 주기교대안진이 억제될 수 있으나, 소뇌 이상에 의해 발 생하는 경우는 이 효과를 기대하기는 어렵다.
Table 1. Etiology of periodic alternating nystagmus Arnold–Chiari malformation and other hindbrain anomalies Multiple sclerosis
Cerebellar degenerations
Cerebellar tumor, abscess, cyst, and other mass Lesion Creutzfeldt–Jakob disease
Ataxia telangiectasia Brainstem infarction
Lithium, anticonvulsant medications and seizures Infections affecting cerebellum, including syphilis Hepatic encephalopathy
Trauma
Following visual loss (due to vitreous hemorrhage or cataract)
Aperiodic form as a component of congenital nystagmus, especially in albinos Peripheral vestibular disorders
Park JH • Gaze Evoked and Periodic Alternating Nystagmus
Clin Neuroophthalmol 6(2):27-30, December 2016 30 http://neuro-ophthalmology.co.kr
REFERENCES
1. Shaikh AG, Ghasia FF. Physiology and pathology of saccades and gaze holding. NeuroRehabilitation. 2013;32:493-505.
2. Choi KD, Kim JS. Central nystagmus. Res Vestib Sci. 2004:3:36-45.
3. Bertolini G, Tarnutzer AA, Olasagasti I, Khojasteh E, Weber KP, Bockisch CJ et al. Gaze holding in healthy subjects. PLoS One. 2013;8:e61389.
4. Cannon SC, Robinson DA. Loss of the neural integrator of the oculomo- tor system from brain stem lesions in monkey. J Neurophysiol 1987;57:
1383-409.2.
5. Leigh RJ, Zee DS. The neurology of eye movements. 5th ed. New York:
Oxford University Press, 2015;360-385.
6. Nakamagoe K, Iwamoto Y, Yoshida K. Evidence for brainstem structures participating in oculomotor integration. Science. 2000; 288:857-859.
7. The Korean Society of Neuro-ophthalmology. Neuro-opthalmology. 1st ed. Seoul: Shinheung medscience, 2013:243-267.
8.Baier B, Dieterich M. Incidence and anatomy of gaze-evoked nystagmus in patients with cerebellar lesions. Neurology. 2011;76:361-365.
9. Bertholon P, Chabrier S, Riant F, Tournier-Lasserve E, Peyron R. Episodic ataxia type 2: unusual aspects in clinical and genetic presentation. Special emphasis in childhood. J Neurol Neurosurg Psychiatry. 2009;80:1289- 1292.
10. Strupp M, Kalla R, Claassen J, Adrion C, Mansmann U, Klopstock T, et al. A randomized trial of 4-aminopyridine in EA2 and related familial episodic ataxias. Neurology. 2011;77:269-275.
11. Abel LA, Parker L, Daroff RB, Dell’Osso LF. End-point nystagmus. Invest Ophthalmol Vis SCi. 1978;6:539-544.
12. Whyte CA, Petrock AM, Rosenberg M. Occurrence of Physiologic Gaze- Evoked Nystagmus at Small Angles of Gaze. Invest Ophthalmol Vis SCi.
2010;51:2476-2478.
13. Leech J, Gresty M, Hess K et al. Gaze failure, drifting eye movements, and centripetal nystagmus in cerebellar disease. Br J Ophthalmol. 1977;61:
774-781.
14. Bondar RL, Sharpe JA, Lewis AJ. Rebound nystagmus in olivocerebellar atrophy: a clinicopathological correlation. Ann Neurol. 1984; 15:474-477.
15. Cannon SC, Robinson DA. Loss of the neural integrator of the oculomo- tor system from brain stem lesions in monkey. J Neurophysiol. 1987;57:
1383-1409.
16. Hashimoto T, Sasaki O, Yoshida K, Takei Y, Ikeda S. Periodic alternating nystagmus and rebound nystagmus in spinocerebellar ataxia type 6. Mov Disord. 2003;18:1201-1204.
17. Leigh RJ, Zee DS. The neurology of eye movements. 5th ed. New York:
Oxford University Press, 2015;657-768.
18. Kim SH, Chung WK, Kim BG, Hwang CS, Kim MJ, Lee WS. Periodic al- ternating nystagmus of peripheral vestibular origin. Laryngoscope.
2014;124:980-983.
19. Tustusmi T, Ikeda T, Kikuchi S. Periodic alternating nystagmus caused by a medullary lesion in acute disseminated encephalomyelitis. Otol Neu- rotol. 2014;35:861-865.
20. Waespe W, Cohen B, Raphan T. Dynamic modification of the vestibulo- ocular reflex by the nodulus and uvula. Science. 1985;228:199-202.