교신저자: 유봉구, 부산시 서구 암남동 34, 602-702, 고신대학교 복음병원 신경과학교실 Tel: 051-990-6364, Fax: 051-990-3077, E-mail: [email protected]
Background: B-type natriuretic peptide (BNP), a serum marker for congestive heart failure, is secreted by the cardiac ventricles in response to excessive stretching. Recent reports suggest that high BNP levels may predict cognitive dysfunction in older patients with cardiovascular disease. The BNP study for different type of dementia is very rare. The aim of the study was to compare the plasma BNP levels between Alzheimer’s disease (AD) and subcortical vascular dementia (SVaD) and to estimate the clinical significance of BNP for dementia.
Methods: We selected two groups of elderly with neurocognitive and functional impairment described as AD and SVaD. Obtained data were analyzed with respect to neuropsychological tests (Korean version of Mini-mental State Examination, Clinical Dementia Rating, and Global Deterioration Scale) and clinical parameters. We measured the plasma BNP levels in 73 patients with AD and 40 patients with SVaD.
Results: Neuropsychological tests did not differ significantly between patients with AD and SVaD.
Compared with Alzheimer patients (56.5±45.7 pg/mL), BNP was elevated in subcortical vascular de- mentia (101.4±225.7 pg/mL, P=0.037). But no significant association was found between K-MMSE and BNP.
Conclusion: SVaD is associated with elevated BNP levels than AD. Elevated BNP probably reflects the larger cardiovascular burden in patients with SVaD. The result probably reflects the large amount of cardiovascular comorbidity in patients with subcortical vascular dementia.
Key Words: Alzheimer’s disease, Natriuretic peptide, Subcortical vascular dementia
피질하혈관성치매에서 증가된 혈장 B형 나트륨이뇨펩티드
김명국, 유봉구, 권수경1
고신대학교 의과대학 신경과학교실, 1온종합병원 내과
Elevated Plasma B-type Natriuretic Peptide Levels in Patients with Subcortical Vascular Dementia
Meyung-Kug Kim, M.D., Bong-Goo Yoo, M.D., Su-Kyoung Kwon, M.D.1 Department of Neurology, Kosin University College of Medicine,
1Department of Internal Medicine, On Hospital, Busan, Korea
서 론
B형 나트륨이뇨펩티드(B-type natriuretic peptide, BNP)는 32개의 아미노산으로 구성된 폴리펩티드로 심실 근육의 과도한 신장에 의한 반응으로 심실의 심근세포에서 분비된다.1,2) 일반적으로 울혈심부전의 좌심실 기능부전에서 증가되며, 증상의 심한 정도 및 예후와 관련이 있다.1-3) 또한 혈장 BNP는 심부전, 심방세동, 뇌졸중, 일과성 허혈발작 등의 위험도를 예측할 수 있는 지표이기도 하다.3)
울혈심부전 환자는 인지기능 장애나 치매의 위험도가 높으며, 높은 BNP 수치는 심장혈관질환을 가진 노년에서 인지장애를 예측할 수 있는 인자로도 알려져 있다.4-7) 지금까지 치매에서 BNP에 대한 연구는 적었 고, 각 치매 유형에 따른 보고도 매우 드물다. 울혈심부전은 알츠하이머병(Alzheimer’s disease, AD)과 관련성 은 명확하게 알려져 있지 않으나, 피질하혈관성치매(Subcortical vascular dementia, SVaD)와는 연관이 있다.8) 이는 SVaD가 심혈관계의 문제로 인해 발생하기 때문이며, BNP는 AD보다는 SVaD에서 더 연관이 있을 것으 로 여겨진다.
본 연구는 임상 증상이 유사한 AD와 SVaD에서 혈장 BNP치를 비교해 보고 BNP와 임상 증상과의 관계 및 두 질환에서 BNP의 임상적 의미를 알아보고자 하였다.
방 법
1. 연구대상
2007년 1월부터 2010년 7월까지 인지기능 장애를 주소로 본원에 입원한 AD와 SVaD 중에서 연구 포함기 준을 만족하는 AD 73명과 SVaD 40명을 연구 대상으로 하였다. AD는 Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV)의 치매 정의를 만족하고, National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA)9)의 probable AD의 진단 기준을 만족하는 경우로 하였다. SVaD는 DSM-IV의 치매 정의를 만족하고, National Institute of Neurological Disorders and Stroke Association Internationale pour la Recherche et l’Enseignement en Neurosciences (NINDS- AIREN)10)의 probable 또는 possible 혈관성치매의 정의를 만족하는 환자로 하였다. 연구 대상군에서는 모두 뇌 MRI와 BNP 검사가 시행되었다.
연구 대상군의 제외 기준은 과거력에서 인지기능의 저하를 일으킬 수 있는 우울증 같은 주요 정신질환, 갑상선 질환, 간이나 신장 질환, 매독, 비타민 B12나 엽산 결핍, 악성종양, 알츠하이머병 외의 퇴행성 뇌질환, 뇌종양, 두부외상, 알콜중독이나 약물남용의 기왕력 등이 있는 경우였다. BNP 수치에 영향을 줄 수 있는 허혈성 심질환 및 울혈심부전, 부정맥 등의 심장질환을 가진 경우도 제외하였다. SVaD 군에서 뇌위축, 열공 뇌경색, 백질변성을 제외한 피질뇌경색이나 다른 뇌병변을 동반하고 있는 경우는 대상군에서 제외하였다.
모두 신체검사, 신경학적검사, 혈액검사, 혈액화학검사, 비타민 B12 및 엽산, 갑상선기능검사, 매독혈청검사, 심전도, 흉부 X선 촬영 등을 시행하였다.
Table 1. Demographic data in AD and SVaD groups
Characteristics AD (n=73) SVaD (n=40) P-value Age (years)
Sex (Male/Female) Education level (years) Hypertension Diabetes Mellitus Hyperlipidemia K-MMSE CDR GDS BNP (pg/mL)
71.6±11.9 28/45 8.66±4.28 41 (56.1%) 23 (31.5%) 22 (30.1%) 16.8±5.2 0.96±0.83 4.08±0.95 56.5±45.7
74.3±8.5 14/26 8.02±4.54 21 (52.5%) 11 (27.5%) 13 (32.5%)
16.1±5 0.95±0.63 4.25±0.85 101.4±225.7
0.101 0.232
0.275 0.962 0.497 0.037
Plus-minus values are mean±SD. AD: Alzheimer’s disease, SVaD: subcortical vascular dementia, K-MMSE: Korean Mini-Mental Status Examination, CDR: Clinical Dementia Rating, GDS: Global Deterioration Scale, BNP: B-type natriuretic peptide.
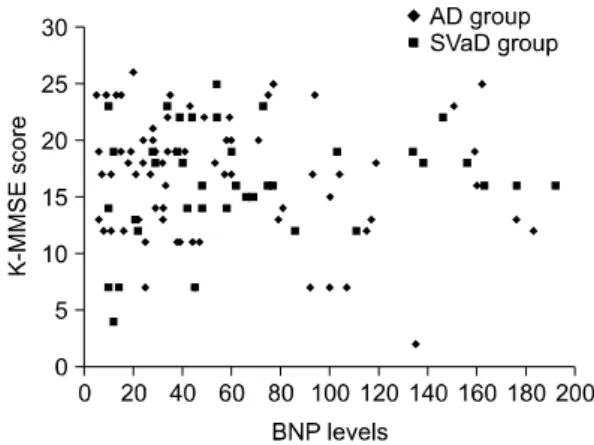
Figure 1. Scatter plot for the relation between BNP levels and K-MMSE score.
2. 조사방법
환자의 나이, 성별, 교육수준, 고혈압, 당뇨병 및 고지질혈증 등을 조사하였다. 인지기능의 측정은 한 국판 간이정신상태 검사(Korean Mini-Mental Status Examination, K-MMSE)11)를 사용하였으며, 환자 및 보 호자와의 면담을 통해 치매단계평가척도(Global Deterioration Scale, GDS)12)와 임상치매척도(Clinical Dementia Rating, CDR)13,14)를 이용하여 치매의 정도 를 평가하였다. 혈장 BNP치는 입원 다음날 아침에 공복 상태에서 정맥혈을 채취하여 Triage BNP 검사 (Beckman Coulter Immunoassay Systems for the In Vitro quantitative measurement)로 측정하였다.
3. 통계분석
SPSS (version 18.0)를 이용하여 나이, 교육수준, 혈장 BNP 농도, K-MMSE, CDR 및 GDS 점수 등을 두 군간에 student-t 검정으로 비교하였다. K-MMSE와 BNP간의 상관관계를 분석하였다. 유의 수준은 P<0.05로 하였다.
결 과
AD 73명과 SVaD 40명의 나이, 성별, 교육수준과 고혈압, 당뇨병, 고지질혈증 유무 등의 임상지표와 K-MMSE, CDR, GDS, 혈장 BNP 농도를 제시하였다(Table 1). 연령분포는 59∼90세로 평균 나이는 AD군에서 71.6±11.9세, SVaD군에서 74.3±8.5세였다. 남녀비는 각각 AD군에서 28명/45명, SVaD군에서 14명/26명으로 두 군 모두 여자가 많았다. 교육수준은 AD군 8.7±4.3년, SVaD군 8.0±4.5년이었다. K-MMSE, CDR, GDS 등의 신경심리검사에서 AD군은 각각 16.8±5.2점, 0.96±0.83점, 4.08±0.95점, SVaD군은 16.1±5점, 0.95±0.63점,
4.25±0.85점이었다. 임상지표 및 신경심리검사 결과는 두 군간에 차이가 없었다(Table 1). BNP 수치는 AD군 56.5±45.7 pg/mL, SVaD군 101.4±225.7 pg/mL로 SVaD군에서 유의하게 높았다(P=0.037). K-MMSE 점수는 AD 군 2∼27점, SVaD군 4∼25점의 분포를 보였고, BNP 수치와는 상관관계는 없었다(Figure 1).
고 찰
본 연구에서 SVaD는 AD보다 높은 BNP치를 보였다. 증가된 BNP치는 SVaD 환자에서 더 많은 심혈관계 부하(burden)가 작용하였기 때문으로 여겨진다.
혈관성치매에는 다발경색치매(Multi-infarct dementia, MID), 전략뇌경색치매(Strategic infarct dementia, SID), SVaD, 관류저하치매(Hypoperfusion dementia) 등이 있으며, 혈전색전성이나 혈류역학적인 문제와 연관되어 발생한다.15) SVaD가 가장 흔한데 약 40%에서 명백한 뇌경색증의 병력 없이도 발생한다.16) MID는 피질 및 피질하에 발생한 다발성 뇌경색이 원인이다. SID는 인지 기능에 중요한 시상, 해마, 꼬리핵(caudate nucleus), 속섬유막의 무릎부위(genu of internal capsule) 등을 침범한 단일 뇌경색으로 발생한다. MID와 SID는 주로 대혈관 병변이나 색전성 원인으로 발생하며, 심방세동이나 울혈심부전이 있는 경우가 많다. 따라서 BNP의 상승을 동반하는 경우가 많고 심질환과 연관된다.4,5,7,17) 본 연구에서 SVaD는 주로 열공경색이나 허혈성 백 질병변이 원인이며 이는 소혈관 질환을 의미하므로 BNP 상승과의 직접적인 연관성을 설명하기는 어렵다.
하지만 울혈심부전으로 인해 뇌의 관류압력의 감소가 나타나면 백질의 변성도 초래될 수 있을 것이다. AD 보다 SVaD에서 BNP의 상승은 뇌에서 혈관성 부하의 증가와 관련이 있다고 여겨진다.
SVaD에서 혈관성 부하의 증가로 인한 BNP 상승은 SVaD 및 울혈심부전, 심장기능이상이 같은 병태생리를 공유한다는 점으로 설명할 수 있다. 심근과 뇌 피질하백질 부위는 해부학적으로 문합이 없는 끝동맥의 혈액 공급을 받기 때문에 혈관의 폐색이나 관류장애에 취약하다. 따라서 노년 동맥경화증, 고혈압성 동맥병증, 혈관내피세포 기능이상, 혈관자동조절의 이상, 빈혈 등으로 혈액관류 및 산소나 당, 영양물질의 공급이 감 소되면 세포의 손상이 심해지게 되어 SVaD의 발병에 기여한다.16,18-22) 또한 울혈심부전은 뇌관류를 저하시키 고, 뇌경색의 위험을 증가시켜 인지기능의 저하를 초래할 수 있다.4,5) 따라서 울혈심부전시 증가하는 BNP가 SVaD에서도 증가할 수 있을 것이다.
본 연구는 환자군의 배제기준에서 울혈심부전을 제외하였다. 그러나 심부전의 표지자인 BNP는 SVaD에 서 AD보다 유의하게 증가되어 있었다. 이것은 심초음파를 이용한 두 군간의 직접적인 비교를 하지는 않았 지만, SVaD가 AD보다 혈관성 병변에 대한 부하가 더 높음을 시사한다.
심부전의 증상이 있는 경우 BNP치가 80∼100 pg/mL를 넘으면 진단에 의미가 있다.23) 이전의 연구들에서 울혈심부전은 BNP치가 각각 675±450 pg/mL와 1,076±138 pg/mL를 보였고, 심부전은 없고 좌심실기능부전만 있는 경우는 각각 141±31 pg/mL와 348±390 pg/mL를 보였다.23,24) 본 연구에서 BNP치가 AD군은 56.5±45.7 pg/mL, SVaD군은 101.4±225.7 pg/mL였다. 울혈심부전을 의심할만한 증상이나 징후가 있는 경우를 제외했기 때문에 SVaD군에서 AD보다 높은 BNP치는 심부전 때문에 증가된 것이 아니고 SVaD의 혈관부하가 원인일 것이다.
높은 BNP치가 인지기능 장애와 관련되는 기전은 명확하지 않으나 추정되는 가설로는 혈액뇌장벽 및 내피기능의 이상이 있다. 심혈관계 이상이 있는 환자에서 뇌혈관질환이나 혈액뇌장벽의 이상을 잘 동반하 기 때문에 BNP치가 높을 수 있고, 이로 인해 인지기능의 이상이 초래될 가능성이 높다. 또한 내피기능 장애가 높은 BNP치 및 뇌 백질변성과 연관되어 인지기능 장애를 유발한다.20,25,26) 따라서 증가된 BNP치는
AD보다는 SVaD와 더 관련이 있을 것이다.
본 연구는 몇 가지 한계점이 있다. 첫 번째는 전향적 연구가 아니라 BNP 검사가 시행된 AD나 SVaD 환자를 대상으로 후향적 분석을 시행한 연구라 전향적 분석과는 다른 결과가 나올 수도 있다는 점이다.
두 번째는 BNP 검사가 AD나 SVaD로 입원한 경우에만 시행되어 본 환자군이 전체 환자를 대변한다고 할 수는 없을 것이다. 하지만 두 군의 나이, 교육수준, 혈관성 위험인자, 치매의 정도 등에서 차이가 없었고, BNP를 상승시킬 수 있는 심장질환을 배제기준에서 제외시켰기 때문에 두 군을 비교하기에 큰 문제는 없을 것으로 사료된다. 세 번째는 적은 표본 크기로 향후 대단위 전향적 연구가 필요할 것이다.
결 론
SVaD는 AD보다 혈장 BNP의 증가가 높았다. 이는 SVaD가 혈관성질환에 대한 부하가 더 높음을 시사한다.
참고문헌
1. Cheung BM, Kumana CR. Natriuretic peptides-relevance in cardiac disease. JAMA 1998;280:1983-4.
2. Maeda K, Tsutamoto T, Wada A, Hisanaga T, Kinoshita M. Plasma brain natriuretic peptide as a biochemical marker of high left ventricular end-diastolic pressure in patients with symptomatic left ventricular dysfunction. Am Heart J 1998;135:825-32.
3. Cardarelli R, Lumicao TG Jr. B-type Natriuretic Peptide: A Review of Its Diagnostic, Prognostic, and Therapeutic Monitoring Value in Heart Failure for Primary Care Physicians. J Am Board Fam Pract 2003;16:327-33.
4. Vogels RL, Oosterman JM, van Harten B, Scheltens P, van der Flier WM, Schroeder-Tanka JM, et al. Profile of cognitive impairment in chronic heart failure. J Am Geriatr Soc 2007;55:1764-70.
5. Hoth KF, Poppas A, Moser DJ, Paul RH, Cohen RA. Cardiac dysfunction and cognition in older adults with heart failure.
Cogn Behav Neurol 2008;21:65-72.
6. Isaac DL. Biomarkers in heart failure management. Curr Opin Cardiol 2008;23:127-33.
7. Gunstad J, Poppas A, Smeal S, Paul RH, Tate DF, Jefferson AL, et al. Relation of brain natriuretic peptide levels to cognitive dysfunction in adults >55 years of age with cardiovascular disease. Am J Cardiol 2006;98:538-40.
8. Polidori MC, Mariani E, Mecocci P, Nelles G. Congestive heart failure and Alzheimer's disease. Neurol Res 2006;28:588-94.
9. McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology 1984;34:939-44.
10. Roman GC, Tatemichi TK, Erkinjuntti T, Cummings JL, Masdeu JC, Garcia JH, et al. Vascular dementia: diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop. Neurology 1993;43:250-60.
11. Kang YW, Na DL, Han SH. A Validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients.
J Korean Neurol Assoc 1997;15:300-8.
12. Choi SH, Na DL, Lee BH, Hahm DS, Jeong JH, Jeong Y, et al. The Validity of the Korean Version of Global Deterioration Scale. J Korean Neurol Assoc 2002;20:612-7.
13. Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology 1994;44:1983-4.
14. Choi SH, Na DL, Lee BH, Hahm DS, Jeong JH, Yoon SJ, et al. Estimating the Validity of the Korean Version of Expanded Clinical Dementia Rating (CDR) Scale. J Korean Neurol Assoc 2001;19:585-91.
15. Lee AY. Vascular dementia. Chonnam Med J 2011;47:66-71.
16. Román GC, Erkinjuntti T, Wallin A, Pantoni L, Chui HC. Subcortical ischaemic vascular dementia. Lancet Neurol 2002;1:426-36.
17. Kondziella D, Göthlin M, Fu M, Zetterberg H, Wallin A. B-type natriuretic peptide plasma levels are elevated in subcortical
= 국문요약 =
연구배경: B형 나트륨이뇨펩티드(B-type natriuretic peptide, BNP)는 심실근육의 과도한 신장에 의한 반 응으로 심실의 심근세포에서 분비되며 울혈심부전의 좌심실 기능부전에서 증가된다. 높은 BNP 수치 는 심장혈관질환을 가진 노년에서 인지장애를 예측할 수 있는 인자로도 알려져 있다. 지금까지 치매 에서 BNP에 대한 연구는 적었고, 각 치매 유형에 따른 국내 보고는 없었다. 본 연구는 임상 증상이 유사한 알츠하이머병과 피질하혈관성치매에서 혈장 BNP치를 비교해 보고 BNP와 임상 증상과의 관 계 및 두 질환에서 BNP의 임상적 의미를 알아보고자 하였다.
방법: 인지기능 장애를 주소로 입원한 치매 환자들 중에서 연구 포함기준을 만족하는 알츠하이머병 73명과 피질하혈관성치매 40명을 연구 대상으로 하였다. 환자의 나이, 성별, 교육수준, 고혈압, 당뇨 병, 고지질혈증, 혈장 BNP 수치 등을 조사하였고, 한국판 간이정신상태 검사, 치매단계평가척도, 임상 치매척도를 이용하여 치매의 정도를 평가하였다. 두 군간의 임상지표 및 신경심리검사, 혈장 BNP 농도를 비교하였고, 한국판 간이정신상태 검사와 BNP간의 상관관계를 분석하였다.
결과: 임상지표 및 신경심리검사 결과는 두 군간에 차이가 없었다. BNP 수치는 알츠하이머병 56.5±45.7 pg/mL, 피질하혈관성치매 101.4±225.7 pg/mL로 피질하혈관성치매에서 유의하게 높았다(P=
0.037). 한국판 간이정신상태 검사 점수는 알츠하이머병 2∼27점, 피질하혈관성치매 4∼25점의 분포를 보였고, BNP 수치와 상관관계는 없었다.
결론: 피질하혈관성치매는 알츠하이머병보다 혈장 BNP가 더 증가되었다. 이는 피질하혈관성치매가 혈관성질환에 대한 부하가 더 높음을 시사한다.
중심 단어: 알츠하이머병, 피질하혈관성치매, 나트륨이뇨펩티드 vascular dementia. Neuroreport 2009;20:825-7.
18. Furuta A, Ishii N, Nishihara Y, Horie A. Medullary arteries in aging and dementia. Stroke 1991;22:442-6.
19. Fisher CM. Lacunes: small deep cerebral infarcts. Neurology 1965;15:774-84.
20. Hassan A, Hunt BJ, O'Sullivan M, Parmar K, Bamford JM, Briley D, et al. Markers of endothelial dysfunction in lacunar infarction and ischaemic leukoaraiosis. Brain 2003;126:424-32.
21. De Reuck J, Decoo D, Hasenbroekx MC, Lamont B, Santens P, Goethals P, et al. Acetazolamide vasoreactivity in vascular dementia: a positron emission tomographic study. Eur Neurol 1999;41:31-6.
22. Milward EA, Grayson DA, Creasey H, Janu MR, Brooks WS, Broe GA. Evidence for association of anaemia with vascular dementia.
Neuroreport 1999;10:2377-81.
23. Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, et al. Breathing Not Properly Multinational Study Investigators. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med 2002;347:161-7.
24. Dao Q, Krishnaswamy P, Kazanegra R, Harrison A, Amirnovin R, Lenert L, et al. Utility of B-type natriuretic peptide in the diagnosis of congestive heart failure in an urgent-care setting. J Am Coll Cardiol 2001;37:379-85.
25. Moser D, Cohen R, Clark M, Aloia M, Tate B, Stefanik S, et al. Neuropsychological functioning among cardiac rehabilitation patients. J Cardiopulm Rehabil 1999;19:91-7.
26. de Leeuw F, de Kleine M, Frijns C, Fijnheer R, van Gijn J, Kappelle L. Endothelial cell activation is associated with cerebral white matter lesions in patients with cerebrovascular disease. Ann N Y Acad Sci 2002;977:306-14.